
Abstract
Vertical groin incisions (VGIs) have been used to access femoral vessels, but reports allude to wound complications. Our aim was to compare VGI with transverse groin incision (TGI) for femoral artery exposure. Over a 5-year interval, 196 patients with 284 femoral artery exposures for supra- and infrainguinal procedures were studied. Primary endpoints were surgical skin site wound infection, seroma, haematoma formation, and major lower limb amputation. Secondary endpoints were graft patency, wound paresthesias, and length of hospital stay. There were 160 TGIs and 124 VGIs. The demographics and risk factor profile were not statistically different between groups. Seroma developed in 4.4% of TGIs and 13.7% of VGIs (p = .005). The complicated skin and soft tissue infection rate was five times greater with VGI (p = .001). The VGI group had a significantly higher rate of major amputation (p = .0005). Significantly higher graft failure rates were observed in the VGI group (p = .011). No paresthesia was reported in any TGI wound. The mean hospital stay was also significantly shorter in the TGI group (p = .006). The study data support and expound on the theory that an alternative incision to VGI offers lower short- and long-term morbidity. Our findings sustain the selection of the TGI in femoral artery surgery for both supra- and infrainguinal procedures without compromise of vessel exposure.
The wound infection rate in vascular surgery is used as an auditing tool to evaluate preventive measures and surgical technique. 1 Traditionally, groin incisions to gain access to the femoral artery have been via a vertical or an oblique approach. 2–4 These techniques, although widely described, carry significant morbidities, such as infection and lymphatic complications. Such potentially catastrophic complications have been attributed to transection of lymphatic vessels and traversing through the moist groin skin crease. 5 An alternative technique is therefore required to avoid such adverse events and prevent any devastating sequelae.
