
Abstract
Objective
The coronal ring of patients with unilateral coronal synostosis (UCS) presents premature fusion. This study aims to elucidate whether or not the dynamic behavior of the orbit in response to intracranial pressure (ICP) differs between patients in whom the premature fusion exists only in the frontoparietal suture (FPS) and those in whom the premature fusion extends to the frontosphenoidal suture (FSS).
Methods
A total of 15 UCS patients were included in the present study. Patients in whom premature fusion was seen inside the FPS and those in whom premature fusion extended to the FSS were categorized as FP Only (4.2 ± 1.4 m/o) and FP + FS groups (4.6 ± 2.2 m/o), respectively. On the basis of computed tomography (CT) data, computer-aided design models were produced. Pressure of 15 mm Hg was applied to the neurocranium of each skull model to simulate ICP. Using the finite element method, the displacements presented by each model's orbits were calculated. Displacements of the two groups were compared.
Results
The orbit demonstrated greater displacement in the FP Only group than in the FP + FS group, suggesting that premature closure of the FSS disturbs growth of the orbit in response to ICP.
Conclusion
In performing surgical treatment for UCS, the degree of fusion that the FSS presents should be evaluated carefully. In cases in which the FSS presents premature fusion, it is recommended to release the fusion at an early stage of cranial growth to improve the appearance of the orbital region.
Unilateral coronal synostosis (UCS) is one of the most common congenital deformities of the skull (Mathijssen et al., 2006; Tomlinson and Breidahl, 2007). Although the main symptom of UCS is asymmetry of the frontal region of the skull, UCS frequently is accompanied by deformity of the orbital region. Because the asymmetrical deformity of the orbital region impairs the appearance of patients, it often requires surgical correction (Meara et al., 2003; Hilling et al., 2006; Netherway et al., 2006; Richardson and Thiruchelvam, 2006).
The basic principle of treatment for craniosynostosis is to release the abnormally closed sutures. In patients with UCS, variations are seen in the range over which premature fusion of the coronal ring extends. For some patients, premature fusion is restricted inside the frontoparietal suture (FPS); for others, premature fusion extends to the frontosphenoidal suture (FSS) (Rogers and Mulliken, 2005). To what degree should the coronal suture be released when the whole ring is affected? Is it enough to release only the FPS—which is easily accessible—or should the release be extended to the FSS; although, the FSS is located close to the skull base and is difficult to approach?
To perform effective surgical correction of the orbital asymmetry, it is essential for the clinician to understand the relationship between the range of premature cranial fusion and the resultant orbital asymmetry, given the morphologic origin of UCS and the growth mechanism of the skull in general.
Attempts to clarify the cause of cranial deformity in craniosynostosis date back to the 19th century. After observing the relationship between skull deformity patterns and prematurely fused sutures in craniosynostosis patients, Virchow hypothesized a cause for craniosynostosis (Virchow, 1851/1852). Virchow explained that the development of the cranial vault is disturbed in the direction perpendicular to the fused sutures. On the other hand, compensatory growth occurs in the direction parallel to the fused sutures. Virchow's hypothesis was questioned by Moss because it did not provide a convincing explanation for skull base deformity—another symptom frequently seen in patients with craniosynostosis (Moss, 1959). Moss attributed the cause of the skull deformity in craniosynostosis to an abnormal growth pattern of the skull base. Furthermore, Moss stressed the importance of intracranial pressure (ICP) as a factor affecting the shape of the cranium (Moss, 1975; Delashaw et al., 1989). Enlow stated that when extrinsic forces work on the skull, the skull grows in ways that conform to the forces (Enlow, 1973; Enlow and McNamara, 1973). Further expansion of Enlow's theory allows the assumption that when certain regions of a skull deform in response to mechanical forces, and when the mechanical forces keep working constantly during the skull's growth, the degree of growth that the regions show should correlate with the displacement that the regions temporarily present in response to mechanical forces. Therefore, it can be assumed that the displacement that the orbit temporarily presents in response to ICP correlates with the long-term growth of the orbit. In other words, the potential growth pattern that a skull takes is predictable when one refers to the deformity pattern that the skull temporarily takes in response to ICP.
Given these theoretical backgrounds, the authors set two hypothetical conditions to be used in designing the present study. First, the orbit displaces in response to ICP and grows in the direction of displacement. Second, the degree of the orbit's displacement correlates with the orbit's degree of growth.
