
Abstract
Purpose
To determine the associations between field-collected surrogates of adiposity and concentrations of resistin, tumor necrosis factor α (TNF-α), interleukin-6 (IL-6), and adiponectin in youth.
Methods
Cross-sectional data from 60 normal weight and 60 overweight adolescents, ages 10-14 years, were retrospectively examined. Body mass index (BMI) percentile, sum of subscapular and triceps skinfolds (SSF), and waist circumference (WC) were used to classify weight status (BMI) or adiposity (SSF and WC). Percentiles for each surrogate were used for comparison groups. Fasting TNF-α, IL-6, resistin, and adiponectin concentrations were measured in plasma.
Results
Multiple regression models, controlling for sex and ethnicity, indicated that TNF-α was associated with BMI percentile (R2 = 0.107, P < 0.05) and SSF (R2 = 0.085, P < 0.05), whereas resistin was associated with SSF (R2 = 0.118, P < 0.05). Adiponectin was associated with all 3 adiposity markers: BMI percentile (R2 = 0.298, P < 0.05), SSF (R2 = 0.297, P < 0.05), and waist (R2 = 0.278, P < 0.05). Analyses of variance indicated higher TNF-α and lower adiponectin concentrations in youth with a BMI higher than the 95th percentile (P = 0.014; P < 0.001) or SSF higher than the 95th percentile (P = 0.025; P < 0.001). Youth with WC higher than the 90th percentile had higher resistin (P = 0.029), higher IL-6 (P = 0.028), and lower adiponectin (P < 0.001) concentrations.
Conclusions
Of the 3 surrogates examined, differences in cytokine concentrations were mostly observed in youth who had WC percentiles higher than the 90th percentiles versus WC lower than the 75th percentiles. Alternatively, from the multiple-regression models SSF, an estimate of subcutaneous adiposity was the surrogate most consistently related to all cytokines, although the degrees of associations were low. The results suggest that although some surrogates were more strongly associated to certain cytokines, WC and SSF seemed more closely associated with cytokines than a BMI percentile indicating obesity.
Introduction
In children and adults, the association between obesity and the presence of cardiovascular disease risk factors and insulin resistance is well established.1,2 However, the mechanisms relating obesity to attendant comorbidities of cardiovascular disease or insulin resistance remain unclear. One of several proposed hypotheses is that adipose tissue acts as a secretory gland releasing hormones and cytokines with proinflammatory or anti-inflammatory activity. 3 These cytokines in turn affect either glucose transport or utilization or endothelial function in a negative4–7 or positive way. 8 Tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), and resistin are positively associated with insulin resistance4–6 and cardiovascular disease, 7 whereas adiponectin is negatively associated with both morbidities. 8
In adults, these cytokines are correlated to specific measures of adiposity with some of them showing a sex dimorphism. 9 Circulating TNF-α, IL-6, and adiponectin concentrations, although mostly associated with visceral adiposity,10,11 are also associated with body mass index (BMI). 11 In contrast, the association between resistin and adiposity is not clear, as some studies in adults found positive associations between resistin and measures of adiposity,9,12 whereas others found no association.13,14
In youth, individual studies have assessed the association between some of these cytokines and subcutaneous, visceral, or total body fat.15–20 However, no published study in youth has examined the relationship between all 4 of these cytokines and several different surrogate markers of adiposity that are routinely used in clinical or field settings. Further delineation of the associations between these surrogate markers of adiposity and inflammatory mediators of obesity has the potential to support use of certain surrogate markers over the others in clinical practice. Thus, the purpose of this study was 2-fold: (1) to determine which surrogate marker for adiposity was associated with most the cytokines (resistin, TNF-α, IL-6, and adiponectin) and (2) to determine which surrogate better discriminated differences in the concentrations of the cytokines between normal and overweight youth. The surrogate markers for adiposity studied were WC as an estimate of trunk adiposity, SSF as an estimate of subcutaneous adiposity, and BMI percentile as an indicator of weight status.
