
Abstract
A ruptured splanchnic artery aneurysm is a rare clinical entity. Its diagnosis requires a high index of clinical suspicion, and management usually requires a multidisciplinary approach. We present a case of ruptured true pancreaticoduodenal artery aneurysm in an 83-year-old woman who was initially treated with transcatheter embolization, but it failed to arrest the bleeding, and she subsequently required laparotomy and surgical ligation. The clinical course and management are discussed with a review of the literature.
True aneurysms of the pancreaticoduodenal artery (PDA) are rare and account for only 2% of over 3,000 splanchnic aneurysms reported since 1960. 1 False PDA aneurysms as a result of pancreatitis or trauma are more common than true degenerative aneurysms. The first true PDA aneurysm was described by Ferguson in 1895, 2 and since then, about 100 cases have been described in the literature, mostly as individual case reports. The natural history and best management options for this rare condition remain ill defined. In this report, a case of ruptured PDA aneurysm is presented and the management options are reviewed.
Case Report
An 83-year-old woman was admitted to the dermatology unit for the treatment of deteriorating plaque psoriasis. She had no significant medical history except the psoriasis and one episode of deep venous thrombosis 8 years ago. There was no history of abdominal trauma or pancreatitis. She smoked 10 cigarettes per day.
Two weeks after admission, she suddenly collapsed in the ward and was attended immediately by the cardiac arrest team. She was semiconscious and hypotensive (blood pressure 88/56 mm Hg) but was breathing spontaneously. She regained consciousness following a small bolus of intravenous fluid replacement and oxygen therapy and complained of severe backache. On examination, a tender pulsatile abdominal mass was palpable and a clinical diagnosis of ruptured abdominal aortic aneurysm was made. An urgent computed tomographic (CT) scan demonstrated no evidence of an aortoiliac or splenic artery aneurysm. There was a large intraperitoneal hematoma at the base of the small bowel mesentery and free fluid in the upper abdomen (Figure 1). The exact source of the bleeding could not be identified. She remained hemodynamically stable and underwent urgent angiography.
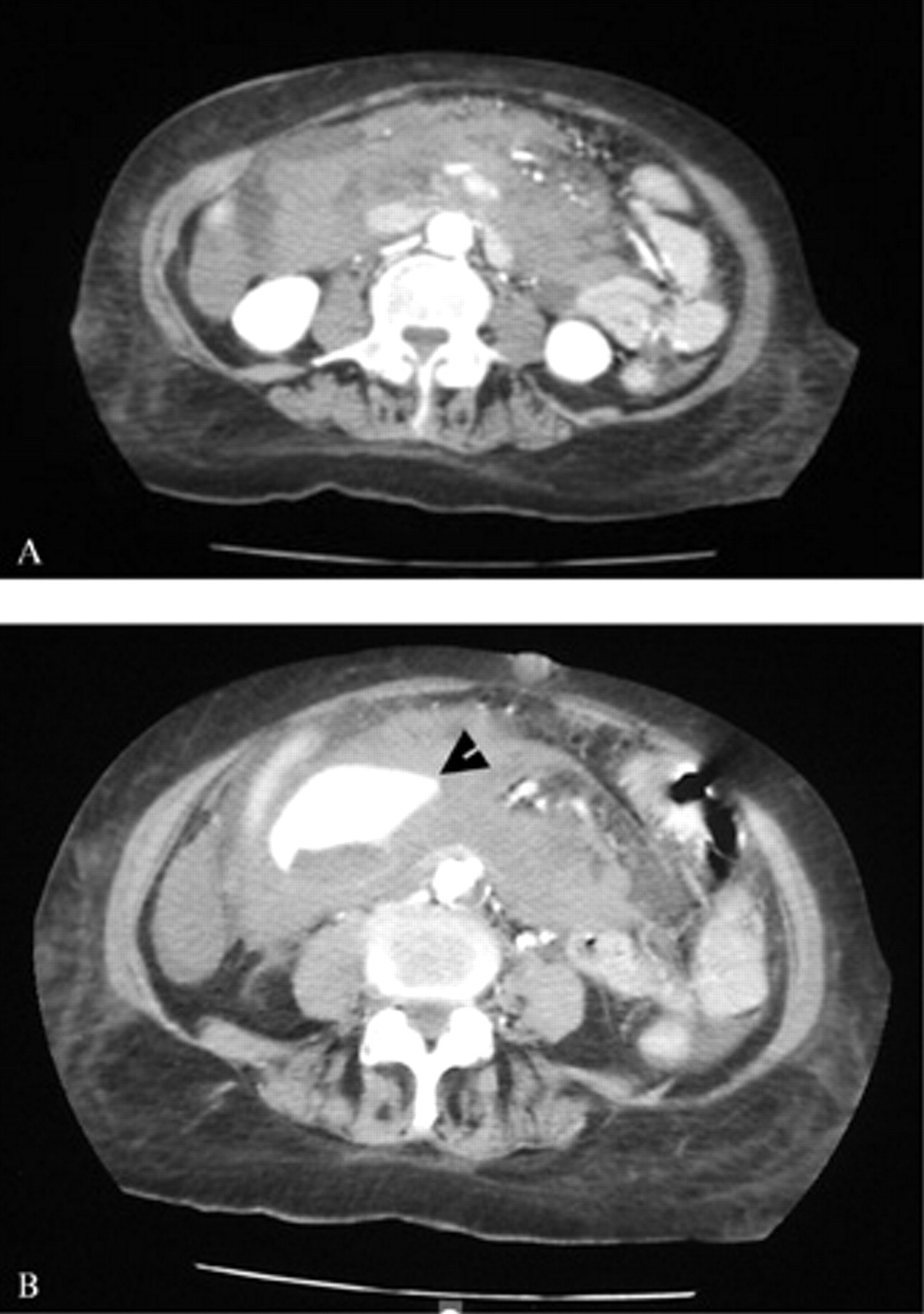
A, Transverse computed tomographic (CT) scan of the abdomen showing a large hematoma in the peritoneal cavity. B, A delayed transverse CT scan of the abdomen demonstrating extravasation of intravenous contrast into the peritoneal cavity suggestive of active hemorrhage (arrow).
The superior mesenteric artery (SMA) was catheterized without difficulty via a right transfemoral approach. An aneurysm was demonstrated in the superior PDA with evidence of active bleeding (Figure 2). Three fibered platinum coils (Boston Scientific, Boston Scientific Cork Ltd., Cork, Ireland) were placed through a microcatheter into the superior PDA, just proximal to the aneurysm. Further imaging showed no flow of contrast into the aneurysm (Figure 3). At this stage, the patient remained hemodynamically stable; therefore, embolization of the PDA distal to the aneurysm was not considered. The patient was transferred to the high dependency unit (HDU) for intensive monitoring.