Under these two hypothetical conditions, the present study aims to elucidate how the range of premature fusion affects the growth of the orbit in patients with UCS.
In the present study, three-dimensional models are produced to simulate the skulls of patients with UCS. On the inner surfaces of the neurocranium of these skull models, loads are applied to simulate ICP. Then, the displacement of the orbits in response to these loads is calculated using the finite element method. Using the displacement as a parameter that reflects the growth of the orbits, interference with orbital growth by premature closure of the FPS and FSS in patients with UCS is evaluated.
Materials and Methods
Study Samples
Computed tomography (CT) examination was performed for 15 patients with UCS. CT images with 0.5-mm thickness were obtained using CB Works (Hitachi Co., Ibaragi, Japan). Before this experiment was performed, the details were explained to the parents of all 15 patients, and their informed consent for inclusion in the study was obtained. Throughout the study, principles outlined in the Declaration of Helsinki were followed. The 15 patients were categorized into two groups according to the condition of the coronal ring on CT imaging. Patients in whom premature fusion was limited to the frontoparietal suture were categorized as the FP Only group; those in whom premature fusion involved both frontoparietal and frontosphenoidal sutures were categorized as the FP + FS group. The FP Only group consisted of eight patients (4.2 ± 1.4 months old); the FP + FS group consisted of seven patients (4.6 ± 2.2 months old). The age ranges of these two groups did not present statistically significant differences.
Simulation Model Production
A three-dimensional computer-aided design (CAD) model simulating each patient's skull (Nagasao et al., 2006; Nagasao et al., 2007) was produced. First, the CT images of patients were saved as DICOM (Digital Imaging and Communications in Medicine) files at 300 dpi resolution. Then bony components of the images were identified. After the bone data were compiled, a three-dimensional CAD model was produced for each patient. Each model was divided into 188,000 to 248,000 shell elements, each of which contained 30 nodes. Model production and subsequent analysis were performed using structural analysis software (ANSYS11.0, ANSYS Co., Canonsburg, PA).
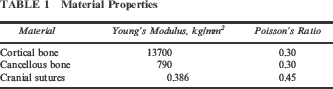
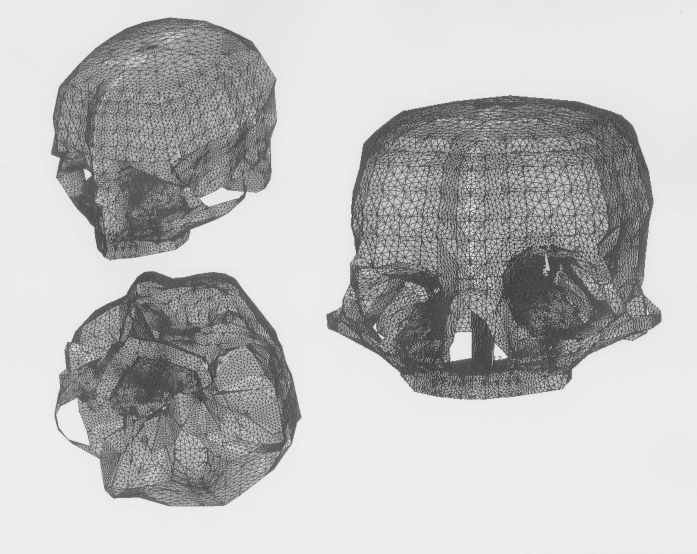
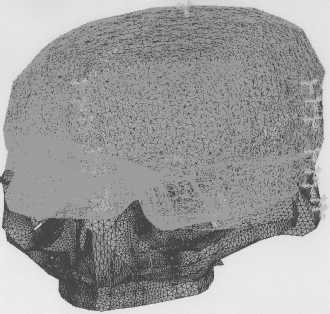
Skull CAD models produced in this manner do not consider the material differences between cranial sutures and bones. Further incorporation of cranial sutures is needed. This incorporation was conducted in the following way. First, with reference to the three-dimensional CT data of the original skulls, patent parts of the cranial sutures were identified by an experienced craniofacial surgeon (T.N.) (Fig. 1A). While the patent sutures were simulated, lines were traced on the corresponding skull models (Fig. 1B and 1C). The material properties of cranial sutures were apportioned to the elements in contact with the traced lines (Fig. 1D); for other elements, the material properties of cortical and cancellous bones presented in Table 1 were apportioned. These material properties were taken from past literature (Pan et al., 2007). Thus, material properties of the components were reflected on each skull CAD model (Fig. 2). For each of the FP Only and FP + FS groups, a representative model is demonstrated in Figure 3.
