
Abstract
Objective
To assess whether individuals born with nonsyndromic oral clefts display a higher frequency of dental anomalies.
Design
A search of MEDLINE, BIREME, OVID ALL EMB Reviews, and The Cochrane Library was conducted. The methodologic quality of the papers selected was assessed and scored. Papers reporting observational controlled studies of nonsyndromic forms of oral cleft matched for dental anomalies in primary and/or permanent teeth were included without language restrictions. Eligible studies were scored as “A”—low risk of bias, “B”—moderate risk of bias, or “C”—high risk of bias and poor quality. Fixed and random effects models were used to aggregate individual odds ratios (OR) and to derive pooled estimates and 95% confidence intervals.
Results
Six studies fulfilled our selection criteria and were included in the meta-analysis. Three distinct subgroup analyses were carried out in terms of dental anomalies. In the tooth agenesis meta-analysis, a random effects model was used because of heterogeneity and showed a significant association between tooth agenesis and oral clefts (OR = 12.31; 95% confidence interval [CI] = 3.75 to 40.36). In the remaining analyses, the fixed effects model revealed a positive association between supernumerary (OR = 4.99; 95% CI, 2.58 to 9.64) and crown morphologic abnormalities (OR = 5.69; 95% CI, 3.96 to 8.19) with oral clefts. Most included studies were of low to moderate quality.
Conclusion
Although general limitations in study design were observed, the evidence suggests that a higher number of dental anomalies in the permanent dentition are noted in individuals born with oral clefts.
Cleft lip and palate constitutes approximately 65% of malformations affecting the head and neck (Owens et al., 1985). It represents a complex phenotype and reflects a breakdown in the normal mechanisms involved during early embryologic development of the face (Cobourne, 2004). The origin of oral clefts is thought to be multifactorial, with both genetic and environmental factors playing a role (Murray, 2002). The incidence of these defects varies according to geographic location, ethnicity, and socioeconomic status, affecting 1 in every 500 to 1000 births worldwide (Murray, 2002; Cox, 2004).
The occurrence of cleft lip and palate and the development of tooth germs have a close embryologie relationship in terms of timing and anatomic position (Stahl et al., 2006). It is suggested that cleft genes produce disturbances in many body tissues and therefore also affect the dental lamina (Johnson, 1967). It has been reported that individuals born with clefts have a higher incidence of abnormal crown morphology, hypodontia, supernumerary teeth, and taurodontism (Schroeder and Green, 1975; Poyry and Ranta, 1985; Dahllof et al., 1989; Shapira et al., 2000; Dewinter et al., 2003; Ribeiro et al., 2003; Letra et al., 2007; Menezes and Vieira, 2008; Küchler et al., 2010). In addition, previous reports have related higher frequencies of dental anomalies as the severity of the cleft increases (Eerens et al., 2001; Slayton et al., 2003; Aizenbud et al., 2005). Studies have indicated that dental anomalies may represent an additional clinical marker for oral clefts, suggesting that isolated cleft lip and palate can be subphenotyped on the basis of dental development (Letra et al., 2007; Menezes and Vieira, 2008).
More recent studies confirm the evidence that common genetic factors may contribute to both oral clefts and dental anomalies (van den Boogaard et al., 2000; Slayton et al., 2003; Vieira, 2003; Vieira et al., 2008). It is well documented that teeth close to the cleft are likely to have malformations or to be missing (Ranta, 1986; Rawashdeh and Abu Sirdaneh, 2009). Less information is available regarding dental anomalies outside the cleft area. The aim of this study was to undertake a systematic review and meta-analysis to assess the evidence that individuals with isolated oral clefts may display higher frequencies of dental anomalies.
Materials and Methods
Search Strategy
Publications of potential relevance to our study were identified by using both exploded MeSH headings and text words in a search of MEDLINE (1966–2009), BIREME (1967–2009), OVID ALL EMB Reviews (1950–2009), and The Cochrane Library. In these databases, the terms were “cleft lip” [MeSH terms] OR “cleft palate” [MeSH terms] OR “cleft lip and/or palate” [tw] OR “oral clefts” [tw] AND “dental anomalies” [tw] OR “tooth abnormalities” [MeSH terms] OR “anodontia” [MeSH terms] OR “agenesis” [MeSH terms] OR “tooth, supernumerary” [MeSH terms] OR “microdontia” [tw] OR “tooth malposition” [tw] OR “tooth, impacted” [MeSH terms] OR “tooth malformation” [tw] OR “tooth transposition” [tw] OR “tooth rotation” [tw] OR “taurodontism” [tw]. Additional articles of potential relevance were identified by manual searches. Observational controlled study designs composed of nonsyndromic forms of oral clefts matched for dental anomalies in primary and/or permanent teeth were included without language restrictions.
