
Abstract
Background: This quantitative educational intervention was conducted to determine the effectiveness of a 1 -day internal medicine orientation for new interns, led by nurse educators instead of medical doctors. Methods: Scheduled within the orientation week curriculum, this project had a purposeful convenience sample of 14 students comprising the entire intern class. An afternoon of 1:1 clinical skills with nursing guidance followed a morning of didactic lecture on medical knowledge and skills transfer. Students completed a pre/postmedical education test (MET) to evaluate knowledge and skills acquired. Results: Interns reported increased confidence with clinical competencies to both nurse educators and the chief resident. Outcome questionnaires revealed statistically significant increases in knowledge about clinical skills after the intervention. Interns witnessed interprofessional teamwork. Conclusion: Nurse educators teaching medical interns facilitates interprofessional team collaboration, communication, and mutual respect. This simulation pedagogy focusing on principles of deliberate practice can have a positive impact on academic and clinical performance.
Keywords
Many teaching hospitals designate June-July as the inaugural month for first-year interns ‘clinical training (Wright et al., 2013). Reaching a milestone of applying theory to practice, the next step involves transitioning to real-life clinical application as an intern. In addition to being ranked at the entry level of the medical hierarchical order, performance under the vigilant eyes of experienced senior residents brings added pressure to master required competences (Teunissen & Westerman, 2011). Having the intellect to retain and narrate information on disease entities and treatment plans lays the foundation for medical competency. However, intellect needs to be partnered with psychomotor skills when caring for patients.
In previous years at the medical school under study, new interns had on-the-job training from physicians, without simulation lab instruction. For this project, the chief resident and the chairman of the internal medicine department collaborated with the nurse educators as clinical experts to design and implement an orientation for first-year interns. The goal was to gain experience with basic medical procedures in the simulation lab in addition to on-the-job training.
Background and Significance
Before simulation entered the educational arena, interns practiced on patients in clinical settings. Simulation provides an alternative method of instruction without detrimental effects on patients (Barsuk et al., 2016). Procedures can be repeated until understanding and proficiency are acquired (McGaghie et al., 2011). The growth from beginning practitioner to competency is achieved by refining skills through active learning and exposure to changes experienced with multiple patient interactions (Benner, et al., 2009, p.104). Nurse educators understand how to facilitate critical thinking and how to guide students to incorporate theory into clinical application (Raymond & Profetto-McGrath, 2005). Leading an orientation for interns introduces the nurse as a partner in interprofessional collaboration.
Having the intellect to retain and narrate information on disease entities and treatment plans lays the foundation for medical competency; however, intellect needs to be partnered with psychomotor skills when caring for patients.
Purpose
The purpose of this study was to investigate whether an orientation for new interns led by nurse educators instead of medical doctors can be an effective intervention. Outcomes were measured by a pre/postmedical education test (MET) and performance of clinical skills with the nurse educators to verify proficiency.
Research Question
Is there a significant difference between pre- and posrintervention measures of knowledge for new interns attending a nurse educator-led internal medicine orientation?
Theoretical Framework
This study employed Ericsson and Poole's (2017) Theory of Deliberate Practice describing four steps that improve cognition, perception, and motor ability to achieve high levels of performance. The first step is having the motivation to challenge oneself to improve performance. The second step incorporates awareness of preparedness with a knowledge base suitable to comprehending the instruction given, in order to master the task at hand. Immediate feedback on one's performance is the third step, necessary for validation or rectification of task accuracy. The final step is for the learner to be consistent and maintain regular practice once proficiency is reached, while aiming for expertise (Ericsson & Pool, 2017).
Literature Review
The literature review explored clinical skills programs led by medical doctors and/or nurse educators nationally and abroad. Interprofessional collaboration in the early stages of medical training proved to be instrumental in understanding the various roles of the health-care team.