The aim of this study was to compare transverse groin incision (TGI) against the vertical groin incision (VGI) for femoral artery access. Primary end points were surgical skin site wound infection, seroma, hematoma formation, and major lower limb amputation. Secondary end points were graft patency, wound paresthesias, and length of hospital stay.
Materials and Methods
Clinical Study
A 5-year longitudinal comparative analysis was undertaken of groin dissections, for vascular reconstructive surgery, within a single vascular unit.
Surgical Procedures
Patients included in this study underwent infrainguinal bypass surgery, aortobifemoral bypass surgery for occlusive disease, and endovascular aortic aneurysm repair (EVAR) (Figure 1). Patients were excluded if they had undergone previous groin dissection, if they were immunocompromised, or if their notes were incomplete. In accordance with these criteria, 196 patients required femoral artery access for both vascular and endovascular procedures (Table 1). Two senior surgeons performed the TGI and VGI, respectively.
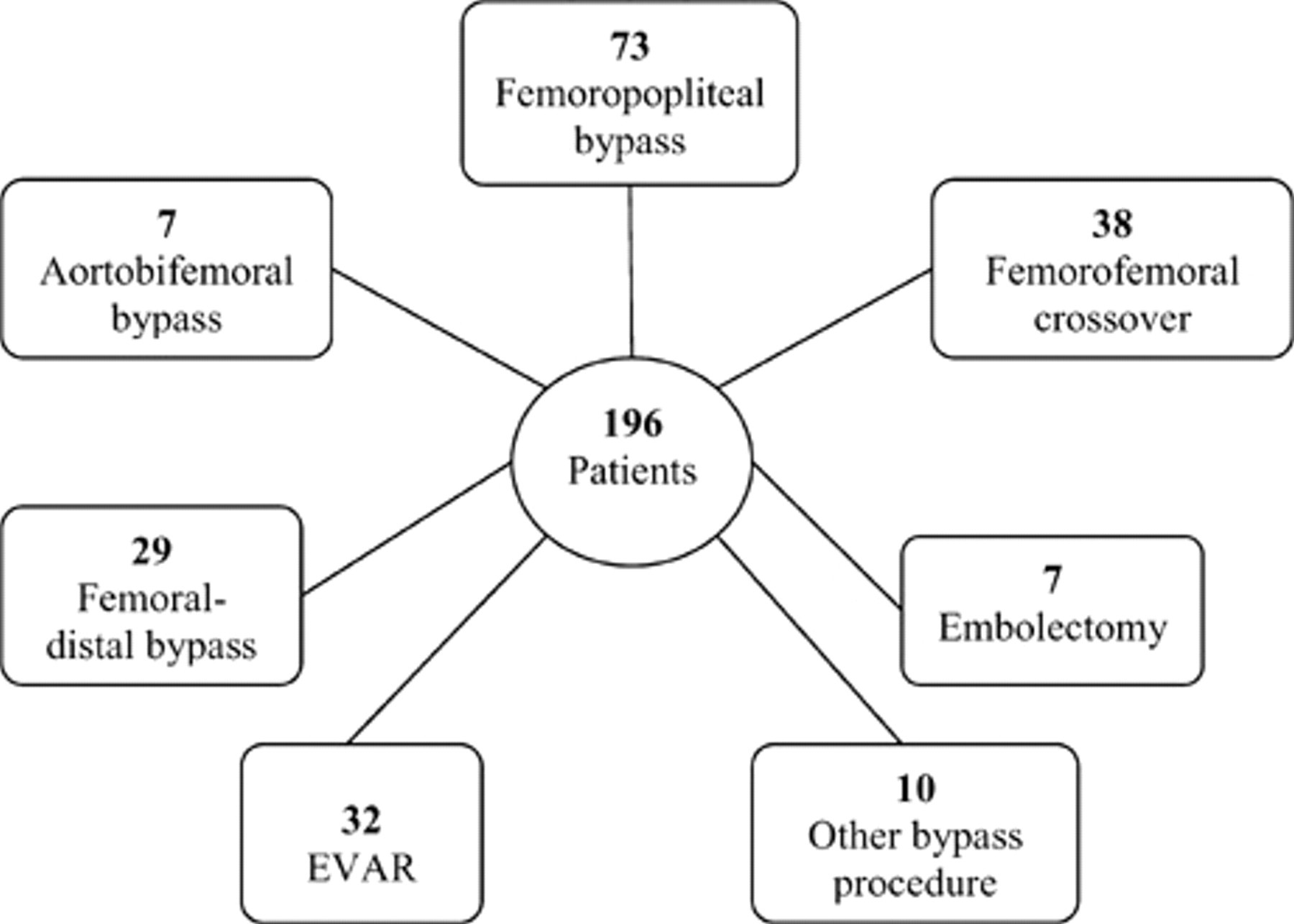
Supra- and infrainguinal procedures requiring femoral artery access. EVAR = endovascular aneurysm repair.
Patient Demographics
Skin preparation, with povidone-iodine solution, was identical in both the TGI and VGI groups. The antibiotic regimen did not differ between the two groups. Prophylactic therapy consisted of 1.2 g of intravenous Augmentin (clavulanic acid [K+ salt] 200 mg, amoxicillin [Na+ salt] 1 g) given at the time of anesthetic induction and continued for 48 hours postoperatively. No antibiotic irrigations were used for the wounds. The TGI used a 3.5 to 5.0 cm incision centered to the midinguinal point and 2 cm superiorly in the skin crease (Figure 2). Tissues with lymph nodes are mobilized from the lateral aspect medially, using electrocautery, to expose the femoral artery (Figure 3). This technique allowed clear identification of the lymphatics and lymph nodes and thus their preservation. Following the supra- or infrainguinal vascular procedure, both wound types were closed with interrupted inverted vertical absorbable monofilament (3-0 Monocryl) sutures to the subcutaneous tissues and a continuous absorbable subcuticular suture (4-0 Monocryl). Patients were routinely ambulated on day 1 postoperatively as tolerated.