Textbooks, dissertations, case reports, case series, review articles, and abstracts were excluded. Two examiners (P.N.T. and C.A.G.R.O.) independently screened each paper by examining the title, abstract, and keywords. If examiners had diverging opinions, the papers were re-examined until a consensus was reached. If relevant data were missing, the authors of the papers in question were contacted for additional information.
Quality Assessment of Studies
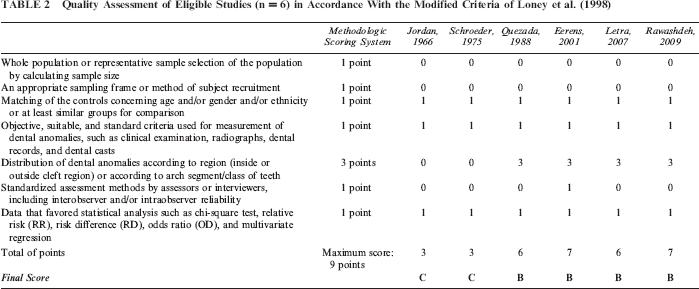
We performed a quality assessment of the remaining studies to control for influence bias, to gain insight into potential comparisons, and to guide interpretation of findings (Higgins and Green, 2005). Selected articles were assessed in accordance with the modified criteria of Loney et al. (1998). Seven criteria were analyzed, and a methodologic scoring system was used to rate the quality of the papers. The authors recommended weights for each item for the scoring system. Thus six criteria were assigned a score of 1 point. Only one was assigned a score of 3 points because it evaluated the distribution of dental anomalies according to the region or according to the arch segment/class of teeth, making 9 the maximum score possible.
After this, researchers classified the studies into three categories with scores “A” to “C” according to predetermined criteria for method and performance. To obtain score “A,” low risk of bias, the study should present 8 to 9 points in the methodologic scoring system; to obtain score “B,” moderate risk of bias, the study should present 5 to 7 points; and to obtain score “C,” high risk of bias and poor quality, it should present 1 to 4 points. Studies assigned the higher scores (“A” and “B”) were weighed more heavily when the meta-analysis was performed.
Meta-analysis
The meta-analysis was performed by the software Rev-Man, version 5.0, provided by The Cochrane Collaboration (http://ims.cochrane.org/revman/download). The OR was used as a measure of effect with its 95% CI between oral cleft and risk of dental anomalies. Heterogeneity between studies was assessed using a standard chi-square test. If homogeneity existed among the studies (p ≥ .10), the fixed effects model (Peto method) was applied to aggregate the data. If homogeneity was rejected (p < .10), a random effects model (M-H method) was the option.
Results
Search queries retrieved a total of 505 papers: 253 references from MEDLINE, 203 references from the BIREME database, 34 articles from the OVID ALL EMB Reviews database, and 15 papers from The Cochrane Library database. Seventeen studies appearing in two database searches were considered only once. Studies were excluded from this review for two reasons (Fig. 1). Most of the excluded studies (n = 480) did not include frequency data for clefts and dental anomalies and were not observational and controlled in design. Two studies that included individuals with oral clefts and additional structural abnormalities or defined syndromes (Dahllof et al., 1989; Budai et al., 2001) were excluded. Eight studies were analyzed and are displayed in Table 1. A total of six studies fulfilled all criteria and were carefully read and ranked as shown in Table 2. Four studies selected for final assessment were graded with the score “B,” and the other two were graded with the score “C.”
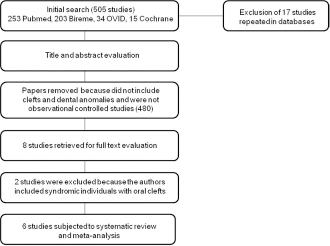
Diagram of literature search and selection process.
