
Abstract
Objective
To explore the role of mental health professionals on craniofacial teams and determine how craniofacial teams assess for psychological concerns in their patient populations.
Design
Online and paper surveys.
Participants
A total of 55 craniofacial team coordinators and 40 mental health professionals who are team members participated in this study.
Results
Results indicated that teams in 2007 generally viewed psychological services on their teams similarly to teams assessed in 1987. Most teams do not use formal measures in their assessment of psychological concerns, and they provide feedback via discussions with the families. Mental health professionals assess a wide variety of potential areas of concern and are generally satisfied with the referral sources available to their patients.
Conclusions
Craniofacial teams appear to practice in a manner consistent with professional standards, and these teams seem to value the inclusion of mental health professionals as part of the interdisciplinary team. Implications and limitations including response rate are discussed.
Interdisciplinary craniofacial teams are composed of a wide variety of health professionals to address the myriad issues that may present for children with craniofacial anomalies (CFAs). Including a psychological assessment as a part of a team evaluation is important in order to address particular concerns of patients and families, evaluate the effectiveness of health care, screen for psychological distress, and assess specific skill areas (Kapp-Simon, 1992).
The American Cleft Palate–Craniofacial Association's (ACPA) Parameters for Evaluation and Treatment of Patients With Cleft Lip/Palate or Other Craniofacial Anomalies (ACPA, 1993), which was most recently revised in 2007, describes recommended practices for team assessment of various areas of concern for patients with CFAs, including psychological and social concerns. Strauss and Broder (1985) described the components of a psychosocial assessment on a craniofacial team (CFT). They noted that clinical interviews inform the clinician of patient psychological concerns and motivation for treatment and can provide information regarding whether further consultations or referrals should be made. Behavioral observations and standardized testing instruments were recommended as supplemental assessment methods. Although these components of psychosocial assessments have been described and recommendations have been made regarding their use, little information is available about how teams actually assess and treat mental health issues in practice.
One study, conducted by Broder and Richman in 1987, surveyed team coordinators via an 11-item postal survey to examine mental health practices on interdisciplinary craniofacial teams. In this study, they found that various psychosocial issues were commonly rated as very important or important to the patient population and that mental health professionals performed a variety of functions on the team, most commonly conducting clinical interviews and taking a family history. Whereas 80% of team coordinators rated mental health services as being very important or important, 20% rated these services as being only somewhat important or not at all important. They also noted that on approximately half of teams, less than 25% of the patients with cleft lip and/or palate were being evaluated by mental health professionals.
Since the Broder and Richman study was published in 1987, there have been a number of changes in health care, including access, funding, and perceptions, that may have altered care for children with CFAs. In addition, there has been increased specialization within professions, particularly in health psychology and pediatric psychology. The present study was designed as a survey of mental health professionals (MHPs) and team coordinators (TCs) on cleft palate/craniofacial teams across the United States. The study aims were to update Broder and Richman's (1987) survey and to describe the current assessment of psychological and social functioning by interdisciplinary craniofacial teams.
Methods
Participants and Procedure
Contact information for the TCs of cleft palate/craniofacial teams in the United States was obtained from the ACPA after obtaining written permission to use its list. This listing included mailing addresses for 224 teams, as well as e-mail addresses for 138 of the teams, including both cleft palate teams and craniofacial teams. Prior to contacting teams, this study was approved by the institutional review board at Saint Louis University.
An initial recruitment e-mail including a link to the study's online survey was sent to all teams for which a contact e-mail address was available. Five of these e-mails were returned as undeliverable. Approximately 1 week later, a paper copy of the survey was mailed to all TCs. Three packets were returned as undeliverable. Team coordinators were asked to complete a portion of the survey (part I) via either hard copy or online and also were asked to pass along the MHP portion of the survey (part II) to the team member who most frequently assesses psychological and social concerns. Two weeks after the initial recruitment e-mail was sent, a follow-up e-mail was sent. All together, 221 teams received copies of the study survey, 133 of which also received e-mail recruitment statements.
