
Abstract
Objective
A gene bank, comprising genetic material and environmental and family history data, is being established in the United Kingdom to improve the understanding of the etiology of orofacial clefting (OFC). This study aimed to identify factors that might contribute to participation in a cleft gene bank and what issues need to be considered in approaching parents to be included.
Design
A qualitative approach was adopted, using focus groups and interviews. Transcripts of audio recordings were analyzed using inductive thematic analysis.
Participants
A UK cleft center invited 100 families of children born with OFC to participate. Inclusion criteria included any parent of a child aged between 6 months and 16 years willing to take part. Sixteen parents participated.
Results
Participants were generally motivated to take part in a cleft gene bank because they value the discovery of new knowledge of the etiology of OFC. They wanted reassurance about the purpose and integrity of the project. Many conveyed shock at the diagnosis of cleft and offered mixed accounts of experiences with health care professionals. They suggested an individualized approach from a trustworthy and sensitive professional when being invited to join the gene bank, avoiding difficult times associated with new-baby challenges and issues related to the cleft.
Conclusions
This pilot study indicates that parents of children born with OFC would be supportive of developing a cleft gene bank, but sensitive issues need to be considered.
Some form of orofacial clefting (OFC) is seen in about 1 in 700 live births worldwide (Mossey and Castilla, 2003). The birth of a child with a cleft evokes a range of parental reactions including guilt, shock, and avoidance (Dolger-Hafner et al., 1997). A child born with a cleft will be treated by a multidisciplinary team and will undergo a number of surgical episodes with potential psychosocial and health implications. In the postnatal period, the family might have concerns about feeding as well as the prospect and outcomes of surgery (Kuttenberger et al., 2010). Physical signs such as scarring and altered speech may have a lifelong impact on both child and family (Strauss et al., 1988). Although the majority of individuals do not experience major psychosocial problems, behavioral problems, depression, and/or anxiety are associated with cleft in childhood (Hunt et al., 2005). It is known that males who are born with cleft palate demonstrate a lower general intellectual capacity than noncleft controls do (Persson et al., 2008). People with cleft generally experience a shorter lifespan and increased risk of mortality from all causes (Christensen et al., 2004). Orofacial clefting clearly affects the individual, their families, and society. There is a need to increase our understanding of the causes of this condition.
Plans for a U.K. Gene Bank
Orofacial clefting has a multifactorial etiology (Cobourne, 2004) with influence from genetic and environmental factors, but many aspects, including complex gene-environment interactions and pathogenesis, are not yet fully understood. Large multicenter studies are required to assess the connection between and influence of genetic and environmental factors (Mossey et al., 2009). There are now plans to establish a gene bank for orofacial clefts in the United Kingdom (The Healing Foundation, Cleft Lip and Palate Research Programme, 2008). This resource will include genetic material (blood/cell lines), family and environmental histories, and demographic data from several thousand children and their parents. Questionnaires surveying background demographic details, family histories, and environmental exposures will be used at the earliest opportunity in an attempt to reduce recall bias (Kallen, 2005).
Ethical Issues in Genetic Research
Ethical considerations exist for any genetic research study (Shickle, 2006), but the particular issues concerning recruitment of participants to a large-scale cleft research program are as yet unknown. For some parents and societal groups, research aimed at preventing this condition may seem inappropriate. The Cleft\ Lip\ and\ Palate\ Association(CLAPA; 2009) and research leaders in this field have raised potential concerns about the establishment of a gene bank for cleft, despite perceived benefits. These concerns include the possibility that the discovery of the cause of clefting may result in a reduced diversity in appearance through the eradication of clefts or through eugenics. Many of those born with a cleft adjust well and can accommodate the associated challenges (Patel and Ross, 2003); some would argue that the cleft is an essential part of their own identity. The rationale of the cleft gene bank being to prevent clefts in the future might therefore be met with mixed feelings. It is important then to explore the opinions of those born with a cleft and their families in the planning of such a facility.
Current Evidence from other Studies
Neonatal Research
Parents will consider participating in neonatal research to investigate congenital conditions if the potential benefits to individuals and society are clear (Hoehn et al., 2005). Informed consent for inclusion in neonatal research is improved through antenatal awareness of research, discussion with parents, clear information, and appropriate training for the approaching clinician (McKechnie and Gill, 2006). Moreover, the timing of an approach for inclusion in neonatal clinical trials and the environment in which this is undertaken are two important factors to be considered to maximize participation and ensure that participants do not feel coerced to take part (McKechnie and Gill, 2006).