Overview of the Eight Case-Control Papers Analyzed
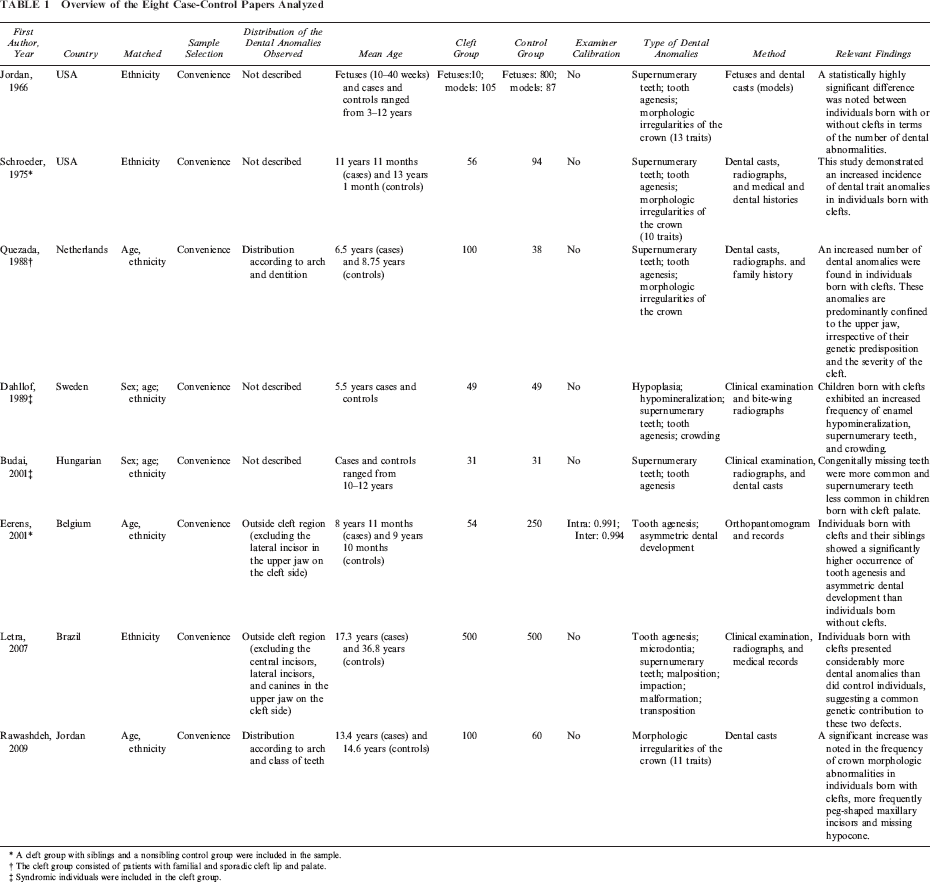
A cleft group with siblings and a nonsibling control group were included in the sample.
The cleft group consisted of patients with familial and sporadic cleft lip and palate.
Syndromic individuals were included in the cleft group.
Quality Assessment of Eligible Studies (n = 6) in Accordance With the Modified Criteria of Loney et al. (1998)
The six eligible studies were selected for the meta-analysis. Three distinct subgroup analyses were carried out in terms of dental anomalies. For tooth agenesis, data from Jordan et al. (1966), Schroeder and Green (1975), Quezada et al. (1988), Eerens et al. (2001), and Letra et al. (2007) were included. For supernumerary teeth, data from Jordan et al. (1966), Schroeder and Green (1975), and Letra et al. (2007) were included. For morphologic irregularities of the crown, data from Jordan et al. (1966), Schroeder and Green (1975), Letra et al. (2007), and Rawashdeh and Abu Sirdaneh (2009) were included. Because Rawashdeh and Abu Sirdaneh (2009) reported data by total number of teeth, we estimated the number of individuals affected for inclusion in the meta-analysis. The frequency of morphologic irregularities of the crown was estimated, on the basis of data from Jordan et al. (1966), Schroeder and Green (1975), and Letra et al. (2007), as 10.0% for the control group (n = 6). The cleft group presented approximately a seven times greater chance to be affected, based on the number of affected teeth reported by Rawashdeh and Abu Sirdaneh (2009); we estimated that 42 individuals born with clefts had morphologic irregularities of the crown. Only one study (Quezada et al., 1988) reported separate results by dentition (permanent or primary), but no data were available regarding the primary dentition in any other studies, and only data on the permanent dentition were included in the analysis.