Survey Development and Content
One section of the survey was completed by the TC (part I, Appendix A). This section addressed basic information about the respondent and his or her craniofacial team. In addition, this section included the 11 items used by Broder and Richman in their 1987 survey. Questions pertained to the characteristics of the teams (e.g., professions represented), the types of services provided by mental health professionals on teams, the significance of various psychosocial issues to the team's patient population, and the overall importance of mental health services to the team. Items taken from the Broder and Richman survey were presented verbatim, though order of presentation of the items was altered slightly to align with the content of other survey items.
The second section of the survey was completed by the MHP who most often assesses psychological and social functioning as part of the team (part II1). This section included basic information about the respondent and his or her team as well as information about the pragmatics of assessing psychological and social functioning as a part of an interdisciplinary team. Data included the frequency of assessing certain content areas, the constructs that were assessed, and the assessment measures or tools that were used. Most items were presented in a forced-choice format with an “other” option allowing the respondent to generate an alternative answer if necessary. Four questions from the Broder and Richman survey were included in order to compare responses across team roles (i.e., TCs versus MHPs). The 2007 revised edition of the Parameters for the Evaluation and Treatment of Patients With Cleft Lip/Palate or Other Craniofacial Anomalies (ACPA, 1993) was used as a guide in developing questions about the functions of the MHP in working with children with CFAs. Two pediatric psychologists who regularly participate on interdisciplinary craniofacial teams were also consulted to provide practical suggestions for survey items as well as format and methodological advice.
Part II is not included in this article due to survey length but can be provided upon request from the first author.
Data Analysis
Descriptive statistics (i.e., proportions and frequencies) were used to gain an understanding of the survey data. Pearson r correlations and chi-square test for independence analyses were used to explore differences in response patterns to key items by demographic variables.
Results
Response Rate
Fifty-five TCs completed part I of the survey (25% response rate), and 40 mental health and other professionals who assess psychological concerns on the teams (MHPs) completed part II of the survey. Because TCs were asked to pass along survey information to MHPs on their team, it is unclear how many MHPs received the survey; therefore, the actual response rate for MHPs is not known. Response rates were much lower than expected, particularly given the high response rate (70%) achieved by Broder and Richman in their 1987 study. The implications of the response rate found in this study are explored in the discussion. Forty-seven percent of participants responded via the paper version of the survey (45% of TCs and 49% of MHPs).
In order to investigate possible biases in response rate, the proportions of TC responders and nonresponders were compared using data that were available about all teams. The proportion of responders and nonresponders did not differ by geographic region (ACPA sections: Western, Central, Midwest, Southeast, or Northeast; ACPA, 2008) (χ24 = 3.18, p = .53) or by population size of the city in which the team is located (i.e., teams located in one of the 50 largest U.S. cities according to the U.S. Census Bureau [2008] versus teams in smaller cities) (χ21 = .047, p = .83). The TCs who received the survey via both e-mail and postal mail (60% of teams) responded significantly more often than those receiving the survey via postal mail only, with 33% and 11% response rates, respectively (χ21 = 16.64, p < .001). This provides some indication that team characteristics may not have affected whether or not teams responded to the survey, but recruitment factors (e.g., having multiple ways to respond to the survey, multiple reminders about the study) may have played a role in study participation.
Sample Characteristics
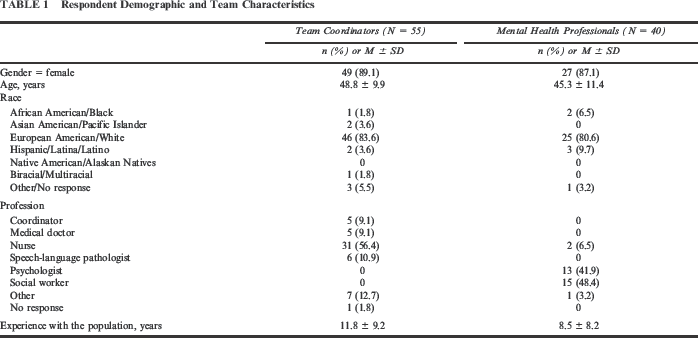
Characteristics of the sample are presented in Table 1. The TCs were most commonly women (89%) and white (83%), with an average age of 49 years. They represented a variety of professions, most commonly nursing (56%). Team coordinators averaged 12 years of experience with the craniofacial population, though the range of experience varied from less than a year to 40 years. Similarly, MHPs were most commonly women (87%) and white (81%), with an average age of 45 years. Social work (48%) and psychology (42%) were the most common professions listed by MHPs. They had an average of 8.5 years of experience with patients with craniofacial anomalies, with a range from less than a year to 30 years.