Demographic and Background Differences
There is little qualitative evidence on the influence that background factors may have on participation in a gene bank for cleft. Demographic differences, including the age and educational attainment of parents, have been found between participants and nonparticipants (Romitti et al., 1998). Recruitment rates in other types of genetic birth disorder research vary between different ethnic groups (Crider et al., 2006). A difference in cultural beliefs on the causes of diseases and attitudes to research involvement may account for differences in participation rates. There are also religious explanations for clefting (Olasoji et al., 2007; Oginni et al., 2010), and these may contribute to differences in participation in cleft research. Being African American (versus Caucasian) is a known predictor for concerns about the use of samples from pediatric biobanks (Goldenberg et al., 2009).
Participation in Biobanks
Participants in the U.K. cleft gene bank may be asked to provide additional data over time, and factors that influence long-term participation will be important. Longitudinal cohort studies such as the Avon Longitudinal Study of Parents and Children have successfully maintained good follow-up rates (Golding et al., 2001). Some cleft cohorts, for example, the Eurocleft study, have established high rates of continued involvement; of the 123 patients with unilateral cleft lip and palate (CLP) whose cleft care outcomes were studied at age 9 years, only three were not present in the study at age 17 years (Moisted et al., 2005). Further work is required to understand what motivates people with cleft to participate in long-term research.
There are important differences between population biobanks and disease-specific biobanks (Gurwitz et al., 2009). These different types of biobanks may require variations in regulation and statute specific to the individual biobank (Gibbons, 2009). There are approximately 107 cord blood banks worldwide (Serrano-Delgado et al., 2009). Ethical issues related to the storage and use of such material as well as participation rates have been explored but not yet in relation to OFC. Public opinion of biobanks that include children have identified some themes such as the importance of obtaining a child's permission to take part, risks versus benefits in participating, and the need to return information to the study participants (Kaufman et al., 2008). It is possible that similar themes may be seen in a group of parents of children born with OFC.
Study Aims
A workshop to discuss a future U.K. gene bank for OFC was held in 2007. A consensus view was formed. Issues surrounding the approach of potential participants should be investigated, and their views on such a method of research should be sought. As a result of this meeting, and in response to the lack of existing evidence to best inform the establishment of a cleft gene bank in the United Kingdom, a project was undertaken as a pilot study. A qualitative approach was used because of the exploratory nature of the research and the need to understand the perspectives and experiences of participants. The aims of the study were to investigate (1) what might motivate parents of children born with CLP to take part in a research program involving a gene bank and (2) parental preferences on how they should be approached for inclusion in a cleft biobank.
Methods
Recruitment
Recruitment of participants was purposive; we approached parents of children born with a cleft as representatives of the group likely to be approached for a cleft gene bank. Their children were aged at least 6 months, whereby they would have experienced at least one surgical episode and would therefore be able to comment on both the time when they received the diagnosis and the experience of their child undergoing surgery. Families' contact details were obtained from a database in a U.K. cleft center. One hundred families in the database were identified as eligible; the inclusion and exclusion criteria are shown in Table 1.
Inclusion and Exclusion Criteria

An invitation letter was sent to these parents together with a supportive introductory letter from the director of the center. If the parent agreed to participate, a further information sheet for the study was sent together with a consent form. When parents returned consent forms, they were contacted by telephone, and an appointment was made to attend a focus group. Focus groups were used to provide a supportive atmosphere and to capitalize on group interactions to generate data (Sim, 1998).
Ethics
The study was reviewed and approved by the Local Research Ethics Committee. The focus group facilitators outlined the importance of the confidentiality of focus group discussions to participants. All personal information was removed during transcription; names were replaced by initials, and all other identifiers (e.g., names of cleft center staff) were anonymized.