Methods
Subjects
Data from 120 youth (60 girls and 60 boys), aged 10 to 14 years who participated in the Cardiovascular Health in Children and Youth (CHIC III) Study between 2000 and 2003, were used for this retrospective study. The CHIC III study was a multicohort study focused on cardiovascular risk factors in 1,370 school-aged youth. 21 Potential subjects for this analysis had to be in pubertal developmental stages 2-4, according to a questionnaire that assessed puberty based on growth spurt in height, pubic hair development, skin changes in both boys and girls, facial hair growth and voice change in boys only, and breast development and menarche in girls. 22 In addition, none of the youth had impaired glucose metabolism (fasting glucose levels >5.6 mmol/L). All subjects meeting the prescribed criteria were included in the subject pool. The subject pool was then divided by weight status (BMI <75th percentile and BMI >95th percentile) based on reference data from the Centers for Disease Control. 23 Body mass index percentile was chosen to dichotomize the sample because it is the standard clinical criteria in the USA for determination of weight status. 23 The 75th and the 95th percentile thresholds were chosen to maximize differences in adiposity between the 2 groups, clearly presenting normal and overweight groups. From this initial pool of subjects, a subsample was randomly selected comprised of 60 youth with normal weight (BMI <75th percentile for age and sex) and 60 youth who were overweight (BMI>95th percentile for age and sex). Sixty subjects per group were selected randomly based on their BMI and their sex using the select random cases procedure of the Statistical Package for Social Sciences for Windows (Version 9.0; SPSS, Inc, Chicago, IL). Sixty youth were selected for each group due to considerations of both power calculations and feasibility of study design. Sixty subjects per group was sufficient to detect group differences of 0.4 ng/mL for TNF-α, 0.6 ng/mL for IL-6, 2.1 ng/mL for resistin, and 1.6 mg/mL for adiponectin, with an α = 0.05, β = 0.2, and a power of 80%. The subjects signed an assent, and their parents or guardians signed an informed consent approved by the institutional review board of the Institution. Ethnicity was self-reported.
Adiposity Surrogate Measurements
The 3 adiposity surrogates of interest for this study were BMI, SSF, and WC. As previously stated, BMI percentile was used as an estimate of overall weight status, SSF was used as representative of subcutaneous adiposity, and WC was used as an indicator of trunk adiposity. These surrogates were measured in the school setting within 3 days of blood sampling. The subjects were dressed in shorts and T-shirts with no shoes. Height was measured to the nearest 0.1 cm using a stadiometer (Perspective Enterprises, Kalamazoo, MI), and body mass was obtained in kilograms to the nearest 0.1 kg using an electronic scale (model 5602; Scale-Tronix, Carol Stream, IL). Body mass index was computed using body mass in kilograms divided by height in meters squared (BMI = kg/m2). Triceps and subscapular skinfolds were measured in triplicate using Lange skinfold calipers (Cambridge Scientific Instruments, Cambridge, MD) and following procedures described by the National Health and Nutrition Examination Survey. 24 The sum of the skinfolds (SSF) was calculated from mean measurements of both skinfolds. Waist circumference was measured to the nearest millimeter using a tape measure at just above the uppermost lateral border of the ilium, at the end of normal expiration following the same procedures as in the Third US National Health and Nutrition Examination Survey. 24 The average of 2 consecutive measurements was considered the WC value. Waist circumference measured at this site has been shown to be the one with the highest correlation with trunk fat mass. 25
Blood Sampling and Analyses
Blood samples were obtained at the school using sterile venipuncture technique between 7 and 9 am after an overnight fast. All subjects included in this study were compliant with fasting procedures as verbally verified by on-site research assistants. Blood samples were collected in tubes containing EDTA and immediately centrifuged to obtain plasma. Plasma was aliquoted, maintained in dry ice, and transported to the laboratory where it was kept frozen at −80°C until analyzed. Concentrations of plasma resistin, TNF-α, IL-6, and adiponectin were measured using standard enzyme immunoassay procedures (Linco Research Inc, St. Charles, Mo and R&D Systems, Minneapolis, MN). The resistin assay had a sensitivity of 0.5 ng/mL with intraassay and interassay coefficients of variation of less than 10% and 11.2%, respectively. The adiponectin assay had a limit of sensitivity of 0.78 ng/mL with intraassay and interassay coefficients of variation of less than 10% and 11.6%, respectively. The TNF-α kit had a sensitivity of 0.5 pg/mL, whereas the IL-6 kit had a sensitivity of 0.2 pg/mL. The intraassay coefficient of variation for TNF-α and IL-6 was less than 10%. The interassay coefficient of variation for TNF-α was 12.2% and for IL- 6 was 18.2%.