Respondent Demographic and Team Characteristics
Comparison with Broder and Richman (1987) Survey
Responses by TCs in 1987 and 2007 were similar for many of the items assessing team characteristics and procedures (Table 2). Due to large differences in response rates for the two surveys, statistical comparisons were not conducted. On average, current teams appear to see more patients than those in the past. The majority of patients continue to be younger than age 18, though more teams see adult patients today (57%) than in the past (42%). Although the proportion of nurses, social workers, and psychologists on teams remained consistent, fewer genetic counselors, psychiatrists, researchers, and educators were listed as team members on current teams. Similar to the pattern found by Broder and Richman (1987), TCs reported that MHPs continue to be primarily social workers (49% of teams), followed by psychologists (36%) and nurses (29%). Teams who do not have MHPs as team members frequently have one or more consultants available. Responses to the 2007 survey suggest that consultants are more frequently affiliated with hospitals and less frequently affiliated with private practice work than in the past. Results also indicate that more patients with cleft lip and palate (CLP) or other CFAs are seen by MHPs at team visits now than in the past.
Study Comparisons by Team Characteristics and Procedures
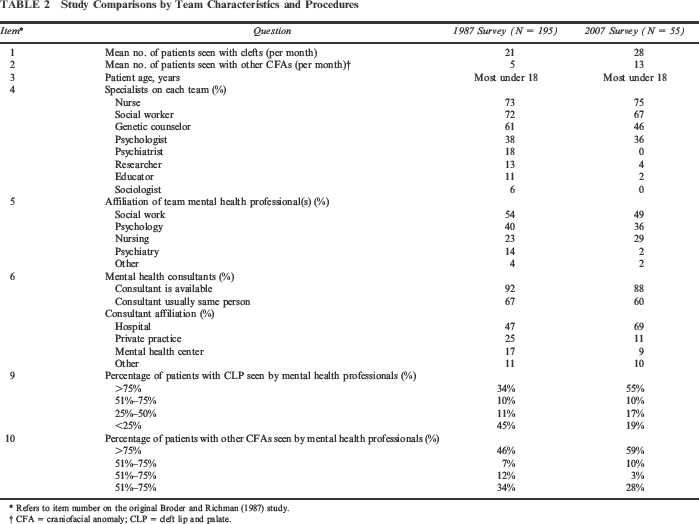
Refers to item number on the original Broder and Richman (1987) study.
CFA = craniofacial anomaly; CLP = cleft lip and palate.
The services provided by MHPs as members of craniofacial teams continue to be primarily clinical interviewing and obtaining a family history. In general, MHPs appear to be providing slightly more varied services today, though patterns between the two surveys were similar in most areas including the conduct of intellectual assessment, personality evaluation, and short-term therapy. Referrals for additional mental health treatment following team assessment are provided more frequently today.
The TCs in 1987 and 2007 responded similarly to an item assessing the TCs' perception of the importance of various psychosocial issues for the team's patient population, with the majority of both groups rating each issue as very important or important (69% to 93% of TCs in 1987 and 63% to 91% of TCs in 2007, depending on the issue).
The final item on Broder and Richman's (1987) survey assessed the TCs' view of the importance of mental health services to the cleft/craniofacial team. Of the TCs, 87% rated mental health services as being very important or important, compared with 80% of teams in 1987. Fewer TCs rated these services as being of little importance or not important at all (4% as compared with 12% in 1987).
Comparison Between TC and MHP Responses
Five items were present in both part I and part II of the survey in order to compare responses between TCs and MHPs.