Research Procedure
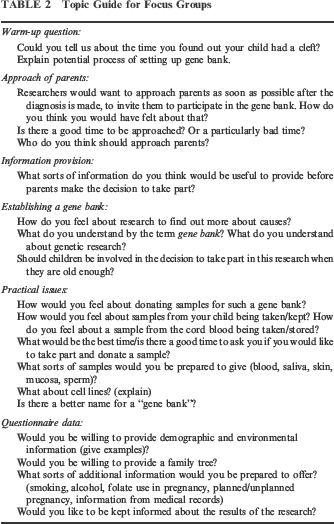
A topic guide was developed by three of the research team members on the basis of existing research (as discussed above) and the processes involved in the establishment of the proposed gene bank (Table 2). Four of the five focus groups were held in a counseling suite on a British university campus. The fifth group was held at the home of a participant because of access issues. One group had only one attendee; this was considered as an interview with data analyzed in the same way as the focus groups. The groups were led by L.W. and co-facilitated by a psychologist experienced in the running of focus groups. Neither of the facilitators was directly connected with the gene bank for cleft, nor were they involved in the clinical care of the children of the participants. The latter provided demographic details, family history, and information about their child's diagnosis before the groups started. Subsequently, they were invited to discuss their experiences regarding the diagnosis of the cleft. L.W. then gave a brief description of the anticipated processes involved in the construction of a cleft gene bank, supported with a visual aid in the form of a poster. This process created openness about the agenda, allowed participants to understand the questions that would be addressed, and provided a common framework for discussion in different groups. The topic guide was used for each group and was delivered through the use of open questions and supplementary questions as appropriate. Focus group data were transcribed verbatim by a freelance secretary who signed a confidentiality form. The transcripts were checked by L.W. against the recordings before analysis began. They were imported into NVivo8 (QSR International, Southport, U.K.), a computer program designed to facilitate management of the data. Analysis of group transcripts was not undertaken until all five groups had been completed.
Topic Guide for Focus Groups
Analysis
Inductive thematic analysis methods were used (Attride-Stirling, 2001; Braun and Clarke, 2006), grounding the results in the data and allowing the analysis to be data driven (Braun and Clarke, 2006). This approach was taken because of the lack of a priori themes in the literature extant related to the approach of potential participants to a cleft gene bank. L.W. undertook the primary analysis; sections of text relevant to the research questions were named and coded into basic themes (Rabiee, 2004). Coding was refined as the analysis progressed (Silverman, 2007); the codes were checked for overlap and repetition. From these data, related basic themes were grouped together to form a smaller number of organizing themes (Attride-Stirling, 2001). Sections of data that were not placed within these themes were subsequently rechecked to see if they provided strong evidence for additional themes or contained contrasting evidence.
A second researcher (E.D.), not present at the focus groups and interview, analyzed the transcribed data separately with no prior knowledge of the research questions but with knowledge of the overall aims of the project, using the same process as L.W. The researchers discussed the findings of their coding and analysis to establish whether there was consistency in the emerging themes. Where there was any discrepancy, the view of L.W. was adopted as she was present at the focus group (Darlaston-Jones, 2007). Overall, there was consensus between the two researchers about the themes arising, and only minor modifications to the names of the themes were made. Five global themes and subthemes were derived and refined by discussion. Following this analysis, L.W. then reread all of the coded data within the themes to verify that the coded sections fit within those subthemes and global themes.
Results