Modeling process for cranial sutures. Material Properties An example skull model viewed from different angles; material differences between cranial sutures and bone are taken into consideration. Ensuring accurate modeling of cranial sutures by the CAD model: This figure presents samples from the FP Only and FP + FS groups, respectively. In the FP Only group sample (left side), only the frontoparietal suture had closed prematurely; in the FP + FS group sample (right side), both the frontoparietal suture and the frontosphenoidal suture had fused prematurely. Arrows in the figures indicate fused sutures.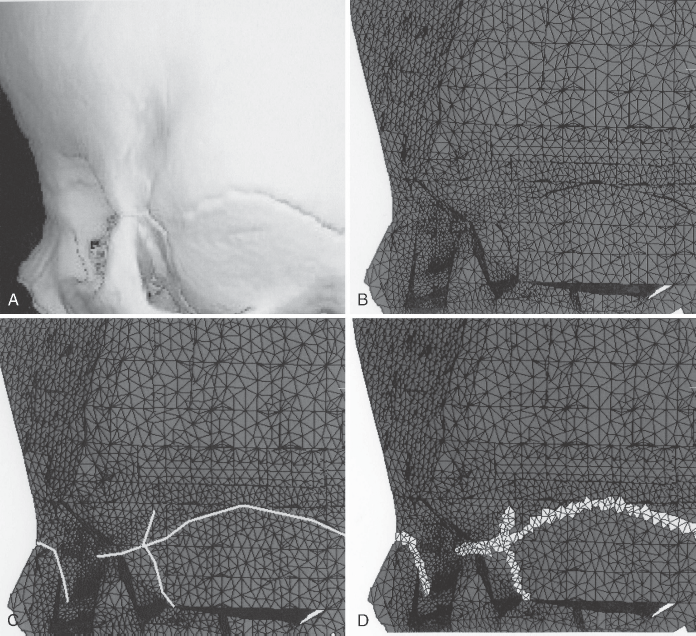
With the assumption that the skulls were fixed at the foramen magnum, zero displacement was given to corresponding areas of the CAD models. Then pressure was applied to the neurocranium of each model, thus simulating ICP.
Whether or not ICP is increased in human patients with UCS remains inconclusive; however, it has been reported that ICP demonstrates no statistically significant difference between rabbits with UCS and control rabbits (Fellows-Mayle et al., 2000, 2004). Under the assumption that this finding is also applicable to human patients with UCS, a pressure within the normal ICP range was loaded onto each model. Because the ICP is normally below 20 mm Hg (Rutigliano et al., 2006), 15 mm Hg of pressure was applied to the inner surfaces of the neurocranium. To each and every element of the inner aspects of the neurocranium (Fig. 4), pressure was applied in the direction normal to each element. Accordingly, this pressure was applied in the superior direction for elements on the cranial vault; pressure was applied in the inferior direction for elements on the skull base (Fig. 5). The displacements that each model's orbits presented in response to loading under these conditions were calculated using the finite element method.
The cranial base of a CAD model is demonstrated. To the internal aspect of the models (shown with double-meshing), 15 mm Hg of pressure was applied to simulate intracranial pressure.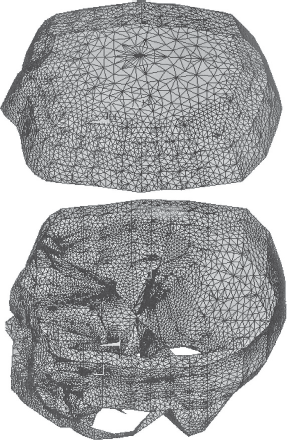
(1) General Transformation
The software used for the analysis is equipped with the ability to demonstrate displacements through the use of color contour maps. These contour maps were compared between the FP Only and FP + FS groups. Thereby, the difference in transformation patterns that the skulls demonstrate in response to ICP was compared between the two groups.
(2) Displacement of Orbital Region
For each model, the following six marking points were set for bilateral orbits (Fig. 6): (1) SOR, the superior orbital rim, (2) MOR, the medial orbital rim, (3) LOR, the lateral orbital rim, (4) SOF, the superior orbital fissure, (5) OC, the orbital canal, and (6) IOR, the inferior orbital rim.