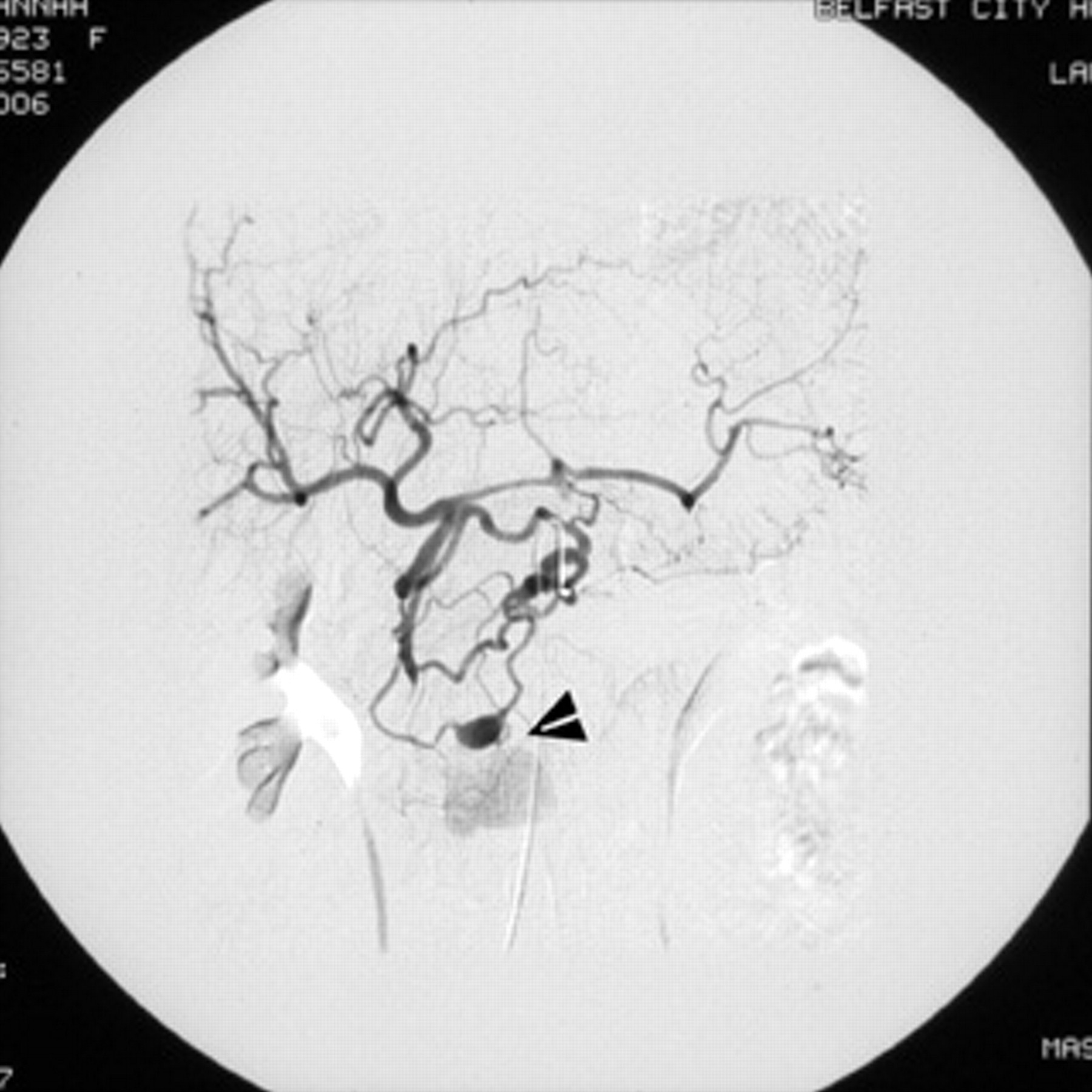
Mesenteric angiogram with selective superior mesenteric artery catheterization demonstrating active bleeding arising from an aneurysm of the pancreaticoduodenal artery (arrow).