Twenty-eight families responded to the invitation letter (33 individuals), expressing an interest in the study. Sixteen parents attended focus groups and interviews in March and April 2008; two failed to attend the focus groups, and the other 17 were unable to participate owing to time pressures. Most of the group were white British, one was white Irish, and two were Chinese. A single participant did not declare their ethnicity.
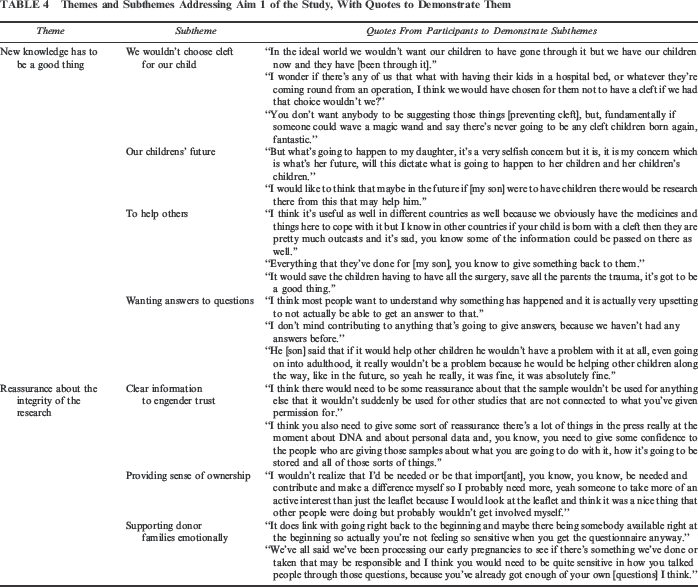
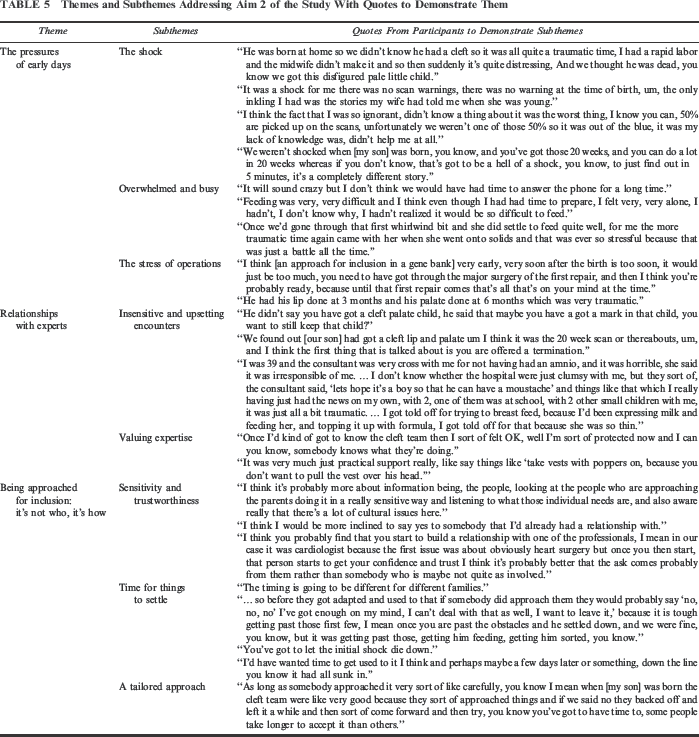
The mean duration of each group was 1 hour, 16.6 minutes (range, 1 hour, 3 minutes to 1 hour, 29 minutes). Participants' details are shown in Table 3. Five themes and subthemes were derived. Two themes were concerned with potential motivators for participation in a gene bank–style research program and are shown in Table 4. Three themes explain how an approach to consent for inclusion should be made, and these are described in Table 5. Both tables include quotes from participants to illustrate these themes.
Participants' Demographic Details *
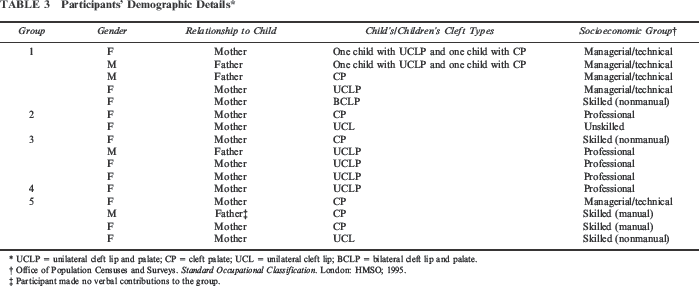
UCLP = unilateral cleft lip and palate; CP = cleft palate; UCL = unilateral cleft lip; BCLP = bilateral cleft lip and palate.
Office of Population Censuses and Surveys. Standard Occupational Classification. London; HMSO; 1995.
Participant made no verbal contributions to the group.
Themes and Subthemes Addressing Aim 1 of the Study, With Quotes to Demonstrate Them
Themes and Subthemes Addressing Aim 2 of the Study With Quotes to Demonstrate Them
New Knowledge Has to Be a Good Thing
All of the participants expressed a view that there were positive gains to be made through research into the causes of cleft but stressed that they had accepted their child and would not change him or her. Several described how they openly discussed cleft with their affected children, who were aware of the genetic implications from a young age. The acceptance of cleft by the family did not appear to conflict with a simultaneous desire to understand more about causation and potential to prevent oral clefts.
We Wouldn't Choose Cleft for Our Child
Participants were generally of the view that life would have been easier for them and their children if their child(ren) had not been born with the condition. The overriding sense was that, ultimately, no parents would wish their child to be born with cleft. Consequently, participants accepted that the ultimate aim was to prevent cleft and discussed this as a largely positive thing.
Our Children's Future
Parents seemed motivated to make a difference by participating in cleft research and were receptive to seeing an increase in knowledge of the causes of cleft for the sake of their children and other generations. This was often discussed in terms of their child's reproductive decisions.
To Help Others
There was also a perception of the global benefits of providing information to reduce the chances of children having clefts in the future. The benefits of the cleft care received in the United Kingdom, which is free of charge at the point of use within the National Health Service, were appreciated by many. Some explored issues of the lack of cleft care and resources for research in developing countries and felt the cleft gene bank might have an impact on the potential of preventing clefting in future generations.
In addition, some participants seemed motivated to participate to give something back to those who had provided care for their child. This may be related to a perceived association of their cleft team with the proposed future research. A common thread appeared to be a desire to save others from experiencing what these families had experienced themselves.
Wanting Answers to Questions
Participants raised questions about what caused clefting in their own child and appeared motivated to take part in both the current study and the cleft gene bank.