With each model, displacements in response to the intracranial pressure were measured at six measurement points. The six points are demonstrated.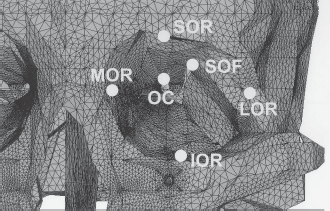
The displacements that these marking points presented in response to ICP were calculated. With each model, displacements of the marking points of the affected side (i.e., the side in which the coronal ring presents premature fusion) were defined as DA (displacement of the affected side); those for the intact side were defined as DI (displacement of the intact side).
As a parameter for quantitative evaluation of the asymmetry that bilateral orbits present, ΔD was defined by the following formula (Fig. 7):
The skull deforms slightly in response to intracranial pressure. The solid lines and the dotted lines indicate the skull shapes before and after application of intracranial pressure, respectively. DA and DI indicate the displacement that a certain point of the skull shows in the deformity. AD, the difference between DA and DI, represents the degree of asymmetry in the deformation.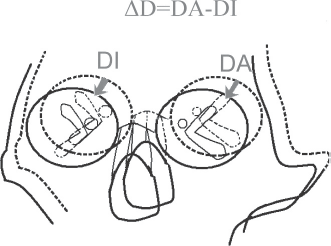

ΔD indicates the relative displacement of a marking point on the affected side against its counterpart of the intact side. When ΔD takes a negative value for a certain marking point, the marking point displaces less on the affected side than its counterpart on the intact side in response to ICP.
The values of ΔD were compared between the FP Only group and the FP + FS group for each of the six marking points. Because ΔD presented a skewed distribution, a nonparametric test (the Mann-Whitney U test) was used for the comparison, p values less than .05 were considered to be statistically significant. All statistical calculations were conducted using the Statistical Package for the Social Sciences (SPSS), version 10 for Windows (SPSS Inc., Chicago, IL).
Results
General Transformation
In both the FP Only group and the FP + FS group, the frontal and orbital regions presented smaller amounts of displacement on the affected side than on the intact side. This finding suggests that expansion in response to ICP is disturbed on the affected side for both groups (Figs. 8 and 9).
The general skull deformity patterns for the FP Only and FP + FS groups are demonstrated. In both groups, the frontal and orbital regions demonstrate smaller displacements in the affected (left) side than in the unaffected (right) side.
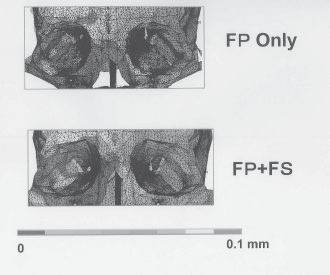
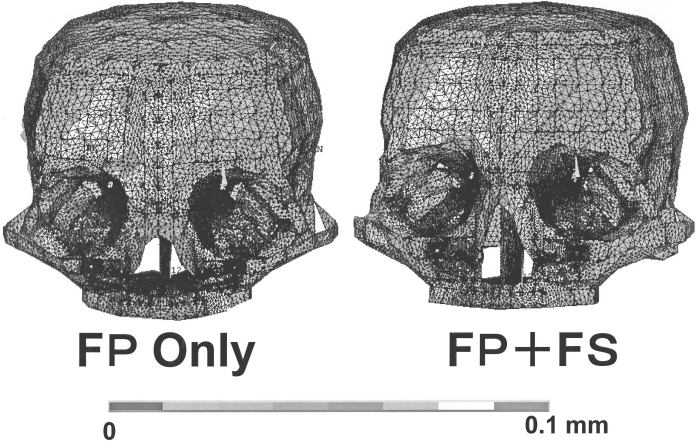
The deformity patterns of the orbital region for the FP Only and FP + FS groups are demonstrated. For the FP Only model, the orbit of the affected side presents less deviation than that of the FP + FS side, indicating that the affected side orbit responds less to ICP in the FP Only models than in the FP + FS models.
