
Abstract
Objective
To explore the views of children with cleft palate and their parents about daily life with otitis media with effusion and associated hearing loss.
Design
A qualitative study. Semistructured interviews were used to collect data from parents. Participatory techniques, including activities on a tablet computer, were used to collect data from children. Framework analysis was applied to interview transcripts.
Setting
Two English cleft units.
Participants
A purposive sample of parents of 37 children aged 0 to 11 years with experience of otitis media with effusion. Their children also took part if aged 6 to 11 years (n = 22).
Results
Themes related to the following: (1) emotions (frustration, anger, sadness, happiness, anxiety), (2) educational experiences (struggling at school, having to sit at the front of the class, requiring extra support, missing lessons for appointments or due to ear infections), (3) social interactions (isolation, communication, reliance on siblings, participation in activities).
Conclusions
A number of areas of interviewees' everyday life were affected by the presence of otitis media with effusion. Parents may need to be forewarned about the possible ongoing nature of this condition and its impact on a child's social and emotional experiences. Children may also benefit from age-appropriate information about otitis media with effusion and its treatment, including information on hearing tests, to help reduce any anxiety.
Otitis media with effusion (OME) is common among children with cleft palate with or without cleft lip (CP±L); approximately 90% will develop this problem (Grant et al., 1988; Sheahan et al., 2003). Research suggests that health-related quality of life for those with OME can be affected due to sleeping problems, irritability, and emotional distress, as well as hearing loss (Brouwer et al., 2005). Regular tests are advocated for early detection of OME (Sheahan et al., 2003), with treatment using either ventilation tubes (VTs) or hearing aids (HAs) recommended if the condition has not resolved within 3 months (National Institute for Health and Care Excellence [NICE], 2008).
Despite the frequency of OME as part of CP±L, previous research has not explored in-depth the views of children and their parents on living with hearing-related difficulties. It is important that their opinions are investigated to provide practitioners with an insight into how OME affects people's lives. Such an understanding could help clinicians when giving information to and making treatment decisions with parents and children. A systematic investigation was therefore planned to examine the impact of OME on the lives of children with CP±L and their parents.
Research described below formed part of a feasibility study prior to developing a trial to compare VTs and HAs for addressing OME in CP±L. This paper centers on what children and parents said about daily life with OME.
Methods
Design
Given that this subject has not been covered in the past and we wish to explore it in-depth, qualitative methods were considered appropriate because their overall aim is “describing, debating and offering insights into a phenomenon” (Smith and Bekker, 2011, p. 48), striving to understand “the meanings that people draw from the situations and activities in which they are involved” (Sim and Wright, 2000, p. 46). In qualitative research, data collected as part of a project, rather than predefined theories or hypotheses, tend to guide the analysis (Knudsen et al., 2012). The Greater Manchester East Ethics Committee approved the study.
Participants
Participants were recruited from two cleft units in the U.K. Parents were eligible to take part if they had a child with nonsyndromic CP±L aged 0 to 11 years with experience of OME (current or in the past). Their child with CP±L was also involved, if aged 6 to 11 years and willing to talk to a researcher. To incorporate a broad range of perspectives, a purposive sample was selected to include children of both genders with variation represented in types of cleft and treatment received for OME. A sampling matrix was used to help ensure diversity among participants (Harman et al., 2013). We continued recruiting until data saturation, which is the point at which no new themes or ideas emerge from additional participants (Morse, 2000). Our approach to recruitment reflected the requirement for a qualitative research sample “to be of such a size that it will generate a volume (and perhaps also a diversity) of data that will provide meaningful insights” (Sim and Wright, 2000, p. 50).
Data Collection
A topic guide was developed for interviews with parents, which started with a very broad question: “Tell me about the history of [child]'s hearing?” Other areas covered included impact of OME and its management on family routines and the child's day-to-day activities. Open-ended questions were asked to encourage parents to share their experiences, with probes used to follow up responses given by interviewees (e.g., “Can you tell me a bit more about that?”).
A separate interview was conducted with children to ensure their views were given equal prominence to those of parents and because we used a different approach to data collection with these young participants. Activities, most carried out on a tablet computer, were devised to explore children's views. Topics covered with children included feelings related to not hearing and what this stopped them from doing. In addition, they were asked how they would describe the problem they had with their ears to another child.