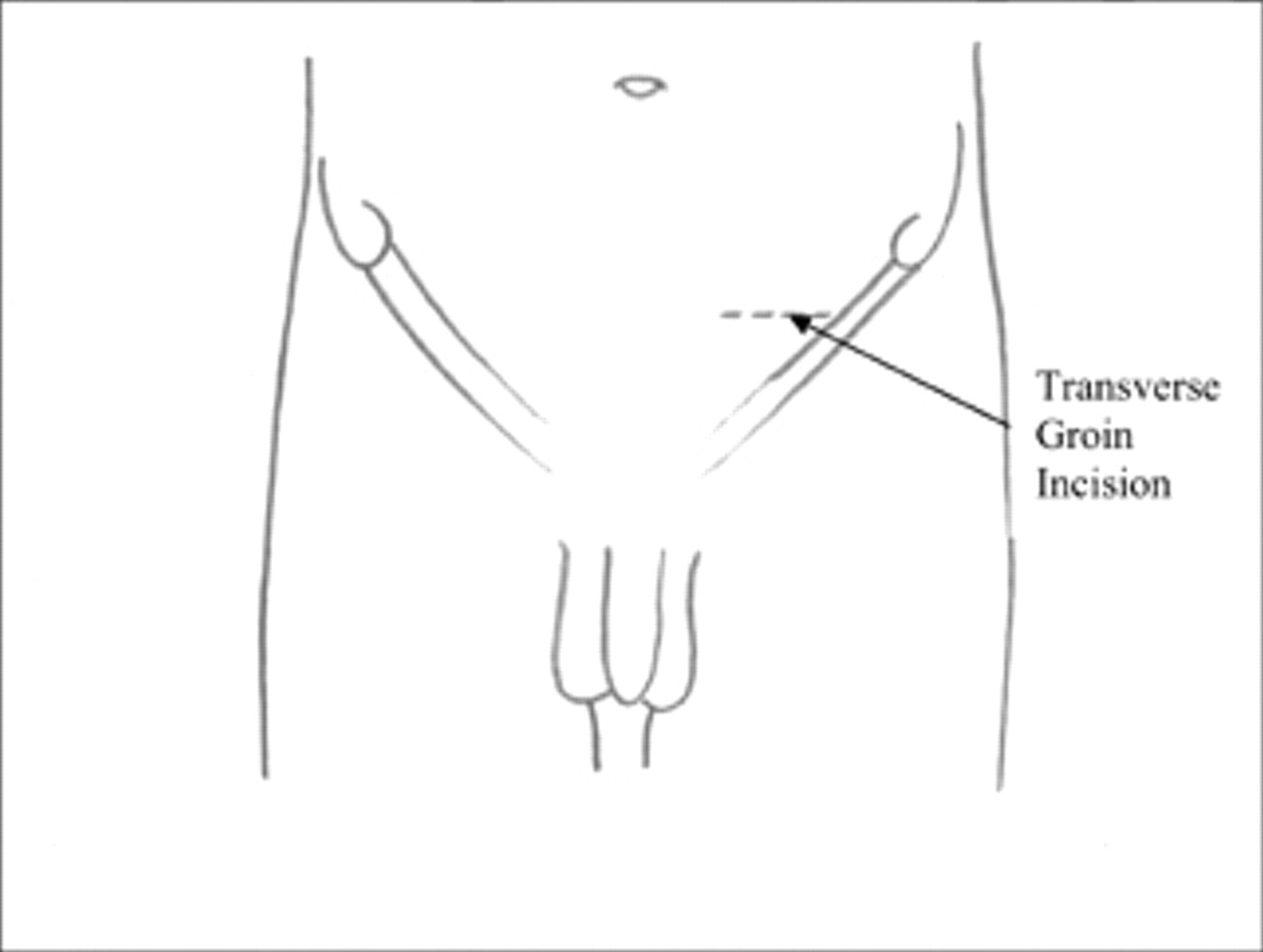
Site of transverse groin incision.