Heterogeneity tests showed that heterogeneity existed in the included studies for assessment of tooth agenesis (p < .0001), and a random effect was used. The same test for heterogeneity did not give a significant result (p > .10) for supernumerary teeth and morphologic irregularities of the crown; a fixed effects model was therefore used.
In the tooth agenesis subgroup, a significant association between clefts and tooth agenesis (OR = 12.31; 95% CI, 3.75 to 40.36) (Fig. 2) was found. The remaining analyses showed an association between clefts and supernumerary teeth (OR = 4.99; 95% CI, 2.58 to 9.64) (Fig. 3) and morphologic irregularities of the crown (OR = 5.69; 95% CI, 3.96 to 8.19) (Fig. 4).
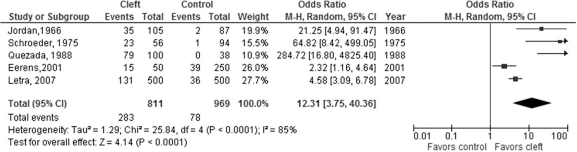
Forest plot between cleft and control groups showing the prevalence of tooth agenesis.
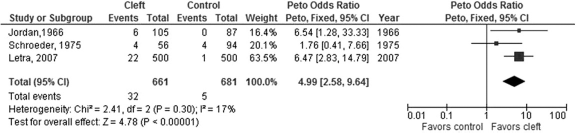
Forest plot between cleft and control groups showing the prevalence of supernumerary teeth.
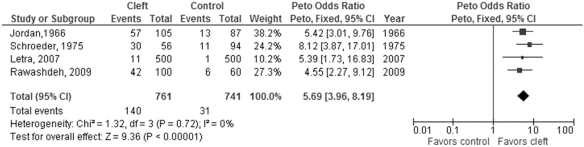
Forest plot between cleft and control groups showing the prevalence of morphologic irregularities of the crown.
Additionally, we performed a sensitivity analysis by removing data to evaluate the influence of individual studies. Heterogeneity in the tooth agenesis analysis was not resolved by excluding any individual study. Nevertheless, upon exclusion of a specific study (Quezada et al., 1988), a smaller confidence interval was observed (OR = 7.54; 95% CI, 2.71 to 20.99). The summary odds ratio was not significantly changed.
Discussion
Comparison of outcomes from prevalence studies conducted in different populations may allow inferences to be drawn about the association between a certain disease and its possible associated factors. These significant inferences should be drawn from high-quality prevalence research. We incorporated existing published criteria on disease prevalence (Loney et al., 1998) and developed critical appraisal criteria to estimate the prevalence of dental anomalies in a definite population (Table 1).
The most striking finding when this systematic review was conducted was the high number of papers that were excluded because of lack of a control group. Moreover, a majority of publications did not analyze separately anomalies inside and outside the cleft region. Given that the cleft region has a bone defect, teeth close to the cleft are commonly malformed or missing (Ranta, 1986; Rawashdeh and Abu Sirdaneh, 2009). For this reason, we decided to attribute higher scores to studies in which authors presented data on dental anomalies by tooth type, arch affected, or location inside versus outside the cleft region. Nevertheless, we are conscious that our meta-analysis presented particular challenges because of differences in study design. Combining data on dental anomalies in the cleft region with those outside the cleft region resulted in the risk of depriving representation of some studies. To reduce potential bias, we carried out three specific subgroup meta-analyses of only relevant and appropriate data. Moreover, to investigate the individual contribution of each study to heterogeneity, we excluded each study from the analysis consecutively and observed only small effects on the results.
Of the eight case-control studies previously selected, two were excluded because of the presence of syndromic patients (Dahllof et al., 1989; Budai et al., 2001). Of a total of six eligible studies, four were considered to have moderate risk of bias (Quezada et al., 1988; Eerens et al., 2001; Letra et al., 2007; Rawashdeh and Abu Sirdaneh, 2009), and two were classified as having a high risk of bias (Jordan et al., 1966; Shroeder and Green, 1975). Also, when these six studies were considered, it was noted that in four of them, the authors showed results according to the region of anomalies or tooth/arch affected.