Field notes were made after each interview to record overall impressions. Recordings were transcribed verbatim as soon as possible after an interview so that emerging ideas could inform future data collection. Each parent and child was interviewed once by the first author, a White British female nonclinical researcher, who did not know participants in advance. Parents gave informed written consent for their involvement and, if appropriate, for involvement of their child. Written assent was sought from children prior to their interview.
Analysis
Data analysis explored transcripts systematically. It involved summarizing what people said to allow for description and then interpretation. Framework analysis was used for this purpose (Ritchie et al., 2003); it was developed for use within social policy and applied research. It consists of five stages: (1) Familiarization with the data (becoming immersed in material collected from interviewees); (2) developing a thematic framework (identifying key issues in transcripts); (3) indexing data (labeling key issues that emerge for each interview); (4) devising a series of thematic charts (allowing the full pattern across cases to be explored and reviewed); and (5) mapping and interpreting data (looking for associations and providing explanations). The qualitative computer program NVIVO-9 (http://www.qsrinternational.com/) assisted with the management of data and producing matrices. The matrix-based nature of framework analysis facilitated sharing of data with members of the analysis team, which consisted of three researchers and three clinicians working with patients who have CP±L. This allowed for ideas relating to coding of transcripts to be debated. It also enabled members of the team to check how data were charted by the first author.
Results
Data collection took place between March and August 2012. Out of 52 families invited to be part of the study, 37 participated (five were from minority ethnic groups). Of those declining, six felt that hearing had not been a problem for their child, six could not be contacted when telephoned to arrange an interview, two did not have time, and one person canceled an interview after agreeing to take part. Most interviews (32 with parents and 19 with children) were carried out in participants' homes; the remainder were conducted in the clinic at parents' request. All but one interview was digitally recorded and transcribed verbatim; one mother of an infant did not want her interview recorded but was happy for the researcher to take written notes.
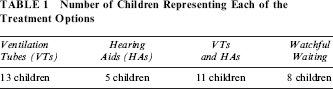
Six interviews were conducted with a couple; whereas, one father and 30 mothers were interviewed on their own. Interviews with parents took between 20 and 65 minutes. The mean age of parents was 34.9 ± 6.7 years. Their children (21 boys and 16 girls) had unilateral cleft lip and palate (n= 13), bilateral cleft lip and palate (n= 6), and cleft palate only (n= 18). They experienced a range of treatment approaches, as shown in Table 1, which highlights that not all had received VTs and/or HAs. At the time of interview, six children had VTs and 11 had HAs. Of the remainder, parents of 11 children felt hearing was no longer a problem; whereas, parents of six children were considering VTs and parents of three HAs, due to difficulties these children were still having with communication and interaction. Of those with experience of VTs, 10 had them inserted on more than one occasion. The average age for first insertion of VTs was 24.5 months, occurring alongside another procedure in more than half of cases. This compared with 48.2 months for the first experience of HAs.
Number of Children Representing Each of the Treatment Options
Data were collected from 22 children, 13 boys and 9 girls, whose mean age was 8.8 ± 1.3 years. Two children aged 6 to 11 years did not want to be involved, so only their mothers were interviewed. Interviews with children took between 10 and 40 minutes.
Analysis highlighted that the impact of OME spanned several areas of a child's life and affected the wider family, including parents and siblings. Three main themes emerged from the data about OME and daily life for participants, relating to emotions, learning and socializing. These are discussed below, with quotations from interviews included to support our interpretation. Pseudonyms are used to protect participants' identity.
Emotional Impact
Narratives contained rich data about the emotional impact of OME. Participants implied that the ongoing, fluctuating, recurring nature of OME and whether it was accompanied by an ear infection were responsible for negative emotions, rather than severity of hearing per se. Frustration stemming from a range of sources was clearly expressed in numerous interviews. Parents became frustrated when calling their child and not getting an answer, wondering whether this was due to selective hearing rather than a lack of hearing:
Stuart's [aged 5] mother: I would get irate…I'd say, “Are you not listening to me?” I mean I can hear a pin drop, you know, and his dad can hear the same and you know, you kind of think he's ignoring you and maybe he's actually not, he just didn't quite catch what you've just said…
Children themselves talked about feeling upset when unable to hear people addressing them:
Richard [aged 10]: I was like getting a bit like sad almost 'cause like mum had to repeat [herself] every single time and I was like I wish she didn't have to do that.