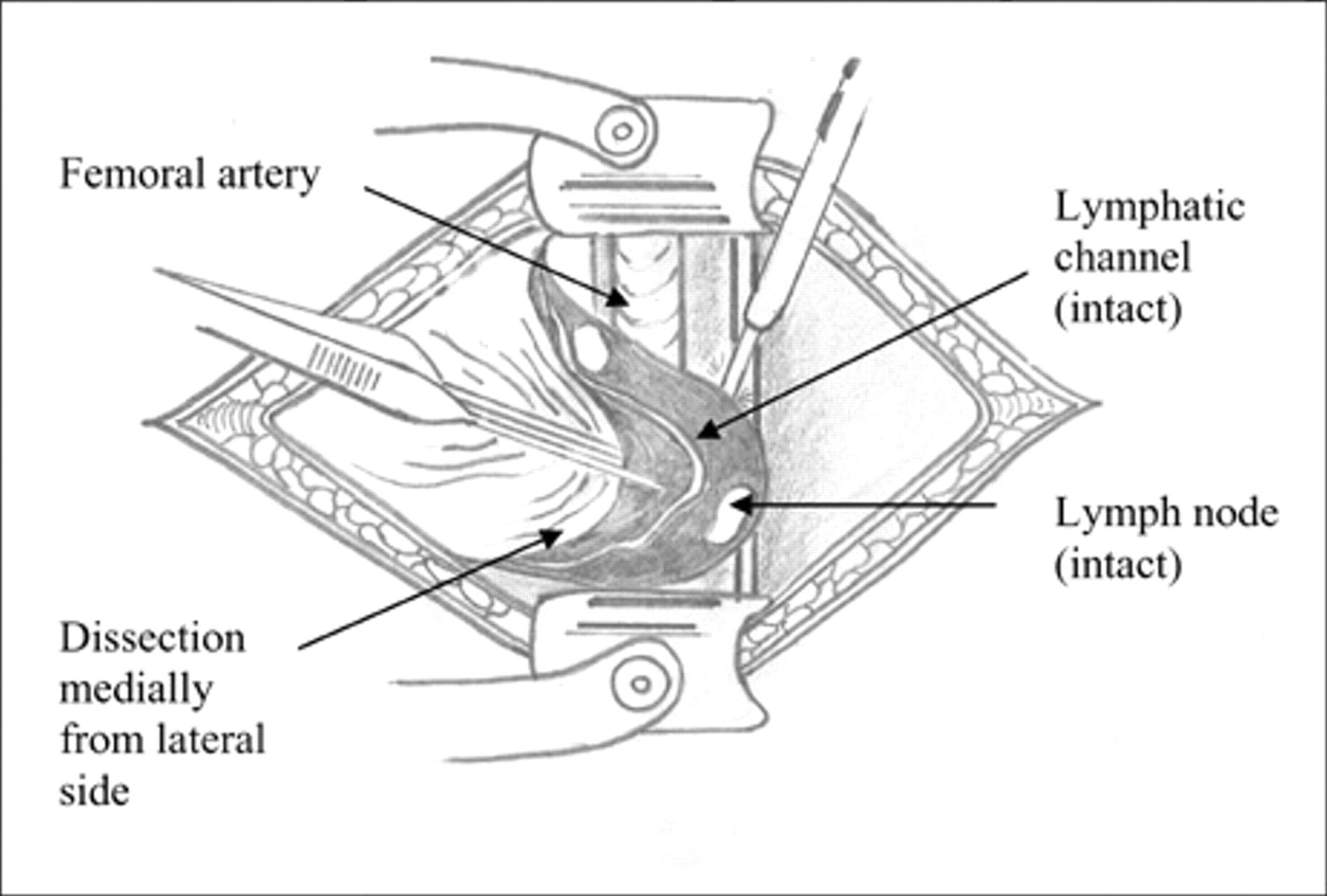
Dissection technique.
Method
Data were acquired from a prospectively maintained VascuBase system (Consensus Medical, Vancouver, BC), which maintains a database of patient demographics and vascular laboratory scanning records. Data collected were entered into JMP IN (SAS Institute, Cary, NC, USA) statistical software. Basic statistics were performed using Pearson goodness of fit chi-square analysis or Fisher exact test when applicable.