Quezada et al. (1988) presented the results according to the arch affected in the permanent dentition. The authors concluded that dental anomalies are predominantly confined to the upper jaw of cleft lip and palate patients, indicating a relationship between cleft formation and formation of the teeth. On the other hand, Eerens et al. (2001) reported that just dental anomalies outside the cleft region were observed, but the authors excluded only the lateral incisor in the upper jaw on the cleft side. Letra et al. (2007) did not include dental anomalies inside the cleft region (affecting maxillary central incisors, lateral incisors, or canines), because the absence of such teeth was likely the consequence of developmental anomalies at the cleft side. Rawashdeh and Abu Sirdaneh (2009) showed results according to arch and class of teeth.
In terms of the quality of eligible studies, several points deserve emphasis. The design of the selected studies did not include sample size calculations or a representative sampling of the population. Most studies were conducted in dental schools, and samples of “convenience” were obtained in these cases. With respect to matching cases and controls, most studies (n = 5) were considered satisfactory because cases and controls were matched for age and ethnicity. Despite the fact that one of these studies (Letra et al., 2007) did not match age in the two groups, it involved a large sample of 1000 participants, and significant differences were observed in the frequency of tooth agenesis, microdontia, supernumerary teeth, tooth malposition, impaction, and multiple dental anomalies between individuals with cleft status and control individuals. The other eligible studies had more modest sample sizes. Critical appraisal of the published data, evaluating the sample size required to answer the research question, is an important step in interpreting the relevance of these results (Noordzij et al., 2010). A large sample size produces narrow confidence limits; this is undoubtedly important if the prevalence or incidence of a given condition is low. Small sample sizes produce large confidence intervals, making the findings less precise (Loney et al., 1998). Despite the limited number of cleft children, the results of Eerens et al. (2001), for example, revealed that the cleft group showed significantly more hypodontia when compared with the nonsibling control group.
Quezada et al. (1988) evaluated morphologic dental anomalies, hypodontia, and supernumerary teeth in patients with and without cleft lip and palate. Family history, dental casts, and radiographs were studied. Based on the occurrence of cleft lip and palate in the family, a distinction was made between familial and sporadic cleft lip and palate. Hypodontia was the only dental trait observed through radiographs/records and compared between cleft and control groups in the study by Eerens et al. (2001). In this study, the term hypodontia was used to indicate one or more missing teeth. Letra et al. (2007) observed the frequency of tooth agenesis, microdontia, supernumerary teeth, malposition, impaction, malformation, transposition, and the combination of more than one dental anomaly, and compared their frequency in healthy individuals and in individuals born with a cleft. Clinical examination, radiographs, and medical records were used as assessment methods. The term agenesis was used to mean hypodontia and oligodontia. Radiographs including orthopantomograms were used in three studies ranked with a score of “B” (Quezada et al., 1988; Eerens et al., 2001; Letra et al., 2007). Intraexaminer reproducibility was reported only in the study by Eerens et al. (2001). Letra et al. (2007) had only one examiner. On the other hand, Rawashdeh and Abu Sirdaneh (2009) identified crown morphologic abnormalities only by dental casts.
Letra et al. (2007) reported that children 8 years of age or younger were excluded from the analysis, mainly because sometimes premolar tooth buds are not visible on radiographs at younger ages. Third molars, which are the teeth most frequently absent in all populations (Graber, 1978; Larmour et al., 2005), were not included in the evaluation of tooth agenesis because of the age range of study participants. Eerens et al. (2001) considered congenially missing teeth if they were absent on the radiograph. However, the mean age of cleft and control groups was between 8 and 10 years. The definition of second premolar agenesis may have introduced bias. On the other hand, the authors did not report whether third molars were excluded, but we believe that these teeth were not evaluated because investigators included young children in both groups.
Conclusion
In summary, in spite of the limitations of studies available in the literature, evidence suggests that individuals born with clefts have more dental anomalies in the permanent dentition than unaffected individuals. This meta-analysis has highlighted the need for more carefully designed studies to analyze individuals with oral cleft with regard to the presence of dental anomalies and possible common causes.
Footnotes
Acknowledgments.
We thank CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior) for financial support.