They also became frustrated when others struggled to understand what they were saying, according to parents. Miranda's mother said that when her daughter became annoyed because she could not be understood it affected her siblings, adding “at times it's quite a lot but the moodiness, yeah, the other two children know that she's more moody about it.” Likewise, Henry's [aged 7] mother recalled how this child behaved in the past:
Oh, he was not a very nice toddler [laughs]. He was quite difficult as a toddler…when other kids were all starting to speak and he couldn't communicate properly with other children…he'd like lash out, you know, he'd try and talk to them but obviously he wasn't making the right sounds and then he'd get frustrated and he was quite physical…
It was common for interviewees to discuss emotions when mentioning treatment for OME. Sometimes this was positive, if VTs or HAs were seen as having helped with hearing. For example, Stuart's mother extolled the benefits of VTs. She recalled how they enabled her child to hear bubbles in the bath, which caused her to cry with relief. Likewise, Claire's mother was ecstatic when her daughter received HAs after several sets of VTs, calling them “little miracles.” However, other emotions associated with treatments were less pleasant. For example, whereas some parents saw the insertion of VTs as a simple, relatively risk-free procedure, others talked about the turmoil they underwent witnessing their child being anesthetized for surgery. Children themselves expressed concerns about operations, stating they did not really know what happened in the surgical theater and wondering whether it would hurt. Some patients talked about feeling VTs inside their ears. Worries were also expressed by children about whether HAs would hurt. Ian recalled thinking that they might be uncomfortable and could give him an electric shock if wet. Parents' anxiety about HAs related to fears of bullying, which did not transpire for children who wore them, although John was annoyed that peers wanted to keep touching them. Children who wore HAs could be frustrated if batteries ran out when they were in the middle of an activity. Some also found it uncomfortable when HAs whistled or amplified background noise, such as babies crying in a restaurant,
Chris [aged 8] said: Well it makes me a little bit, when they do it, it makes me feel like wanting to go over and just say, “Can you just shut up that baby please?” …It's just really going through my ears and hurting them…it drives me a bit crazy and you don't want to see me crazy.
Interviewer: So when you're in the restaurant what will you do?
Chris: I turn them [HAs] off…and start trying to calm myself down, but when I put it on, turn them back on, if they're still screaming I turn them off again and if I turn them off three times, a third time, I just start getting a little bit more angry every time.
Parents could be frustrated that treatment failed to cure their child's hearing problem. Some believed that in the case of VTs, their child's situation became worse due to ear infections they associated with their insertion. A couple of parents were annoyed because they felt they were not listened to by practitioners when expressing their reluctance to have VTs:
Claire's [aged 10] mother: They said that it would be an in-and-out job, they would get it done and she'd be home and I would see an improvement. There was no improvement at all, she got an ear infection just a week later and was very ill with it… After every hearing test, it showed how poor her hearing was and I still went away confused as if to say…what's gonna happen next, and every time it was oh grommets, grommets, and I kept saying it's not working…
Jeremy's [aged 10] mother: I think him having the grommets has caused more agony and ear infections and sleepless nights and like I as a parent not even knowing how these things, how they were going to put because I remember the last time when I really got angry and refused they didn't listen to me.
As the quotation above implies, ear infections could leave parents feeling helpless because they were unable to alleviate their child's pain, which in some cases resulted in sleepless nights:
Elaine [aged 9]: Um yes, like every week, every few weeks I get an earache…one night when I had my earache in the left ear I just went in and said “my ear's really, really sore”…I was like up till 4 o'clock in the morning just going I'm going to die if I keep on putting up with it.
Jeremy [aged 10]: Like it always like comes, like probably if it's gonna hurt it'll come at night, not like day time ‘cause well, it just hurts…like right now it's not hurting, but if I was to pain it would do it at night. So that's why I don't get any, much sleep.
Some children appeared to be frightened each time they had a hospital appointment but struggled when asked to specify what exactly caused their fear. Laura's mother suggested it may be because tests can lead to procedures that necessitate a stay in hospital. Hence, even simple assessments, such as a hearing test, caused some young interviewees to feel anxious. This was compounded, according to Henry's narrative, by seeing different practitioners and feeling shy when meeting new people. Parents could also be apprehensive attending appointments in case their child needed a procedure, as the following interview extract indicates:
Jason's [aged 10] mother: …you dread the hearing tests that are coming up then, and then we do it and everything's fine…
Jason's father: …can't sleep the night before can you…
Jason's mother: I couldn't sleep on the [day] last week coming to the cleft palate team but that's just the way I am.