Wound infections were identified by a senior member of the vascular surgical unit and graded according to the Szilagyi classification. When only the dermis was affected, the infection was classified as grade I; in grade II infections, the involvement extended into the subcutaneous region but did not invade the arterial implant; in the instances called grade III, the arterial implant proper was involved in the infection. 6 Graft occlusion, major amputations, wound paresthesias, and postoperative stay rates were analyzed for significance.
Results
Wound Infection
Twenty wound infections (16.1%) developed in the VGI group in comparison with 5 (3.1%) in the TGI cohort (p = .0001) (Table 2). Ten percent of these VGI infections were Szilagyi grade III, involving graft material and requiring initial intravenous antibiotic therapy, with subsequent tissue loss amputation procedures. None of the infections observed within the TGI group were Szilagyi grade III (p = .190) (Table 3).
Comparison between Transverse and Vertical Groin Incision Outcomes
Comparison of Wound Infections between Transverse and Vertical Groin Incisions
Seroma Formation
Seventeen (13.7%) seromas were observed in the VGI group compared with 7 (4.4%) in the TGI group (p = .005) (see Table 2).
Major Amputation
For any revascularization procedure, limb salvage is always a primary end point. Two (1.3%) amputations were performed following bypasses using the TGI surgery, whereas 13 (10.5%) subsequent amputations were required following the original VGI surgery (see Table 2).
Postoperative Stay
The duration of inpatient stay following surgery was significantly longer in the VGI group (p = .006), with an average rate of 24.54 days compared with 13.12 days in the TGI group (see Table 2).
Hematoma Formation
Nine hematomas were observed in the VGI group, in contrast to 6 in the TGI group (p = .19) (see Table 2).
Graft Occlusion
There was a significantly higher rate of subsequent graft occlusion in the VGI group. There were 18 grafts (7.3%) affected within the VGI setting compared with 9 (5.6%) compromised grafts following TGI (p = .011) (see Table 2).
Wound Paresthesias
No paresthesiae were reported by any patients within the TGI group, whereas eight patients reported altered sensation within the wounds of the VGI (p = .0012) (see Table 2).
Discussion
The TGI technique, for femoral artery access, has significantly better technical and clinical outcome, in our experience, compared with the traditionally adopted vertical technique. The incision and subsequent mobilization of subcutaneous tissues allow clear identification of lymphatic vessels. With these lymphatics protected at an early stage of the reconstructive procedure, the results demonstrate that seroma (4% TGI vs 14% VGI; p = .005) and wound infection (3% TGI vs 16% VGI; p = .0001) rates are significantly improved. Previous evidence of patients undergoing lower extremity arterial bypass procedures has wound complication rates as high as 17 to 44%, with the VGI contributing significantly to this figure. 7,8 Roberts and colleagues reported lymphatic complications in vertical and oblique groin incisions after femoral revascularization procedures. 9
The oblique incision preferred by Chuter and colleagues was adopted initially in an attempt to avoid the high incidence of wound necrosis, lymphatic leak, and wound infection that they had experienced when exposing the femoral artery through the usual vertical incision. 2 The incision lies inferior to the TGI, with the dissection being performed along the line of the incision. They reported no wound complications in over 30 cases of endovascular repair. However, incidences of hematoma formation were not reported, a complication that was lower within the TGI group of our study (see Table 2). Caiati and colleagues reported promising results with the same technique in 100 patients receiving endovascular aortic stent placement. 3 Of 176 groin incisions, they reported an incidence of 2.8% lymphatic wound infections. The reason for this low incidence of lymphatic complications was deemed to be partly due to changing the direction of dissection from oblique to vertical below the skin, along with careful ligation of small lymphatic branches. This was in a single operative group and needs to be reflected on with the evidence of Schwarz and colleagues, who demonstrated that of 98 infrainguinal bypass procedures, 31% developed wound complications, with 4% localizing to the groin. 10 In a study solely looking at EVARs, 39 patients underwent unilateral VGIs to gain access to the femoral artery. 11 In this study, there were seven complications (18%) involving the vertical incision. These complications varied from superficial cellulitis to one reported case of lymphocutaneous fistula. The advantages of the TGI with the oblique approach reported by Chuter and colleagues and Caiati and colleagues are the convenience of this incision in obese patients, partly owing to avoidance of excessive pannus, and a tension-free closure. 2,3
van Himbeeck and colleagues reported an overall incidence of wound complications, including hematoma and seroma, following arterial reconstruction as 13%. 1 Their definition of wound infection was equivalent to Szilagyi grade II infection. A similar, but slightly lower, grade II infection rate was seen with VGIs in our study (10%). This contrasts markedly with less than 2% Szilagyi grade II infections seen in the TGI cohort of our study (see Table 3). The increased incidence of infection in the VGI group with recognized subsequent thrombosis of the graft is reflected in the higher rate of occlusion within this cohort (7.3% VGI compared with 5.6% TGI; p = .011).