The majority of MHPs (97%) and TCs (87%) rated assessing mental health concerns as part of a team as important or very important; whereas, 0% of MHPs and 4% of TCs rated it as of little importance or not important at all. Although most MHPs (82%) and TCs (78%) were satisfied with their team's assessment of mental health concerns, 15% of MHPs and 16% of TCs were somewhat dissatisfied or very dissatisfied with their team's assessment process. Mental health professionals tended to rate specific psychosocial issues as being very important or important more frequently than TCs (Table 3), though statistically significant differences in response patterns were found only for the “developmental skills” item (χ21 = 4.39, p < .05), with MHPs rating this domain higher. The majority of both groups found each issue to be very important or important for their patients, with job acceptance (i.e., difficulty becoming employed) being rated the least important psychosocial issue for the patients, possibly because fewer patients in a pertinent age range are seen. Most TCs and MHPs reported that children should be assessed for mental health concerns at every visit, with the second most frequent response for both groups being “during and between visits.” Team coordinators and MHPs indicated that a variety of barriers to effective mental health assessment exist (Table 4). Mental health professionals described specific barriers as occurring less frequently than did TCs, with significant differences in response patterns being found for “lack of patient interest/motivation” (χ22 = 18.20, p < .001) and “lack of parent interest/motivation” (χ22 = 16.30, p < .001). Both groups reported lack of professionals' knowledge/training as being the least frequent barrier to effective assessment.
Perceived Importance of Specific Psychosocial Issues to the Team's Patient Population
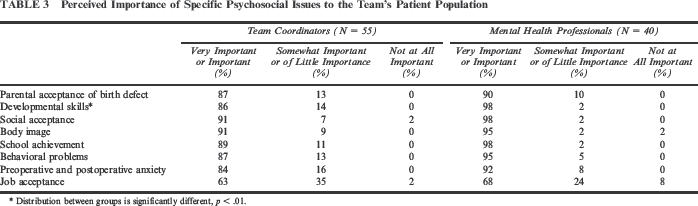
Distribution between groups is significantly different, p < .01.
Frequency of Barriers to Assessment of Mental Health Concerns

Distribution between groups is significantly different, p < .001.
Mental Health Services on Craniofacial Teams
Assessment
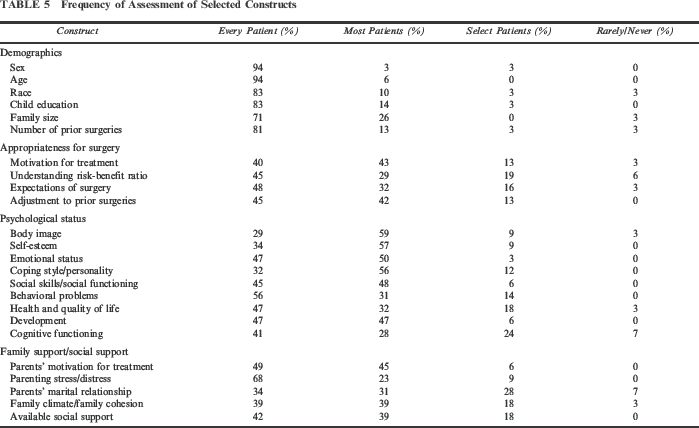
MHPs were asked how frequently they assessed constructs within each of the following categories: demographics, appropriateness for surgery, psychological status, and family/social support (Table 5). Results indicated that demographic variables were assessed for nearly all patients; whereas, appropriateness for surgery was assessed somewhat less routinely. Frequency of assessment of psychological status constructs varied somewhat by construct. For example, whereas emotional status, social skills/functioning, and development were assessed with every patient or most patients by more than 94% of teams, quality of life and cognitive functioning were assessed in select patients only or never assessed on 21% and 31% of teams, respectively. Family support questions similarly varied by construct, with parenting stress and motivation for treatment being more routinely assessed than marital relationship, family climate/cohesion, or available social support.
Frequency of Assessment of Selected Constructs
MHPs were also asked to note the assessment method used for each construct (i.e., interview, questionnaire, or performance-based measure). Results indicated that teams typically assess demographic variables (i.e., sex, age, race, child education, family size, and number of prior surgeries) via interview (approximately 71% of teams), though questionnaires are also regularly used by some teams (approximately 21% of teams). Appropriateness for surgery was almost exclusively assessed via interview, though one to two teams reported using questionnaires. Interviews were also the primary assessment method for psychological status variables (used by 66% to 97% of teams, depending on the construct), though the use of other methods also varied by construct. For example, body image, self-esteem, emotional status, and social skills/functioning were assessed via questionnaire by approximately 24% of teams. Two constructs, development and cognitive functioning, were occasionally assessed via questionnaire (approximately 10% of teams) or performance-based measures (approximately 20% of teams). Coping style/personality, behavioral problems, and quality of life were almost exclusively assessed via interview, though a few teams also reported using questionnaires.