Clinical Skills Programs Led by Medical Doctors
The Council of the European Union Vocational Directives mandates 5,500 medical training hours for medical schools in member countries, but inconsistencies remain with individual institutions regulating quality and content of these hours (Cumming & Ross, 2007). Morris et al. (2016) surveyed 75 medical interns after 6 months of a 12-month training program at an Irish hospital, to evaluate the effectiveness of a clinical skills program. Halfway through the program, preceptors had not been given a report of skills competency levels attained by individuals. Over half of the students did not feel prepared for internship, with only 3 of 14 mandatory skills taught to 100% of students; the remaining 11 skills had been taught to 16%–72% of students. Eventually all students were instructed in every skill as they proceeded through the program, by utilizing deliberate practice to attain competency. Recommendations for improvement included standardization of clinical education.
McKenzie and Mellis (2017) assessed effectiveness of an Australian program in which 53 new interns participated in a mandatory skills program followed by 4 weeks of clinical practicum. Anonymous questionnaires were completed by 77% of students prior to and 70% immediately following the program. The study concluded that participants achieved significant improvements in skills and slight improvement in communication and organization.
Clinical Skills Programs Led by Registered Nurses
Elms and Chumley (2006) profiled 176 Texas medical students in a clinical skills cross-professional instruction developed and implemented by nursing faculty. Skills were reviewed, demonstrated, and practiced by students. Nursing faculty teaching skills laboratory received highly positive ratings from students, who felt markedly prepared for clinical practice. A Lebanese medical school investigated 132 medical students ‘clinical skills over a 2-year period when cross-professional instruction led by nursing faculty was established (Abdallah et al., 2014). Nursing instructors presented didactic lecture and, along with proficient nursing students, taught hands-on clinical skills. Data from 126 questionnaires revealed an extremely positive rating for nursing faculty and clinical skills. Qualitative responses noted satisfaction with the program and requests for additional simulation lab and hospital contact. Cross-professional instruction enhanced student capabilities and filled the void that previously existed to provide hands-on clinical skills prior to entering hospital internship.
Methodology
This educational intervention took place in an acute care hospital classroom and simulation lab. Previously, there was no formal curriculum used when new interns were taught by doctors. Skills training during internship was randomly experienced, depending on assigned patient cases. Interns had no opportunity to learn clinical skills in the simulation lab taught by doctors or nurse educators. This purposeful convenience sample of students (n = 14) comprised the entire intern class. Training commenced during orientation week. Given the composition of the educational program, university institutional review board approval was deemed not necessary.
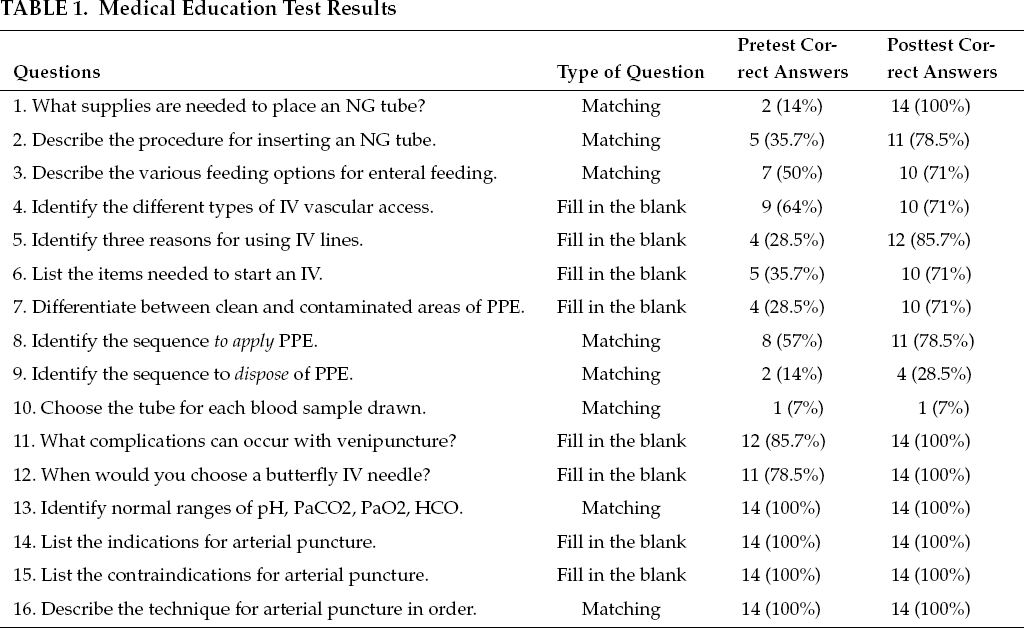
The intervention began with all students completing a preproject MET designed by the nurse educators, to evaluate their current knowledge. The MET, based on a comprehensive review of clinical skills and knowledge commonly required for hospital internship, covered primary and subtopics of nasogastric (NG) tubes, intravenous (IV) therapy, personal protective equipment (PPE), blood collection, and arterial blood gas (ABG) interpretation (see Table 1). Content validity was established through consultation with the chief resident, nurse educators, and medical-surgical nurses from units that commonly worked with interns.