Further evidence supports a move away from the traditional VGI. In a study of abdominal aortic aneurysm stent graft repairs, using an oblique incision, a low wound complication rate (4.7% paresthesias and 2.38% wound seroma) led the authors to conclude that their data supported this alternative to the VGI. 4 However, in their study, the oblique incision was found to be too low an approach. Such a problem was not encountered and is therefore not reported in our data in any of the EVAR procedures. These rates of paresthesias contrast to a zero incidence within our TGI cohort, related to the mobilization of tissue with lymph nodes from the lateral to medial aspect, far away from the femoral nerve. The TGI approach allowed an excellent operative field, and, in particular regarding groin profundaplasty, no difficulty was encountered in accessing the third part of the profunda artery.
The cost of such decreased morbidity is experienced not only by the patient but also the health care provider as affected patients have been found to have a significantly prolonged hospital stay (p = .006) (see Table 2). Extended hospital stay is most often related to intravenous antibiotics requirements, 12 and we noted that the west of Ireland demographic is a graying population, in which poor social circumstances are encountered, along with a scarcity of step-down facilities such as convalescence or nursing homes. There is always the possibility of more devastating complications requiring more aggressive therapy, such as drainage or excision and muscle flap coverage. 13 Only one of the four patients with a lymphatic complication in the series of Caiati and colleagues did not resolve with conservative treatment. 3 Shermak and colleagues reported the incidence of groin lymphatic complications following arterial revascularization procedures involving the groin. 13 They alluded to the high percentage of affected patients receiving antibiotics, anticoagulation, or antiplatelet therapy when they presented with symptoms of lymphatic disruption, often 14 or more days following the initial arterial revascularization procedure.
It has been proposed that owing to a difference in oxygenation of the skin on the lateral and medial aspects of the VGI reported by Raza and colleagues, 14 the oblique incision may be less disruptive to the blood supply of the wound. 3 This theory would hold true for the TGI technique.
It remains to be studied whether the approach of TGI is as effective in accessing the previously dissected groin. However, anecdotal evidence from our high deliberate practice volume center suggests that TGI is a preferable incision even in the setting of re-do groin exposures, regardless of what type the original incision was.
The results in our study dispute previous evidence suggesting that surgical femoral artery exposure adds little morbidity to the endovascular repair of abdominal aortic aneurysms. 15 The patient profiles of Slappy and colleagues were only those who underwent EVAR surgery. 15 No infrainguinal procedures were performed in this study group, and no comparative analysis was performed to an alternative incision. Once again, this is of importance when we consider the results of Schwarz and colleagues. 10 Despite an overall wound infection rate of 2%, Slappy and colleagues demonstrated that the VGI was associated with 14.6% of wound fluid collections at 1 month, 2.6% of which were still present at the 6-month interval. This correlates well with our data of seroma formation within the VGI group (13.7%) and is in stark contrast to an overall seroma formation rate of 4.4% within the TGI group.
Conclusions
Compared with VGI, TGI has a lower propensity to disruption of lymphatic vessels with less complicated skin and soft tissue infection and a shorter hospital stay. The study data support and expound on the theory that an alternative incision to VGI offers a lower short- and long-term morbidity. Our findings sustain the selection of the TGI in femoral artery surgery for both supra- and infrainguinal procedures without concession of vessel exposure.