Participants were presented with a list of 53 measures used in clinical settings and in research with children with CFAs as well as room in which to write additional measures. The MHPs were asked to identify measures used clinically by their team and to rate their level of satisfaction with the measure. The most commonly used measures were the Bayley Scales of Infant Development, the Child Behavior Checklist, and the Wechsler Intelligence Scales (Wechsler Preschool and Primary Scale of Intelligence, Wechsler Intelligence Scale for Children, or Wechsler Adult Intelligence Scale), which were each used by 23% of teams (n = 9). Of the remaining measures (including the 14 additional measures identified by participants), 20 were used by two to four teams, and 24 were used by only one team. Of teams, 70% (n = 28) did not endorse using any formal assessment measures.
Information regarding psychological and social functioning is obtained routinely from parents (82% of teams), directly from the patient (77% of teams), and less frequently from teachers (8% of teams), though 75% of teams reported obtaining information from teachers for select patients. Information obtained from parents or patients was often via an interview with a MHP (70% to 72% of teams) and less frequently via standardized measures (20% of teams). When information was obtained from teachers, 22% of teams used an interview, and 24% used standardized measures.
Feedback and Referrals
Feedback regarding psychosocial assessments was provided via a discussion with the family on 88% of teams. More than half of teams reported that they frequently provided feedback via a report sent to the family, though a quarter of teams reported never using this method. Every team endorsed the provision of feedback in some format.
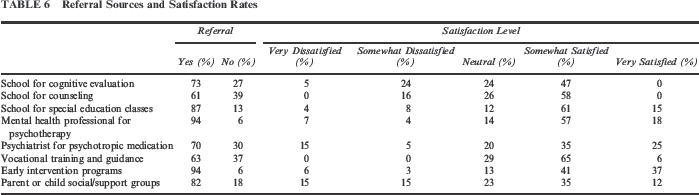
Participants were also asked about referrals that are made following assessment by the team. Results indicated that referrals are not generally given to all patients, and the frequency of referrals tends to increase with age. Specific items addressed the type of referral resources that are given and the MHPs' level of satisfaction with the availability of specific referral resources (Table 6). Referrals to MHPs for psychotherapy and to early intervention programs were the most frequently used; whereas, vocational training and counseling at the child's school were used less often. Participants were generally satisfied with the availability of the referral resources for their patients, though some types of referral resources achieved lower satisfaction ratings. For example, satisfaction with the availability of cognitive evaluations and counseling services at schools, medical treatment by psychiatrists, and parent or child social/support groups each were rated as somewhat or very dissatisfied by 16% to 30% of the respondents.
Referral Sources and Satisfaction Rates
Treatment
Thirty-one percent of MHPs reported that they provide psychological treatment for individuals seen by their team. Of those, 100% provide treatment via individual therapy, 91% provide family therapy, and 36% provide group therapy.
Respondents also were asked how frequently they perform specific functions with patients seen by their team, either through work with their team or in subsequent psychological treatment (Table 7). Results indicated that the most frequently performed functions of MHPs included providing a supportive environment for the child to talk about his or her experience and addressing behavior management issues or teasing. Less frequently performed functions included providing program planning for children with developmental delays, addressing possible rejection by other family members, and providing referrals for vocational training or guidance for adolescents. In general, the functions that MHPs perform were varied.
Frequency With Which Mental Health Professionals Perform Specific Functions on Teams
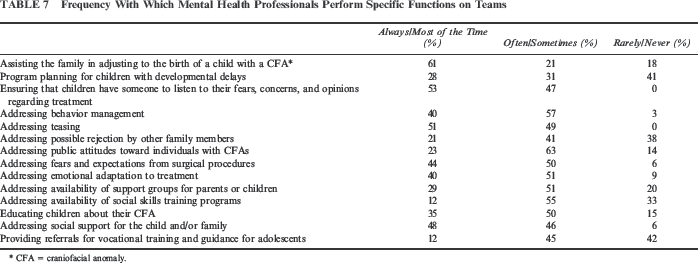
CFA = craniofacial anomaly.