Statistical Analysis
For descriptive purposes, means and SDs were computed for all subjects in the study. Because the cytokines’ concentrations were not normally distributed, their values were transformed using the natural logarithm to obtain a normal distribution for the multiple-regression and ANOVA analyses. The main analyses were conducted in 2 steps. First, to determine the relationship between the cytokines and the different surrogates for adiposity, separate multiple-regression models were analyzed for each cytokine. Each evaluated model included one of the surrogates (BMI percentile, SSF, or WC), controlling for ethnicity (African American, white, and other), and sex. The BMI percentile model included BMI as a dichotomous variable due to its bimodal distribution (<75th and >95th percentiles groups). Second, ANOVAs were used to determine which surrogate better discriminated differences in the concentration of the cytokines between high and low percentiles of the different surrogates. From the initial 2 groups based on BMI percentile (normal and overweight), 2 other subgroups were a posteriori formed, one based on SSF percentiles and the other based on WC percentiles. The SSF groups were based on the 75th and the 95th percentiles from NHANES I. 26 Although grouping based on the NHANES I data may not be totally appropriate in the present day, it is currently the only available nationwide data on SSF by sex and age. The WC groups were developed using the age-, the sex-, and the race-specific tables of percentiles developed by Fernandez et al. 27 from NHANES III data. The WC percentiles grouping was based on the 75th and the 90th percentiles because abdominal adiposity is defined as a WC higher than 90th percentile. This subgrouping based on percentiles of SSF and WC resulted in a loss of some subjects from the initial 120 participants. Statistical significance was held at P < 0.05. Analyses were conducted using Statistical Package for Social Sciences for Windows (Version 9.0; SPSS, Inc).
Results
Subjects’ Characteristics
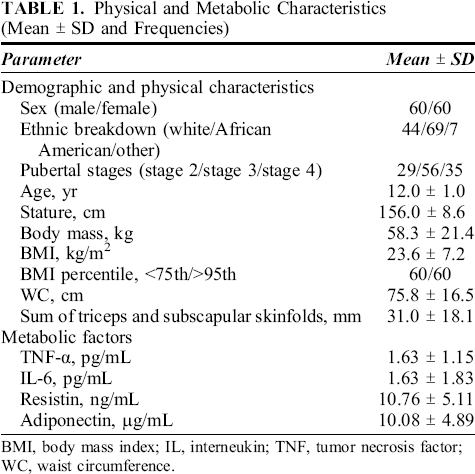
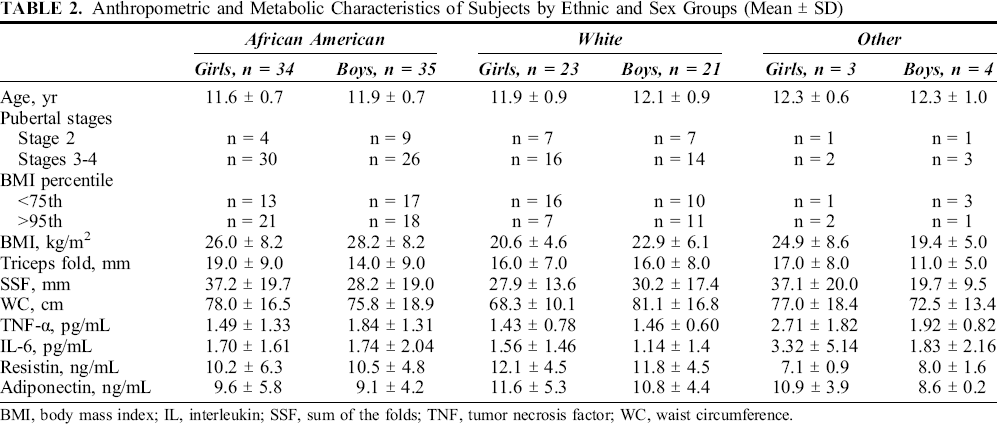
The subjects’ characteristics are presented in Table 1. The subjects were 11.9 ± 0.8 years. Racial distribution was 57% African American, 37% white, and 6% other races including Native American, Asian, and other. Subject characteristics presented by sex, and ethnicity categories are also provided in Table 2.