Displacement of the Orbital Region
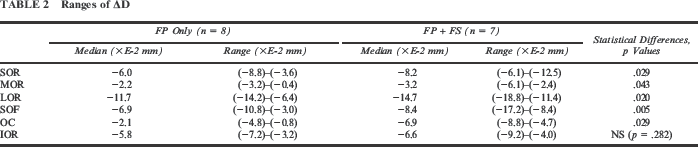
At five (SOR, MOR, LOR, SOF, OC) of the six marking points, ΔD demonstrated smaller values for the FP + FS group than for the FP Only group (Fig. 10; Table 2). This finding indicates that expansion of the affected side orbits is more disturbed for the FP + FS group than for the FP Only group, and that the bilateral orbits tend to present greater asymmetry for the FP + FS group than for the FP Only group.
ΔDs at the measurement points are demonstrated. Displacement differences between the affected and intact sides are greater for the FP + FS group than for the FP Only group, indicating that the effect of the intracranial pressure is disturbed more on the affected side of the FP + FS group than on that of the FP Only group. Ranges of ΔD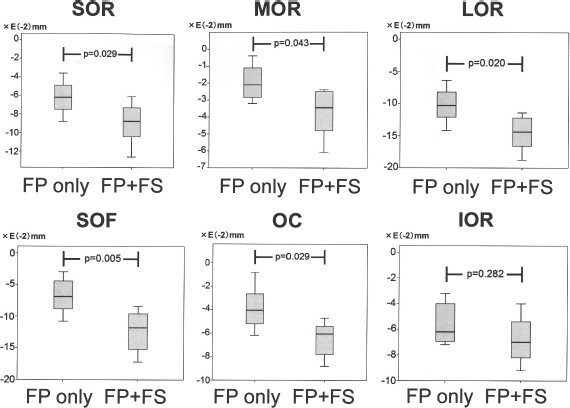
Discussion
Unilateral coronal synostosis is the second most common craniosynostosis (Shillito and Matson, 1968). In patients with UCS, the anterior part of the skull develops asymmetry as the result of premature fusion of the frontoparietal suture (FPS) and/or the frontosphenoidal suture (FSS) (Rogers et al., 2002; de Ribaupierre et al., 2007; Marucci et al., 2009). Asymmetry of the skull also occurs when the lambdoid suture develops premature fusion (Ellenbogen et al., 2000; Komuro et al., 2004). Furthermore, even when no suture presents premature fusion, skull asymmetry can occur in response to asymmetrically applied extrinsic forces (Lee et al., 2008; Liu et al., 2008; McKinney et al., 2008; Spermon et al., 2008). Despite their etiologic differences, these deformities often are categorized within the same genre as “plagiocephaly” because of their symptomatic similarity. However, these three diseases are distinguished from one another on the basis of morphologic patterns that the skull base presents. The skull bases of patients with UCS are characterized by severe asymmetry of the anterior fossa. Accordingly, bilateral orbits present the greatest asymmetry in patients with UCS, often requiring surgical correction. Believing that an etiologic understanding of the cause of the orbital asymmetry is essential in providing effective treatment for patients with UCS, the authors conducted the present study.
The findings of the present study demonstrate that the anterior displacement of affected side orbits is more disturbed in the FP + FS group than in the FP Only group. By referring to this fact and the second hypothesis—that the degree of the orbit's displacement correlates with the orbit's degree of growth—it can be inferred that premature fusion of the FSS aggravates the growth disturbance of affected side orbits, thereby exacerbating bilateral asymmetry of the orbits.
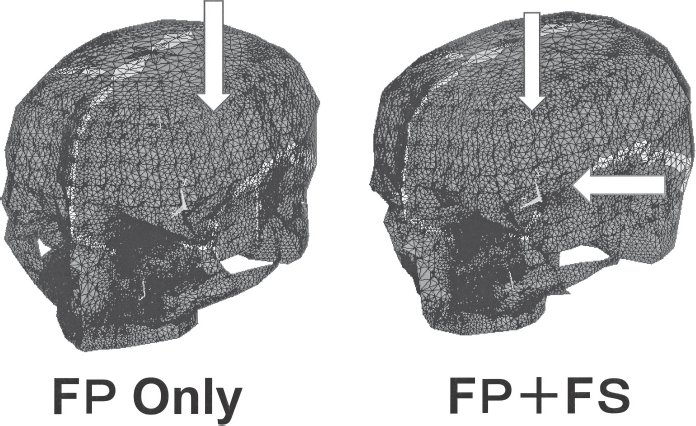
These findings provide guidance for what we should do with prematurely fused FSS. Because premature fusion of the FSS disturbs growth in the orbital region on the affected side and exacerbates asymmetry of the orbits, it is recommended to release the FSS when it is prematurely fused (Fig. 11). Release of the FSS will enhance the effects of subsequent treatments—whether cranial distraction or correction with helmets after the release. The surgical approach to the FSS is often tricky because of its proximity to the skull base. However, the recent development of surgical guideline systems makes the approach to the skull base easier (Piatt et al., 2006). With the help of these systems, prematurely fused FSS should be released to eliminate interference with the biomechanical stimulation of orbital growth by ICP. Thereby, the release of prematurely fused FSS may improve the symmetry of the orbital regions.