Response Patterns
Responses were analyzed to determine whether they differed by individual respondent demographic or team characteristic variables. The only two characteristics with sufficient variance that were of clinical interest were years of experience working with the craniofacial population and training background.
Years of Experience with the Population
Pearson r correlations were used to determine whether participant responses varied by the number of years of experience working with the cleft/craniofacial population. Ratings of importance of various psychological issues to the patient population varied significantly by experience only on the topic of job acceptance (r = .27, p < .05), in which participants with more experience rated this as a more important issue. Experience level was not significantly associated with ratings of importance of mental health services to the team or importance of assessing mental health services as part of a team. Level of satisfaction with the team's assessment of mental health concerns did vary significantly by experience (r = .25, p < .05), with participants with more experience reporting higher levels of dissatisfaction. Years of experience were not significantly associated with how frequently participants felt mental health concerns should be assessed or ratings of barriers to effective assessment of mental health concerns.
Training Background
Chi-square analyses were used to determine whether participant responses varied significantly by training background, that is, medical (physicians and nurses) versus mental health (psychologists and social workers) training. Results indicated that training background was not significantly associated with participants' responses regarding importance of various psychosocial issues, importance of mental health services to the team, importance of assessing mental health concerns as part of a team, satisfaction with the team's assessment, recommended frequency of assessment, or perceived barriers to effective assessment.
Discussion
Results of the current study indicate that assessment of psychological concerns on interdisciplinary craniofacial teams is a complex process that varies somewhat by team but that has remained fairly consistent over the past few decades. The findings contribute to an understanding of how craniofacial teams are integrating ACPA recommendations for psychosocial care.
Evolution of Mental Health Care on Teams
Overall, surveys completed by TCs in 1987 and 2007 were generally similar, though a few differences emerged. Changes in the composition of teams over the past two decades may reflect expanding roles of team members (e.g., nurses, social workers, or psychologists may be performing some of the duties previously conducted by educators, research assistants, or psychiatrists) or the impact of managed care on the composition of interdisciplinary teams. Consolidation of services within the hospital setting may contribute to the use of consultants affiliated with hospitals rather than in private practice. Increased screening rates among all CLP patients could be due to increased recognition that the degree of facial difference does not determine psychosocial morbidity, and thus, careful consideration of developmental, family, and other child factors is needed for all patients regardless of CFA severity. Referrals for further mental health treatment after the team assessment are more common now, possibly reflecting both the ease of making referrals to hospital-affiliated MHPs and an increased view that mental health services are an important part of adjustment for children with CFAs.
Consistency Across Team Roles
A unique aspect of the methodology used in this survey was the targeting of multiple members of interdisciplinary craniofacial teams as study participants. In this way, items were presented to the team member who was most familiar with the team practices and patient issues, ideally leading to more accurate results.
The TC and MHP ratings were similar for most survey items, though a few interesting differences were found. Greater knowledge of the role of developmental skills in psychosocial functioning may have contributed to MHPs rating developmental skills as being significantly more important to their patient population than TCs did. The fact that 15% to 16% of each group reported some level of dissatisfaction with their team's process for assessment of mental health concerns suggests that there is room for improvement in mental health assessment on some teams. In regard to barriers to the effective assessment of mental health concerns, TCs who often coordinate team visits may have greater knowledge of these barriers than MHPs who see only a subset of patients.
Varied Assessment of Mental Health Concerns on Craniofacial Teams
This study suggests that MHPs routinely address potential psychological and social concerns in a wide variety of areas when conducting a mental health assessment. The less frequent assessment of cognitive functioning may reflect time limitations for conducting a cognitive assessment and/or the presumption that cognitive functioning is assessed in the school setting.