Physical and Metabolic Characteristics (Mean ± SD and Frequencies)
Anthropometric and Metabolic Characteristics of Subjects by Ethnic and Sex Groups (Mean ± SD)
Multiple Regression Analyses
Table 3 contains the results of the multiple-regression analyses. For each cytokine, 3 separate regression models were tested, one for each surrogate, BMI, SSF, and WC; all included sex and ethnicity as control variables. The standardized β-coefficients ± SE are presented for each surrogate marker of adiposity as well as the total R2 ± SE for the regression model. For TNF-α, the models containing BMI percentile and SSF were significant, but the model for WC was not significant. Sum of skinfolds and WC were both significantly associated with IL-6 (P < 0.05), but the regression models including those parameters were not significant. For resistin, both the SSF and the WC models were significant (P < 0.05). All the models for the adiposity surrogates were significant for adiponectin (P < 0.01).
Total Variance (R2) and β-Coefficients for Separate Multiple Regression Models for Each of the Four Cytokines and Surrogate Markers of Adiposity (BMI Percentile, SSF, and WC), Controlling for Sex and Ethnicity

Fasting cytokines based on BMI, SSF, and WC percentiles
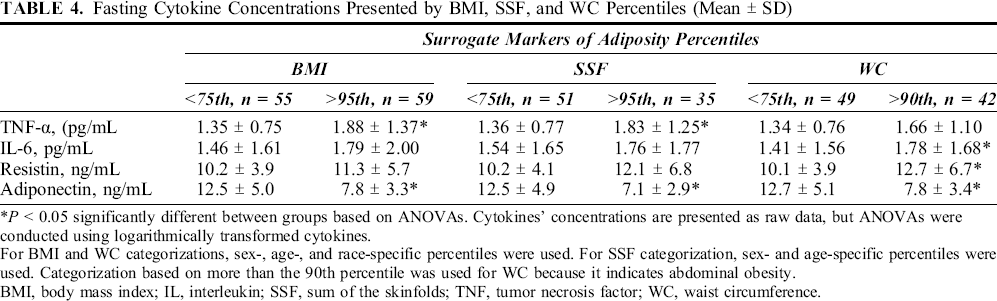
The cytokine concentrations for the 3 different grouping methods are presented in Table 4. TNF-α concentrations were higher (P = 0.014) and adiponectin concentrations were lower (P < 0.001) in youth with a BMI higher than the 95th percentile. Youth with SSF higher than the 95th percentile had higher TNF-α (P = 0.025) and lower adiponectin concentrations (P < 0.001) than youth with SSF lower than the 75th percentile. Finally, youth with WC higher than the 90th percentile had higher resistin (P = 0.029), higher IL-6 (P = 0.028), and lower adiponectin (P < 0.001) concentrations than those with WC lower than the 75th percentile.
Fasting Cytokine Concentrations Presented by BMI, SSF, and WC Percentiles (Mean ± SD)
Discussion
To our knowledge, ours is the first study in youth that compared cytokines concentrations based on WC and SSF percentiles as well as BMI percentile. Of these 3 surrogates, BMI percentile seemed to be least related to the cytokines. Although the regression analyses found that SSF was associated statistically with all 4 cytokines, when grouped by SSF percentiles, there were no differences in IL-6 or resistin. This could be perhaps due to SSF thresholds not being as sensitive as WC thresholds to indicate differences in these 2 cytokines.