Medical Education Test Results
After completing the preproject MET, a didactic lecture reviewing skills application with supporting rationale was followed by clinical skills training in the simulation lab with 1:1 nurse educator guidance. Clinical skills were performed by the interns with 1:1 faculty evaluation utilizing a skills checklist. The competency in skills included preparation, procedure, and postprocedural concerns. The checklists were based on the review in lecture. Skills were continually practiced without penalty until the procedure was correctly performed. Feedback on intern performance supported their skills development. Participants submitted post-project METs after completing orientation week.
Results
Descriptive Statistics
Descriptive statistics were identified by tallying pre-and postintervention questionnaire responses and converting them into percentages (see Table 1).
Quantitative Data
Quantitative data was scored using means, standard deviations (SD), and standard error of the mean (SEM). Two-sample paired tailed t test analysis of the differences between pre- and postintervention questionnaire scores were compared to establish whether clinical knowledge improved following the intervention. Comparing the outcome questionnaire differences between groups for pre/postintervention, the paired t test results showed the two-tailed p value equals 0.0022, which is strongly statistically significant. See Table 2.
In a safe, controlled simulation environment, students can make errors without fear of harming patients or of retribution.
Statistical Analysis of MET Results
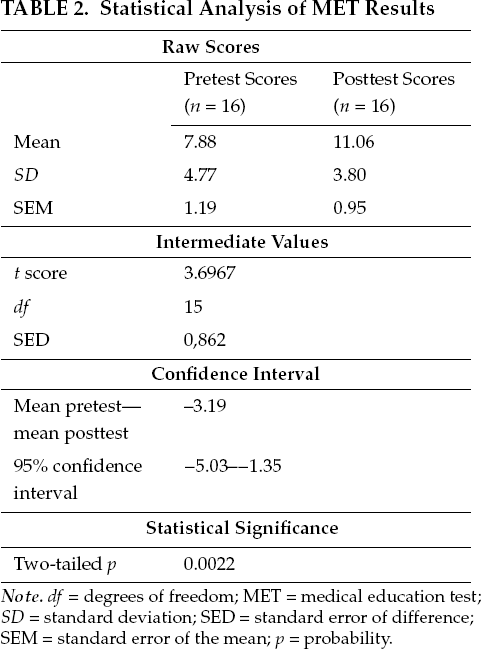
Note. df = degrees of freedom; MET = medical education test; SD = standard deviation; SED = standard error of difference; SEM = standard error of the mean; p = probability.
Students ‘initial MET questionnaire results were deficient in understanding basic concepts and skill techniques. Didactic lecture followed by clinical lab sought to connect information, utilizing simulation to immediately develop and apply hands-on procedural skills learning instead of gradually learning on the job. Training with equipment and supplies for tasks such as NG intubation, venipuncture, urinary catheterization, and IV pump management and IV preparation were valuable for becoming adept with these skills. Results on the MET postintervention questionnaires indicated marked improvement, with significantly higher scores and skills knowledge base. Students ‘evaluations of the program were positive: they verbalized that the lecture combined with the hands-on training improved their skills understanding, technique, and proficiency, increasing their confidence level and preparing them to provide quality care.
Discussion
The transition from medical student to intern can be challenging and intimidating. Factual knowledge learned in medical school now must be integrated with clinical performance. Simulation can be used as a supplement but not as a substitute for clinical training (Laschinger et al., 2008). Strategizing realistic simulation to enhance clinical education is vital (Cant & Cooper, 2010; Issenberg et al., 2005; Maran & Glavin, 2003).