A clinical interview was by far the most common format used to assess various constructs, including quality of life, a topic that has recently gained attention among craniofacial researchers (Patrick et al., 2007). Although MHPs on different teams tended to assess similar construct areas and generally use similar assessment methods, the specific measures (when they are used) varied considerably, and few measures were used consistently across sites/teams. In fact, the most commonly used measures were used by a maximum of 23% of teams, and 70% of MHPs did not report using any questionnaires or performance-based measures in their assessments. The reasons for this low rate of using standard measures is unclear, though possible reasons include lack of finances to purchase measures, lack of time to score and interpret data, low or no reimbursement for testing, or possible concern about the validity of such measures because very few measures have been standardized for use in the craniofacial population. The use of standardized measures of child behavior and functioning can provide normative values against which the child's behavior can be compared. In addition, these measures can minimize the possibility that psychosocial areas of concern may be missed in an interview conducted by a MHP who likely has limited time to interact with the child and family being assessed. Standardized questionnaires may be particularly time efficient and clinically useful because these forms provide a wide array of information on child functioning and often can be completed while the patient and family wait to be seen by the team.
Mental health professionals reported almost always getting information from both parents and children, and it is encouraging to note that 75% of MHPs also reported approaching teachers for information on select patients. Though challenging, the use of multiple reporters is consistent with the systems theories advocated by Engel (1977) to account for the patient's functioning in multiple roles and settings.
Provision of feedback to patients and families highlights the multiple roles often held by the psychologist or other MHP on the team, as described by Nash and Zevon (1992). Not only do MHPs function as behavioral scientists, consultants, and educational resources for the team members, but they can directly benefit the family through their role as a clinician, providing education and support for the family.
Because research suggests that not all children with CFAs experience psychological concerns (Rumsey, 2001; Lockhart, 2003), it makes sense that not all patients are provided with referrals for further mental health treatment/assessment. Referrals may increase with age as children encounter increasing social difficulties or as developmental or cognitive concerns become more apparent. The majority of MHPs reported being satisfied with the availability of referral resources in their communities, yet rates of dissatisfaction were somewhat high for some referral resources, suggesting that potentially beneficial community resources are not always readily accessible. The percentage of respondents (29%) who rated their satisfaction level with the availability of referrals to the school for cognitive evaluation as being dissatisfied or very dissatisfied is particularly disconcerting because respondents also rated cognitive skills as being one of the least commonly assessed areas during team evaluations. In the Parameters… (ACPA, 1993) document, repeated cognitive evaluations are recommended for all children with craniofacial conditions due to the increased rate of learning disorders in this population.
Contributions and Implications
This study provides an update to data reported by Broder and Richman (1987) regarding psychological services offered by interdisciplinary craniofacial teams, indicating that the role and perception of the MHP on craniofacial teams has changed little between 1987 and 2007. Given that the Parameters… (ACPA, 1993) document has been published and revised multiple times since the original survey, each time highlighting the role of mental health services on the craniofacial team, data from these two surveys suggest that MHPs have consistently been an important part of these teams. When differences between the surveys were found, they typically reflected an increased role of mental health services and have been consistent with standards as described in the Parameters… (ACPA, 1993) document.
This study also provided data indicating significant variability in whether and how assessment measures are used, yielding an opportunity for improvement in clinical care and research. Inclusion of standardized measures can provide normative information against which to compare child and family functioning, thereby informing treatment decisions. Additionally, inclusion of standardized measures can promote consistency across teams, facilitating coordination of care for families who relocate and promoting collection of higher quality information on the psychosocial needs of this population, which may guide the future research or treatment guidelines.
Limitations
A primary limitation of this study is the low response rate (25% for TCs). This is less than the average response rate (mean, 49.6% ± 15%) found in a meta-analysis of clinical and counseling psychology postal mail surveys that found a range in response rates of 14% to 91% for surveys from studies published in these fields (Van Horn et al, 2009). It is interesting that a number of studies have indicated that response rates to survey studies have been declining significantly over the past few decades (Van Horn et al., 2009). The response rate found in this study, though not ideal, may reflect this trend or may reflect a lower response rate sometimes found with surveys of medical professionals (24.8%; Del Valle et al., 1997) and surveys seeking information about an organization/team (mean, 35.7% ± 18.8%; Baruch and Holtom, 2008).
Research on response rates for psychology and public opinion studies has indicated that low response rates do not necessarily result in decreased accuracy (Ray, 1987; Curtin et al., 2000; Keeter, 2000; Langer, 2003). In fact, some studies have suggested that lower response rates could be more accurate than higher response rates achieved through multiple-contact recruitment methods (Ray, 1987; Visser et al., 1996) because encouraging higher cooperation could lead to inclusion of respondents who provide nonresponsive answers or by “changing random noncooperation to systematic noncooperation” (Langer, 2003, p. 16).