Jason's father: Because you fear the worst, don't you…
Jason's mother: Yeah, ‘cause I just thought because [speech therapist] had said he had like a nasally, like a very throaty speech. So I'm thinking, either his tonsils need to come out or his adenoids or maybe there's an air gap in the cleft palate repair, grommets, anything.
Effect on Learning
Children who had little problem with hearing loss did not appear to experience significant educational difficulties. In contrast, those who had ongoing or repeated OME were said to be hindered in their learning because they misheard things, missed key information from teachers, or struggled with words. Some parents talked about the child's hearing problem only being detected once at school because they entered a setting with more people and noise. Children mentioned that teachers spoke loudly so they could hear. However, it was sometimes difficult in the playground, dining hall, or assembly due to background sounds (e.g., others chattering, acoustics in the hall). Talking about how loud pupils could be at school, Jeremy said, “I just feel like telling them you're gonna break my hearing aid.”
Problems with learning could occur before OME was identified. For example, prior to Joanna's diagnosis, teachers labeled her as having attention deficit/hyper-activity disorder, yet once she had VTs she was better able to concentrate and her work improved. A similar story was recounted by other participants, who felt their child's ability to focus was hampered by his or her poor hearing and that learning advanced once OME had been addressed. Confidence in the classroom also increased in the case of Joanna, whose parents said she was less reliant on the teacher for help post-VT insertion.
Once a diagnosis was established, mothers and fathers made sure teachers were aware of their child's needs by talking to them at parents' evening and passing on details of outcomes following a clinic appointment. Most interviewees requested their son or daughter be given a seat near the front so the child could see the teacher's mouth. Several children mentioned they could not hear when they were at the back of the classroom and felt it was better to be nearer the front, although Paul noted that this meant he had to be well behaved because the teacher could see what he was doing. When asked why he liked sitting at the front, David (who wore one HA) said because he could see better; in her interview, his mother said this child watched people's lips when they spoke. Some children who wore HAs talked about only using them in school, adding they were able to hear in the quieter home environment. Jeremy's mother felt that wearing HAs in the classroom was advantageous for her son because they were a visible reminder to teachers of his hearing difficulties.
Children who wore HAs received assistance at school from sensory services. Parents welcomed this help because staff from the service ensured that teachers understood the child's special educational needs. Some of these children also had one-to-one support at school to address speech and vocabulary delay. In Miranda's case this was stopped once she received VTs, which annoyed her mother, especially since the child returned to wearing HAs once the VTs fell out, yet the additional assistance was not recommenced. Likewise, Jeremy's mother talked about the extra support her son had at school being withdrawn, which she attributed to the local authority cutting resources.
Extra support was described by parents as necessary in some cases to prepare the child for secondary school. When this move was approaching, parents gathered medical information to send forward to new teachers to ensure their child was given appropriate support. Children expressed some concerns about how they would be treated at secondary school if wearing a HA. Likewise, parents wondered whether their son or daughter would be bullied or would manage with less support:
Jason's [aged 10] mother: …if he's at the back of the class, and I know in secondary school you can sit where you like…so that concerns me a great deal cause if Jason doesn't, if he can't hear you or can just hear a little bit he'll just go somewhere else [daydreams], you know…
Parents also worried that staff at secondary school may be less accepting of absences for medical reasons, including severe earache, if happening on a regular basis.
Children could lose time from school due to OME. School might be missed if the child had been unable to sleep due to earache, although some children insisted on going to school, even if in pain, so they had a full attendance record. Several parents talked about trying to keep school absences to a minimum because they knew that surgery would require more time off. This was easier to do when appointments could be arranged for the start or end of the day and if families did not have to travel a great distance to clinics.
Schools were described as varying in how well they accommodated children's health needs. Some parents said teachers had been understanding and cooperative. Others talked about being censured by the school:
Joanna's [aged 9] mother: We used to get letters home saying that her attendance was poor and it had fallen below what they say is the norm, and we'd say well, it's because of her hospital appointments, and then they started getting funny and saying…
Joanna's father: How many appointments does she have and things like that.
Joanna's mother: They needed every letter we got sent.
Joanna's father: They've eased off a bit now, haven't they…Since you tried taking like four letters in at a time, OK we believe you.