Several wanted to know the results from future gene bank research and generated a number of ideas for communication of findings including Web-based material, newsletters, and meetings with fellow participants to discuss results.
Much of the time in focus groups was spent gathering information about how the study might be set up and what findings might arise. Some parents considered the long-term implications of enrolling a child into a research project by proxy. Participants seemed to think that their children would also want answers to questions.
Reassurance About the Integrity of the Research
Participants wanted reassurance that samples would not be used for any other purposes or projects apart from the specific cleft gene bank.
Clear Information to Engender Trust
Information about the study was seen as essential, together with the need to include information about what was being done with the samples and who would have access to data and samples. Participants appeared to be more concerned about this than with procedural aspects of obtaining samples; they considered blood tests and saliva samples to be commonplace in genetic research and easy to obtain. There was no overall consensus among participants on the use of cell lines and “waste” tissue samples (from closure procedures). Some found the thought of a tissue sample more tangible. Others thought that the use of cell lines was somewhat “creepy.” Participants' responses emphasized there was a need to engender a sense of trust and confidence from the researchers that the samples would be used appropriately. Overall, the participants reported that if enough information was provided, they would be happy to give samples.
Providing Sense of Ownership
Participants considered that parents participating in future research would want to feel a sense of ownership in the project. They recognized this as a long-term research project and that contributors needed to be valued. This would potentially ensure better participation rates, and the contributors would see this as a something with which all would want to be involved.
Supporting Donor Families Emotionally
Participants raised the issue that there should be emotional support both during the completion of any questionnaires and throughout any potential gene bank study. Being provided with information about other sources of support (sign posting) was also discussed. This was particularly influenced by parents' worries about being asked for information about agents they perceived as responsible for causing their own child's cleft. Several participants described how they felt a sense of guilt that they had caused the cleft or that they were blamed by others for the anomaly. These issues ran throughout the focus groups and interview.
The Pressures of the Early Days
Parents' experiences of the birth of their child can influence initial parental coping and adaptation. Even though experiences were recounted retrospectively, participants vividly conveyed the intensity of the emotional and practical demands they faced following the birth of their child. These early experiences would influence the ability and inclination of parents to participate in research, and it seems that the early days are not the time to approach parents for inclusion.
The Shock
Many participants described the feeling of shock at discovering their child would be or was born with a cleft, and some related this to the appearance of the cleft itself. This theme was common to all groups. Not all parents had received a diagnosis of a cleft at the 20-week ultrasound. There were differences in perceived pressures between parents who had received a diagnosis antenatally and those who learned of the cleft at birth or shortly afterward. Many participants assumed that not having an antenatal diagnosis made the initial discovery harder to deal with and spoke about the psychological benefits of being able to prepare as a family for the child's difference where a diagnosis had been made at the 20-week ultrasound. This was countered by others who considered that an antenatal diagnosis increased stress during the pregnancy and added the issue of whether or not to proceed with the pregnancy.
For those who learned of the cleft at birth, the diagnosis came at a time when other new baby adjustments were required. Some participants had experienced a lack of understanding about feeding and other cleft-related issues at the maternity hospital, prior to seeing a cleft specialist. Participants were anxious when their baby had feeding difficulties (and, for one family, weaning was a stressful time). They made it clear that their time was fully absorbed with all of these issues and anything else would be an unacceptable burden. Any approach to join a gene bank should be avoided at this time.
Some participants had additional worries from having a child in a special care baby unit or from tests carried out to establish the exact nature of their child's anomaly. Some participants described interactions with health care professionals who were perceived as placing participants under duress to undergo further investigations or procedures, including amniocentesis and, in some cases, termination of the pregnancy.
The Stress of Operations
Participants described the particular pressures of their child having to undergo surgery.
Despite the stresses of the period after the birth, several participants emphasized that their child and indeed the family were doing well at the time of the study and had adapted to living with cleft. The improvement they and their child experienced as the child grew and developed was a theme running through the focus groups. Many stressed the positive side of the experience of having a child born with a cleft.
Consideration should be given, therefore, to approach families when they are moving toward adaptation, even though this may not be a predictable or linear process. This factor is seen within the “time for things to settle” theme.
Relationships with Experts
Throughout the early stages and subsequently, participants' experiences with health care professionals were mixed. This could have implications for initial coping and adaptation to early day pressures, which in turn could affect the point at which parents would be ready for approach for inclusion.