An analysis of responders and nonresponders on team-based and recruitment-based characteristics in this study failed to find evidence of respondent bias by team region or city size. Receiving the survey via multiple formats appeared to encourage higher participation, which is consistent with other research (Truell, 2003). Although obtaining a high initial response rate would have been preferred in this survey study, these results may be viewed as contributing novel information regarding the role of mental health professionals on craniofacial teams.
Another limitation of this study is that a 5-point Likert format was used for some of the data in order to compare responses between the current survey and that of the Broder and Richman study (1987). This limited response range may have resulted in skewed data and limited the range of data that could be explored via statistical analyses. For example, level of satisfaction with the team's assessment of mental health concerns and importance of mental health assessment to the team may have shown more variability if these items were measured on a scale from 1 to 10. In addition, items often reflected respondent perception and may not reflect actual behaviors on teams.
Areas for Future Research
Evaluating the relative sensitivity and specificity of existing standardized measures for this population is an important next step in furthering clinical research because the use of these measures could save time during the family's visit to the team, streamline the effective assessment of psychological concerns, and provide a means of comparison across sites for clinical and research purposes.
Other interdisciplinary teams also may benefit from the use of a survey study such as this one in order to assess how consensus standards are applied and to identify areas needing possible intervention. As the interdisciplinary team approach is used in more settings to address more medical conditions, continuing to clarify the roles and practices of each team member will be an important goal.
Footnotes
Craniofacial Team Survey – Team Coordinator Version
Gender: ___ Male ___ Female
Age: ___ Years
Ethnicity:
___ African American/Black ___ Asian American/Pacific Islander ___ European American/White ___ Hispanic/Latina/Latino ___ Native American/Alaskan Natives ___ Biracial/Multiracial ___ Other: _____
Profession: _____
How long have you been working with the craniofacial population? ____ Years
What is the setting for your team?
___ Children's hospital ___ General hospital ___ Outpatient setting ___ Other:_____
Which of the following professionals regularly participate on your team?
Medical:
Dental:
Behavioral:
Other:
How frequently are patients scheduled to be seen?
Approximately how many patients with
Approximately how many
does your team evaluate each month? _____
Please circle the percentage of your patient population in each age group:
What is the specific professional affiliation of the mental health professional(s) regularly on your team?
If your team does not have a mental health professional regularly on team, are consultants available?
Is the consultant usually the same person?
What is the consultant's affiliation?
Please indicate (by percentile, %) what type of service is provided by the mental health professional.
___ Interviewing – family history ___ Intellectual assessment ___ Screening developmental skills ___ Personality evaluation ___ Therapy – short term ___ Therapy – long term ___ Support service during hospitalization ___ Research ___ Referral source ___ Learning (achievement) skills ___ Don't know
Please rate the psychological issues of your patient population:
Very important Important Somewhat important Of little importance Not at all important
What percentage of your
What percentage of your
If the above two answers were not 100%, what are the selection criteria for assessment or referral?
___________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
If your team does not have a mental health professional at team regularly, what percentage of children are assessed for psychological concerns by other team members?
Who assesses for psychological concerns in this case?
___________________________________________________________________________________________________
How important are mental health services to your team?
___ Not at all important ___ Of little importance ___ Somewhat important ___ Important ___ Very Important
How important do you feel it is to assess psychological concerns as a part of a craniofacial team?
___ Not at all important ___ Of little importance ___ Somewhat important ___ Important ___ Very Important
How satisfied are you with your team's current assessment and treatment of psychological issues?
___ Very dissatisfied ___ Somewhat dissatisfied ___ Neutral ___ Somewhat satisfied ___ Very Satisfied
How frequently do you feel psychological concerns should be assessed?
___ Every time the patient is seen by the team ___ During and between visits to the team ___ Only when other professionals have expressed concern about the patient ___ Patients should never be assessed for psychological concerns ___ Other:_____
In your opinion, how often is each of the following an important barrier to effective assessment of psychological concerns in children with craniofacial anomalies?