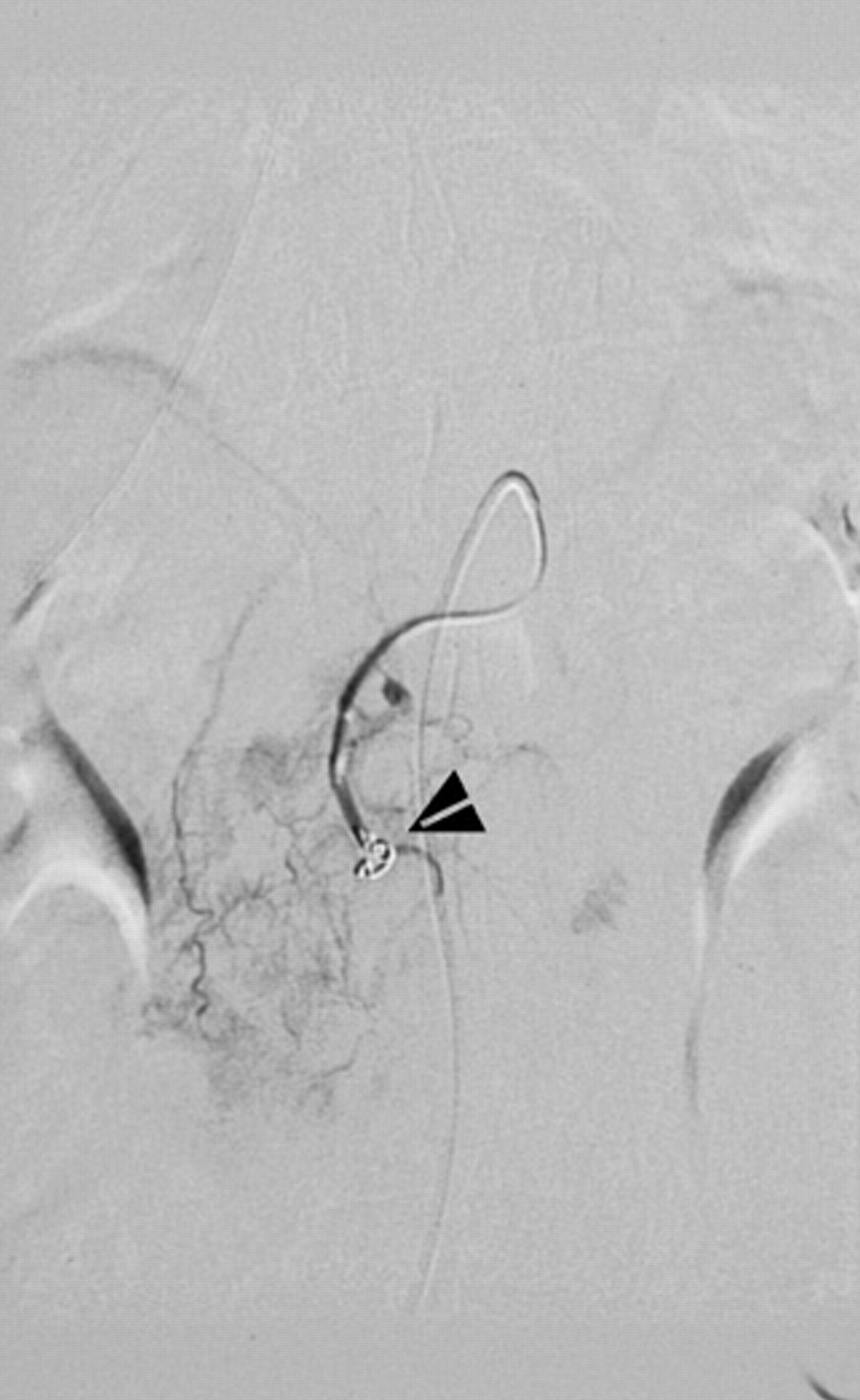
Coil embolization of the pancreaticoduodenal artery aneurysm (arrow).
Fifteen minutes after admission to the HDU, she deteriorated and became tachycardic and hypotensive. An emergency laparotomy demonstrated free intraperitoneal blood (> 3 L), and a large hematoma was identified in the small bowel mesentery. The anatomy adjacent to this area was extremely distorted. However, active bleeding was identified from an aneurysmal cavity deep in the hematoma in an area that was supplied by the PDA. The bleeding points were oversewn, and the raw hematoma was treated with a combination of hemostatic agents of Quixil (ORMIX biopharmaceuticals S.A., St. Genese, Belgium) and Surgicel (Johnson and Johnson MEDICAL Limited, Gargrave, North Yorkshire, UK). The small bowel and colon were examined and remained well perfused. During the procedure, eight units of packed red cells and three units of fresh frozen plasma were transfused. She remained in the intensive care unit for 2 days and was subsequently transferred to the ward.