Several parents talked about changing jobs once their child was born, becoming self-employed, going from full-time to part-time employment, or opting to do night shifts so their work could fit in with the health needs of their child. Some had stopped working altogether. However, not everyone was able to accommodate appointments easily and, in a few cases, getting time off work was problematic, as the following quotation implies:
Judy's [aged 8] mother: Um, it was more difficult for my husband. He actually lost his previous job over it…my husband had a massive dispute with his ex-employer over time off due to Judy and lost his job…I don't drive…me husband with the car, it makes life a lot easier…You don't want to be dragging her on a train and things when she's going into hospital.
Bearing on Social Interaction
Problems with communication could impede children's social functioning and resulted in them becoming isolated from peers if they were unable to hear:
Claire's [aged 10] mother: She would keep away from children because she knew they wouldn't understand her and she wouldn't be able to hear them. In the playground they would be playing and chasing each other, and she wouldn't be able to hear and she would have to try and look at faces so she would withdraw herself…
Fiona's [aged 3] mother: She couldn't really communicate with anyone and for a long time, up until very recently, the teacher said that she's yet to initiate conversation with anyone …I think the hearing aids helped a lot and her speech is better ‘cause now the back of the palate is closed, she can talk better…
In some cases, parents would interpret for their child, acting as an intermediary, although Ian's mother implied that children could then become reliant on a parent talking for them. Certain interviewees also mentioned their child was quite clingy before their OME was addressed, which they attributed to a lack of confidence due to poor hearing.
It was suggested that children could come to depend on siblings, not only to interpret what they were saying but also as a source of company, meaning they did not always mix with their peers:
Elaine's [aged 9] mother: Yeah, at birthday parties and all them things she'd be sitting under the table with the dog while the rest of the children played…I think you know at that time as well she has a younger brother she'd rely on him a lot as well you know, he'd have made some friends and she tagged along…
As a consequence, some parents encouraged their child to engage in activities without a brother or sister, so they learned to be independent.
Swimming was a potential social event affected by OME. Interviewees noted that children with VTs or chronic ear infections were advised not to perform this activity for a specific period of time or to do so with an earplug, which could cause problems because it meant the child was unable to hear in the pool. They could also be self-conscious about wearing an earplug when others did not have one. Some parents had struggled to get individual tuition to ensure that their child was safe when learning to swim:
Judy's [aged 8] mother: When they send out the letters I think for getting ready for swimming lessons, I'm gonna mention it to them that you know she can't swim yet, she's still in armbands, and her friends may find that peculiar but there's a reason for it because like I say, I can't put her in a swimming lesson with 20 other screaming kids plus the earplugs in—she can't hear. She's not gonna learn to swim if she can't hear. So really I need, it needs to be more one-to-one.
Having HAs made parents feel less anxious when the child was outside the home. Prior to these devices, they might hold the child close to them due to concerns about traffic. Chris' mother said HAs allowed her son to have more freedom:
Chris' [aged 8] mother: …without his hearing aids he would be very limited. There's no way I would let him, I mean at the minute if he wants to play out and he'll play out just in front of the house, without hearing aids it wouldn't happen because he wouldn't hear the cars coming down, and also when we're in a park even when he has his hearing aids on I won't let him go too far because if I need to shout to him he won't hear me, he doesn't hear me, and without his hearing aids that would be impossible. He would have to stay next to me most of the time, I wouldn't let him run off.
Other activities mentioned during interviews that could be affected by hearing included ice skating and the cinema. Claire talked about her experience of going to the cinema before she had a HA:
Claire [aged 10]: I'd just sit next to my mum giving her a hug and watching it. Couldn't hear anything, I'd just watch it…and look at the faces and see what they were doing.
However, if a child wore a HA, it could make the sound in a cinema too loud. When this was the case, Ian said he took his HA out and put it in his pocket. Similarly, being at a birthday party, for some children, could be confusing due to the noise, described by Judy in the following way:
Judy [aged 8]: It was, it's a bit loud and when people are talking to me they're like, like midget voices.
Interviewer: Like midget voices, right, because they're squeaky, am I right? Why are they like midget voices?
Judy: They're like a little mouse talking to me.
Discussion
No previous known qualitative research has been published that explores how OME affects the emotions and everyday encounters of those with CP±L and their parents. Therefore, this paper helps to increase understanding of the psychosocial experiences of this patient population. Participants with CP±L and their parents reported a range of negative consequences associated with OME that could prevent children from engaging fully with their social world, due to emotional distress, educational delay, and communication problems. Although some children in our research appeared to have a good social life, for others hearing loss had a detrimental effect on their interaction with others.