Of the 16 questions on the MET, all but one showed improvement in scores after the intervention. The question matching various colored tubes with the appropriate blood tests showed the lowest score, with no improvement postintervention. Scores for disposal of PPE were also low, pre- and postintervention. There were no skills lab stations for identification of blood tubes and for PPE, although these areas were reviewed in didactic lecture. Perhaps stations to practice and reinforce learning about blood tubes and PPE would have helped improve scores in these areas. The highest scores in pre- and postintervention were for questions associated with ABG sampling and interpretation.
Limitations
This orientation was conducted at one hospital for 1 day with one group of 14 new interns. The nurse educators were a clinical faculty member and a simulation director. The study may have had different findings if several lecturers, clinical faculty, simulation laboratory instructors, and a larger group of medical students took part. The data results are pre-and post-single intervention. Three independent variables that were traditionally deficient in medical education were included in this program: teaching by nurse educators instead of doctors; hand-on practice in the simulation lab versus no opportunity to practice; and a structured curriculum purposefully designed by nurse educators with interprofessional collaboration versus no formal curriculum. Any of these three variables could have had a major impact on the results.
Implications
The findings of this study demonstrated the need to educate graduate medical students in clinical skills at the beginning of internship. This simulation lab is not ordinarily used as a routine part of orientation for new interns to learn clinical skills taught by any professional. A didactic lecture about clinical competencies followed by actively applying those clinical competencies during simulation lab linked theory to practice. In a safe and controlled environment, students can make errors without fear of harming patients or of retribution.
Leading an orientation for interns introduces the nurse as a partner in interprofessional collaboration.
Further research about novice intern orientation to clinical skills could involve a randomized controlled study. One group would be taught by nurses with their developed curriculum and another group taught by doctors with their own developed curriculum. Both groups would use the same assessment tool. Both groups would be equally familiar with using the same simulation lab equipment and both would use the same assessment tool.
Conclusion
The goal of this project was to determine the effectiveness of a 1-day clinical skills intervention lead by nurse educators. Interprofessional teamwork between medical school faculty and nurse educators resulted in a curriculum with didactic lecture and simulation lab for clinical skills practice.
Interns achieved clinical competencies and witnessed interprofessional teamwork. The respectful professional relationship between the chief resident and the nurse educators demonstrated the value each placed on the others ‘specialties. Recognizing nurse educators as clinical experts supporting intern training established a foundation for collegial relationships. At this formidable stage in the new interns ‘medical education, acknowledging each health-care member for their valuable contribution will transform the traditional medical hierarchy to reflect interdependence. Integrating health-care professionals to provide health care as a cooperative measure, and not in silos, will promote strong teams ensuring optimal patient care.
Footnotes
Disclosure. The authors have no relevant financial interest or affiliations with any commercial interests related to the subjects discussed within this article.
Funding. The author(s) received no specific grant or financial support for the research, authorship, and/or publication of this article.
Maryanne Barra, DNR RN, FNP-C, (she/her), is an associate professor at Seton Hall University College of Nursing in South Orange, New Jersey. As a family nurse practitioner, she has worked in the Battered Women's Shelter, College Health, Hospice, and Assisted Living. She is an experienced educator in med-surg, maternal/child, community, acute, chronic, critical, and long-term care in the undergraduate and graduate programs.
Samantha Singh Hernandez, MSN, RN, MSW, LMSW, (she/her), is director of the Regional Perinatal Simulation Center at RWJBarnabas Health in Livingston, New Jersey. She has integrated simulation education across multiprofessional health-care education in clinical, nonclinical, and academic settings. Focusing on the use of simulation with debriefing, assessment, and self-awareness, she has designed, implemented, evaluated, and standardized educational programs for staff development.
Janet Czermak, DNR RN, APN-BC, (she/her), is an associate professor in the Graduate Nursing Program at the College of Mount Saint Vincent in Chatham, New Jersey. Her areas of expertise are med-surg, critical care, pharmacology, and pathophysiology. Dr. Czermak developed several online pharmacology courses and modules. She authored a pharmacology textbook, study guide, and numerous book chapters.