Postoperatively, her oral intake was poor, and she complained of increasing abdominal fullness and developed a palpable mass in the epigastrium. Her amylase and liver function tests were normal, and a repeat CT scan demonstrated evidence of gastric outlet obstruction as a result of compression from a liquefying hematoma but no active bleeding from the oversewn area. Successful percutaneous drainage of hematoma was performed, and she remained well at 3 months following her initial surgery.
Discussion
A PDA aneurysm is a rare but clinically significant lesion. Most PDA aneurysms are false aneurysms developed secondary to either an inflammatory process, such as pancreatitis and endocarditis with mycotic embolization, or trauma, including iatrogenic injury. True degenerative aneurysms of the PDA are much less common and are associated with local turbulence in blood flow. An association between a PDA aneurysm and celiac axis stenosis was first described by Sutton and Lawton. 3 They suggested that the aneurysm formation was secondary to a state of high blood flow in the PDA as a result of enhanced collateral flow from the SMA in the presence of celiac stenosis or occlusion. The celiac axis could be occluded as a result of compression from median arcuate ligament, atheroma, or fibromuscular dysplasia. An association between an inferior PDA aneurysm and congenital absence of the celiac trunk was described in a recent case report by Armstrong and Franklin. 4
In about 50% of cases, atherosclerotic degeneration is a major cause of aneurysm formation in the PDA. 5 In addition, 24% of patients with PDA aneurysms have associated aneurysms in other locations, including renal, aortic, and intracranial arteries, indicating a generalized atherosclerotic degeneration. Our case probably represents a true isolated degenerative PDA aneurysm as there was no preceding history of any abdominal complaints. The celiac artery was demonstrated to be normal in the urgent mesenteric angiography, and there was no evidence of other aneurysms on the CT scan.
Most PDA aneurysms remain asymptomatic and are discovered incidentally on a CT scan or angiogram during the course of investigation of an unrelated illness. However, some aneurysms are symptomatic. Abdominal pain is the commonest initial symptom and is reported in 52% of patients. 6 Other presentations include jaundice, gastric outlet obstruction, and pulsatile mass. 7 The significance of the aneurysm lies in its potential for rupture resulting in life-threatening hemorrhage, as demonstrated in this case report. Some 62% of PDA aneurysms remain undiscovered until they present with catastrophic intra-abdominal hemorrhage, carrying a mortality rate of 21%. 6 Neschis and colleagues found no correlation between the size of the true PDA aneurysm and its propensity to rupture. 8 In addition, 17.6% of ruptured PDA aneurysms were ≤ 1 cm.
In recent years, transcatheter arterial embolization (TAE) of PDA aneurysms has been considered the initial treatment for both ruptured and nonruptured aneurysms. Endovascular treatment includes obliteration of the aneurysm using a range of embolization agents (Gelfoam, intravascular coils, ethanol sclerosant, and detachable balloons). In most cases, visceral revascularization is not required. However, if aneurysm occlusion compromises the circulation to the liver, celiac revascularization is recommended by either an endovascular or an open technique prior to embolization of the PDA aneurysm. 9 Despite its claimed safety and efficacy, TAE is not always successful, and in an elective setting, percutaneous thrombin injection under CT guidance can be a successful alternative. 10 However, in case of a ruptured aneurysm, emergency surgery with ligation or oversewing of the aneurysm is essential after a failed attempt at TAE. Visceral revascularization in the form of celiac angioplasty, aortohepatic bypass, or reimplantation of the PDA is required only in case of visceral ischemia. 11
This case highlights the significance of ruptured PDA aneurysm as a differential diagnosis in sudden unexpected hemodynamic instability in elderly patients. It also demonstrates that transcatheter coil embolization of the ruptured aneurysm may be initially successful, but intensive monitoring following treatment is required. Further hemodynamic instability requires a prompt decision for surgical treatment, which could be lifesaving in this rare but potentially fatal condition.
Footnotes
Acknowledgment
We thank Mr. Adrian Knipe, Department of Medical Illustration, Belfast City Hospital, for his assistance in the production of the technical figures.