Valuing Expertise
Although some participants experienced negative comments and pressures from health care professionals, overall there was a feeling that they valued the expertise from cleft team and CLAPA personnel and trained parents. At the time of diagnosis, some participants saw the cleft team within a very short space of time and praised their sensitivity as well as the quality of the advice and support they received. Other parents had received support from CLAPA in the form of advice and practical issues such as ordering feeding bottles.
Being Approached for Inclusion: It's Not Who, It's How
The role of the person undertaking the approach was not as important as the manner in which this approach was made. When asked who the most appropriate person to approach future participants would be, there was no consensus within or between groups, although the specialist cleft nurse was the person mentioned most frequently. On the basis that the person approaching may be part of the cleft team, the experiences participants had with various members of hospital staff appeared to be important.
Sensitivity and Trustworthiness
Although participants were not directly asked to describe the attributes desirable in the person approaching them for inclusion in a gene bank, many volunteered their opinions in this area. Common attributes included sensitivity, trustworthiness, and the professional's ability to identify the most appropriate moment for the approach.
Several participants expressed the importance of being approached by someone they knew (e.g., another parent) or a health care professional they had already met.
In addition, being given the appropriate information and the ability to talk through practical aspects of the study was important to several participants. For some, there appeared to be an information paradox: At times, too much information was provided, and at other times, too little.
Time for Things to Settle
All groups identified a need to give families time for the initial practical and emotional demands to subside. Again, there was a clear sense of the need to consider the particular trajectory (in terms of experiences and circumstances) of individual families. Participants were asked to consider potential difficulties that parents might encounter if asked to partake in research as soon as possible after diagnosis. There were specific time points identified as to when an approach would be less welcome: the time of the diagnosis, surgery admission, feeding, and weaning stages.
A Tailored Approach
It appears important to tailor the manner in which an approach is made and the methods of delivering information to the individual family. Many expressed empathy for other parents and not only gave their own opinions about how the approach should be made but also speculated about how others may feel. Several participants stressed the importance of considering family circumstances, and according to some, the local cleft teams excelled at this, as shown in Table 5. Some participants felt they would prefer to be approached about the study in person, and others considered that a leaflet briefly introducing the study, followed by personal contact, would avoid overburdening parents. There was agreement that approach methods should be as inclusive and as flexible as possible to encourage participation.
Discussion
This study indicates that parents of children born with a cleft may be in favor of the establishment of a cleft gene bank and that they would actively contribute to such a resource. Insights into the research question, “What might motivate parents of children born with CLP to take part in a research program involving a gene bank?” are provided by the theme “New knowledge has to be a good thing” and countered by “Reassurance about the integrity of the research” (see Table 4). In response to the research aim to discover “parental preferences on how they should be approached for inclusion in a cleft biobank,” the themes “The pressures of early days” and “Relationships with experts” influence the theme “Being approached for inclusion: it's not who, it's how,” which gives an indication of potential contributory factors and influential processes (see Table 5).
What Might Motivate Parents of Children Born with CLP to Take Part in a Research Program Involving a Gene Bank?
The findings suggest that parents of children born with a cleft who agreed to participate in this study want to be involved with efforts to answer questions about the etiology of the condition. One motive for participating is the perceived benefit of knowledge for future generations of an individual's own family as well as those affected worldwide. Parents indicated awareness that other countries may lack the skills, resources, and research to enable children born with a cleft to have a normal life. Other work with families of probands affected by different genetic conditions has supported these findings (Ponder et al., 2008). Many parents, in the absence of definite answers concerning the causes of cleft, carry a burden of responsibility about their child's diagnosis that appears to contribute to the motivation to participate in research concerning etiology; this requires further exploration. Further work is required to understand which of these motivating factors has the greatest impact on parents, to ensure that parental expectations of the potential outcomes of the research are realistic.
This study has highlighted the need for further careful exploration of issues relating to consent by proxy for the affected child. Participants felt that their children would favor participation, but as this issue was not explored in depth, it requires further clarification. Other work has shown that 46% of respondents, when asked about their hypothetical involvement in pediatric research, felt they would want to be contacted again as adults to provide renewed consent (Goldenberg et al., 2009). The current study supports the qualitative work undertaken by Kaufman and colleagues (2008); both studies have demonstrated that parents have considered the rights of the child in their long-term involvement in large-scale biobanks. In addition, a questionnaire-based study in the United States has demonstrated that parents would be happy for their child's blood to be stored if the child's permission was also sought (Tarini et al., 2009). It is often the case that genetic material is gathered and stored for future (and sometimes, rather vague) research. The fact that participants want to know exactly how the materials will be used and are concerned about other uses is really critical in informing protocols for consent for gathering and using these kinds of data. Perhaps participants realize that although they want to believe that clear answers are possible, this is a remote possibility, and prevention of clefting will be difficult to achieve. However, one participant expressed the view that one motive for taking part in gene bank research was to seek reassurance that efforts are being made to understand the cause.