For cases in which both frontoparietal and frontosphenoidal sutures present premature fusion, release of only the frontoparietal suture does not provide sufficient treatment effect (left). The frontosphenoidal suture also should be released (arrow on the right).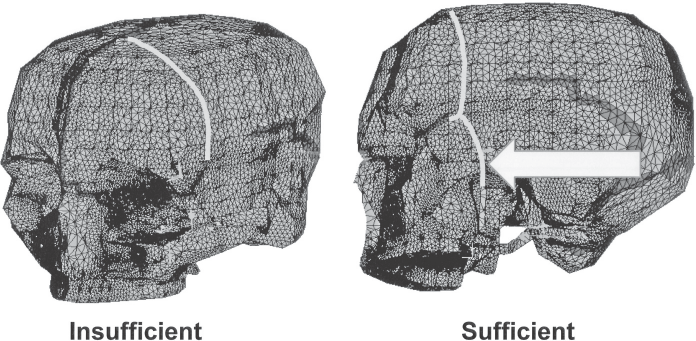
Development of a simulation system that tries to predict the growth pattern of the skull is the novelty of the present study. On the other hand, controversy might be raised regarding some aspects of the present study's simulation system. First, although the authors visually evaluated patency/closure for cranial sutures from patients' CT data, the real extent of patency/closure can be detected at the cellular level only by evaluating osteoblast differentiation and proliferation of osteogenic progenitor cells at the sutures (Sun et al., 2007). However, cellular level evaluation is difficult to perform on actual patients. Therefore, the authors evaluated CT data. Although methodologic validity of the CT-based evaluation has been proved (Sherick et al., 2000; Stadler et al., 2006), the accuracy of the evaluation could be improved further by incorporating other devices, such as ultrasound (Regelsberger et al., 2006). Second, although the present study considers only ICP in the loading, actual conditions are more complex. To improve the reality of the loading conditions, the functions of the muscles attached to the skull and the intrinsic growth potential of the bones also should be considered as loading factors. These factors need to be quantified before they are included in the loads, requiring extensive biomechanical measurement. Furthermore, the validity of these measurement data must be verified by performing retrospective feedback on actual clinical cases. A substantial number of jobs must be performed before the growth pattern of craniosynostotic skulls can be predicted accurately using the simulation system that the authors are now developing.
However, when its practical validity is established through these refinements, the authors' simulation system may become a useful armament in elucidating the morphologic origin and in planning treatment strategies for various types of craniosynostosis. For instance, it has been reported that hypotelorism in patients with trigonocephaly sometimes corrects itself after simple release of the prematurely fused metopic suture, without widening of the interorbital distance by surgical intervention (Marchac and Renier, 1985; Fearon et al., 1996). Whether or not hypotelorism corrects itself would differ among patients, depending on the morphologic individuality of the skull. If a patient's cranial base is thick, with hardened sutures, the orbits are immobilized and are unlikely to move apart in response to ICP. For these patients, surgical intervention should be performed on the bilateral orbits. On the other hand, for patients with a thin skull base and flexible sutures, hypotelorism is expected to correct itself because of the flexibility of the skull base. The difference between these response patterns would be predictable with effective application of our simulation system. When the orbits of the simulated skull present a considerable degree of lateral displacement in response to ICP, hypotelorism in this patient is likely to correct itself. On the other hand, if the orbits present little displacement, the patient will need surgical correction for hypotelorism. Thus, using the present simulation system, the surgeon might be able to plan treatment strategies effectively. The ultimate purpose of the authors' study is to be useful for prediction in such situations through further refinement of the system.
Footnotes
Acknowledgment
Part of the present research was supported by a grant-in-aid for scientific research provided by the Japanese government (Category C: 18500349).