Previous research has shown that children with cleft can become frustrated when they are not understood, which can result in them avoiding talking (Damiano et al., 2006). As a consequence, parents may compensate by talking for their child to avoid communication difficulties. We also found children turning to siblings as a source of support.
Cleft care should aim to optimize “facial appearance and function, feeding, hearing, speech and psychosocial adjustment” (Jeffery and Boorman, 2001, p. 189), yet our data highlighted that approaches aimed at correcting hearing loss could augment anxiety among patients and their parents. For example, fear surrounding the insertion of VTs was mentioned. In addition, some children stated they felt VTs in their ears. We tried to get them to expand on the discomfort they associated with VTs, but they struggled to do so. Although the VTs may have felt tight when first inserted, alternatively this might reflect the child's recollection of VTs falling out. Some children expressed being initially fearful of HAs, believing they might hurt. Those wearing these devices received extra support at school from a sensory team. This could be seen as marking them out as different to peers, but this was not an issue raised by children during interviews. Despite the anxieties associated with treatment, positive results were described by participants once hearing loss was corrected, including improved communication and the ability to concentrate and learn. This mirrors findings from other research, stating that parents noted changes in their child's behavior (e.g., less irritable, better at sleeping) when chronic OME was addressed (Facione, 1991). Unfortunately, however, rectifying the problem is not a simple one-off solution. For some interviewees OME was a sustained problem that continued to affect several areas of the child's life.
It may be beneficial to warn parents about the possible emotional impact of OME on children and prepare them for the potentially ongoing nature of this condition. It is acknowledged that this must be balanced against causing unnecessary angst, because for certain families we interviewed OME did not have a significant impact. However, most interviewees mentioned at least some aspect of daily life that was affected. In particular, children seemed anxious when attending what may be considered a simple and relatively painless hearing test or mold fitting. Children should be asked for their thoughts on OME and its treatment, otherwise their fears may be left unaddressed. Their anxieties might also stem from gaps in understanding and knowledge of OME. Fuller information designed for children, which explains procedures and interventions for OME in an age appropriate manner, might therefore be helpful.
Our data suggest that most children valued attending school and some continued going even if they had a painful earache. This may have been because they wanted to attend favorite subjects, a comment made by a couple of interviewees. It could also relate to a wish to be “normal” and to fit in with peers; a qualitative study involving 12 adults with cleft reported that they felt different from other children growing up as a result of the time they spent away from school due to cleft care (Chetpakdeechit et al., 2009). Extra attention may need to be paid to patients approaching a move to secondary school, when anxiety associated with hearing was expressed by parents and children. In preparation for this move, parents talked about providing information on the child's condition to the new school. Parents often described acting as a conduit between health care professionals and school; even though other services may be copied to documents about the child's hearing, this information may not be read or retained, meaning that some parents felt like the key link for the child and their interaction with different professionals, including teachers.
Strengths and Weaknesses
We followed guidelines for producing good qualitative research (Elliott et al., 1999), applying the following strategies for this purpose: (1) triangulation by seeking information from different sources and involving more than one researcher in the analysis; (2) keeping a diary to allow for transparency in terms of decisions made in conducting the study and developing themes; and (3) providing extracts from interviews to ground the interpretation in examples. We managed to gather data from children with CP±L as well as parents. Previous research has failed to explore the views of these individuals (Sharif et al., 2013). Results were based on participants' perceptions and recollections and interpreted through the lens of a multidisciplinary analysis team. The study highlighted areas of living with OME that may not have been considered by clinicians previously and, in that sense, the paper provides new knowledge in this area. Participants were invited to talk about something that may have happened many years previously (e.g., having VTs). To overcome this difficulty we tried to explore young interviewees' views about what it might be like for other children to have OME and to receive VTs or HAs. Interviews were conducted by a nonmedical, experienced qualitative researcher in participants' homes, which may have enabled more honest and candid responses than if they had been carried out in the clinic by a member of their treatment team.
Conclusion
Otitis media with effusion and associated hearing loss can have a negative impact on the daily lives of patients with CP±L and their family, including psychological well-being, educational performance, and social functioning. Children may have fears about interventions for this condition due to a lack of knowledge. Parents can feel helpless in how to support their child when they encounter problems such as poor communication and earache. Practitioners should prepare parents for the emotional turmoil that can result from OME. They should also ensure that children understand what is happening to them, assessing and addressing any anxiety they have related to this condition and its management.