Efforts to engender trust and an understanding of what a cleft gene bank is and what it entails were seen as important by many. Participants emphasized the need for absolute clarity on data protection. It is known that participants appreciate the benefits of genetic research despite having suspicions about potential uses of the information (Bates et al., 2005). Those with inheritable cancers are known to positively support genetic research, but security and confidentiality of data are important concerns (Henderson et al., 2008). Reassurance will be needed for participants regarding the security of donated samples long term. They also need to realize that follow-up information on other aspects (e.g., data on the children of children born with OFC) may be requested. This will affect the design of initial and subsequent consent forms and information sheets.
A further issue is that in wider, non-OFC biobank studies, parents have concerns that genetic information about their children could be used as a basis for discrimination later in life (Kaufman et al., 2008).
Parental Preferences on When and How They Should Be Approached for Inclusion in a Cleft Biobank
The results highlight that there are difficult times in families' lives when an approach for inclusion would be less welcome. There appears to be strong enough evidence from the current study and from others that it is inappropriate to approach potential participants at these difficult times, despite the potential benefits to researchers of minimizing recall bias, which might occur if data collection is delayed. The participants' needs and the researchers' priorities must be carefully balanced. Considerable stress resulting from new baby issues, difficulties with feeding, surgery, and the anticipation and aftermath of surgery were vivid in participants' memories. Others have shown that feeding difficulties and the experience of surgery are stressful periods for parents (Young et al., 2001; Kuttenberger et al., 2010). In this study, the stress associated with these and other difficult times influenced participants' views about how and when an approach to participate in a gene bank should be made but also motivated them to want to take part in research.
The difference in the two subthemes of relationships with experts is stark; on one hand, several participants had had very positive experiences, especially with CLAPA and cleft team members, but there was regular mention of upsetting suggestions such as termination of the pregnancy and a lack of sensible feeding advice. It is likely that the relationship that participants had with health care professionals influenced both their ability to cope with the challenges they faced and also their attitude toward the teams they met. These may in turn influence participation. Participants appeared to be happy for various health care professionals or a CLAPA representative to approach them, but sensitivity and an awareness of the family's situation were considered essential prerequisites for this task (i.e., “it's not who, it's how”). Many expressed a preference to be approached by someone (another parent or health care professional) who already had a relationship with the family. It is known that parents of children born with a cleft appreciate the support provided by fellow parents (Nusbaum et al., 2008). The apparent desire for the approach to be made by someone who is familiar and trusted must be balanced alongside any perceived coercion to participate, if the invitation to participate were to come from the treating clinician or other member of the cleft team. Parents may believe that were they to participate, their child would receive more attention and better treatment (de Melo-Martin and Ho, 2008). Others may feel they would be letting down the cleft team by not participating. In the current study, some participants appeared to want to give something back to the cleft team. A potential solution may be for the clinician or other cleft team member to act as a middle man and allow the full process of valid consent to be facilitated by another member of the research team. In this study, all participants were cared for by one regional cleft team. It may be that participants from other regions would have expressed different views.
Participants felt that the amount of information offered to potential cleft gene bank contributors should be carefully balanced; sufficient detail should be provided so potential participants could make an informed decision about participation but not so much that potential contributors felt overwhelmed. Individuals vary considerably in the amount of information they prefer and differences in coping style are a factor (Folkman and Lazarus, 1980). This study supports the findings from the Healing Foundation Patient Information Project (The Healing Foundation, 2008). When acquiring information, people with visible disfigurements favor face-to-face contact with health care professionals, with a tailored approach to the amount and detail of information provided, based on the needs of the individual person.
Focus Group Dynamics and Reflections on the Role of the Facilitators
Researching this subject qualitatively through the medium of focus groups has facilitated an in-depth exploration of participants' perceptions. Focus groups were chosen in preference to in-depth interviewing since participants can support each other and can engender a perception of safety in numbers (Kitzinger, 1995). The use of focus groups appeared to facilitate understanding and empathy. Participants compared and contrasted experiences and appeared able to open up and talk about personal issues. Similar disclosures were made in the interview possibly because one of the facilitators took on more of a participant role as she disclosed that she had a child with a visible difference. This changed the insider-outsider barrier (Corbin Dwyer and Buckle, 2009), perhaps putting the participant at ease. Some participants were couples, which may have had an effect on a partner's willingness to divulge certain things or to express a personal opinion. The lead facilitator (L.W.) emphasized her role as researcher rather than clinician so that the participants did not feel inhibited about discussing their experiences with the cleft team. No additional influence of the researchers on the proceedings was evident.
Validation of the Results
The data were analyzed by a second researcher who read and analyzed all of the transcripts. She was unaware of the research questions, although she was not blinded to the research aims. There was agreement on emerging themes, and where there was any lack of agreement, this related to the naming of themes rather than what they represented. An in-depth assessment by the two coders of noncoded sections of the data helped validate the data and strengthen the themes that emerged.
During the data analysis, there was sufficient overlap and repetition of themes to draw conclusions, and there was no overwhelming evidence that further data collection would yield new themes.
Study Limitations
This work was undertaken as a pilot study to inform the establishment of a cleft gene bank based in the United Kingdom. It is a small study with a limited participant group. The nature of qualitative research means that there will inevitably be differences between this group and others who may take part in similar studies. The study gained data from only 16 of approximately 200 potential participants, so there may be a selection bias. It is possible that the methods of approaching potential participants for this study (i.e., with a letter from the director of the cleft center) may have been an influencing factor on participation rates; if parents had negative views about genetic research or the cleft team, they may have been unwilling to take part for fear of disappointing the cleft team by revealing such opinions. In addition, parents may have thought that the time commitment required for participation in the focus groups was too great. No information was available to characterize those not taking part in the current study, with respect to details such as time pressures, demographics, or cleft type. Owing to the restrictions of U.K. data protection law, the research team was unable to access the database used to make this initial approach (undertaken by a third party), which contains information about the nonresponders.
Although in this study participants were in favor of the establishment of a gene bank and an associated research program, a greater understanding of factors that may prevent people from contributing to gene banks is needed. A variety of concerns about genetic research more generally have been reported among participants in the United States (Bates et al., 2005), including the fear of the creation of genetic classes or of forms of racial discrimination. Studies to discover differences within and between minority ethnic groups are important to highlight any cultural differences that exist, aid the recruitment of representative samples to cleft research, and also further enrich our understanding of motivation to participate. Differences in cultural or religious beliefs (e.g., toward science and the donation of blood samples) may influence findings, although neither this nor ethnicity were raised as issues in the current study.
Despite the recounting by participants of real and valid experiences, it is acknowledged that the participants are not necessarily representative of all parents who would be approached for inclusion in a cleft gene bank in the future. The 16 parents in the current study all expressed their willingness to participate in gene bank research, but they were self-selected and may have been more motivated in this regard. Any potential dissenters within the focus groups may have been reluctant to voice their opinions, perceiving the majority to be in favor. L.W. may have been perceived as being part of the cleft gene bank research team, and this may have influenced respondents to express more positive views.
Future Directions
This study has focused on the parents of children born with a cleft lip and/or palate. The children themselves, and adults who were born with a cleft, are also stakeholders in this process, and their views should be sought through further studies to strengthen the current work. There are sensitivities to consider in such research. If the aim of the cleft gene bank is to prevent cleft, then those born with the anomaly may find it difficult to discuss the merits of such a research program. In addition, adults with clefts may conceive children with a greater than average chance of having a cleft. As future parents, their opinions should be sought and taken into consideration when a cleft gene bank is created. Owing to the lack of information available about the nonresponders in this study, consideration should be given to future studies assessing the impact that such a gene bank may have on minority ethnic groups, as they may not have been fully represented here. For instance, focus groups led by community leaders of different cultural groups may prove fruitful.
Conclusion
This pilot study used qualitative research methods to demonstrate that a sample of 16 parents who have children born with OFCs are positive about future research into etiology. Wanting answers to their own questions, they considered that new knowledge was desirable, but they also required reassurance about the purpose and integrity of the project. An individualized approach toward parents was perceived to be important, particularly as this approach is likely at a time when there are considerable pressures for a new parent of a child born with a cleft. Further work is required to extend the findings of this initial study, but this preliminary research is useful in informing the establishment of a cleft gene bank in the United Kingdom.
Footnotes
Acknowledgments
This work was supported by the Craniofacial Society of Great Britain and Ireland. The authors would like to thank Dr. Fiona Fox, Mrs. Rosemarie Winter, Mrs. Liz Albery, Dr. Kate Gleeson, and all the participants for their invaluable contributions to this research. This work was supported with a grant from the Craniofacial Society of Great Britain and Ireland, with a further indication of funding from the Healing Foundation.