The associations between TNF-α and resistin concentrations and SSF are novel findings in youth. Similar to other studies that used SSF to compute body fat percentage,28,29 we found an inverse association between adiponectin and SSF. Waist circumference was associated with increased IL-6 and decreased adiponectin. Although the degree of association between WC and IL-6 was low, this finding confirms previous results.11,17,30 In contrast to a study by Moon et al., 20 we did not find a significant relationship between TNF-α and WC. However, the youth in the present study were younger (mean age, 11.9 years) than the adolescents studied by Moon et al (mean age, 15.3 years). Perhaps this association develops with age and accrual of trunk adiposity and/or the potentiating interactions that could develop among cytokines. 31 In adults, resistin has been linked with trunk adiposity 32 ; we found that the overall model was significant but WC as a predictor was borderline significant (P = 0.075). Due to the dynamic nature of WC during the years of growth, an adjustment may be required when studying the association between WC and resistin or TNF-α in youth. In support of this contention, when both cytokines’ concentrations were compared by WC percentiles rather than absolute waist measurements, significant differences or trend were obtained between groups.
Overall, with the exception of adiponectin, the associations obtained either between SSF or WC and cytokines were low. Had we used a more sensitive measurement of subcutaneous adiposity or abdominal adiposity, the found associations might have been stronger. However, adipose tissue is one source of all these cytokines,3,31,33 but TNF-α, IL-6, and resistin are also produced by the muscle and immune system cells,3,31,33 and thus circulating concentrations of these cytokines may not be strongly related to adiposity. Conversely, adiponectin is produced solely by the adipocytes, and the association with adiposity surrogates should be, and was, stronger.17,18 Nevertheless, when evaluating all these weak associations together, one can relate increased adiposity to increased overall inflammation, a metabolic abnormality that can be in turn related to insulin resistance and vascular disease.
Percentiles of BMI, WC, and SSF
To account for the dynamic nature of growth in our subjects, we examined percentiles for BMI, WC and SSF. Our BMI results confirm the results of previous studies.11,15,20,28,34 Overweight youth (BMI >95th percentile) are characterized by having higher concentrations of TNF-α, lower concentrations of adiponectin, but similar IL-6 and resistin concentrations to normal weight adolescents.11,15,20 Previous research suggested that IL-6 concentrations seem to be significantly elevated only when adolescents had a BMI higher than 97th percentile. 34
Youth with WC higher than the 90th percentile had higher resistin and IL-6 and lower adiponectin concentrations than those with WC lower than the 75th percentile. Although no significant differences were observed in TNF-α concentrations using Fernandez et al cutpoints (P = 0.079), if TNF-α concentrations were compared based on WC groups using Li et al. 35 WC cutpoints, those youth with abdominal adiposity (WC >90th percentile) showed a trend toward higher TNF-α concentrations than their counterparts (P = 0.056). These 2 separate analyses would suggest higher TNF-α concentrations if adolescents have a WC higher than the 90th percentile. Given that there are no other studies that evaluated differences in these cytokines between WC percentiles, we cannot contrast our results to other studies including a pediatric population. Our findings are, however, in agreement with the adults studies relating trunk or central adiposity to resistin, IL-6, TNF-α, or adiponectin.10,11,30,32 On the basis of our results, we suggest that WC percentiles could be used as a screening tool potentially linked with increased inflammation in youth. This finding has clinical implications, as WC measurements can be almost as easily obtained as BMI in the clinician's office. Moreover, WC results are highly reproducible 25 and do not rely as heavily on technician experience as skinfold measurements. 26
The sample of youth studied had unique and relevant characteristics: an even number of girls and boys, from a diverse ethnic background, and at pubertal stages associated with higher insulin resistance. Although the differences in these cytokines’ concentrations between percentiles of BMI, WC, and SSF were low (∼20%), they may have an important physiological role in the tissues either in relationship to insulin resistance or atherosclerosis.4–8,17,28,31 Moreover, these differences in the concentrations of these cytokines are likely clinically meaningful. These elevated or decreased cytokines concentrations may herald “the tip of the iceberg,” the early stages of an interactive process in which the inflammatory mediators associated with the obese state are linked to insulin resistance and other comorbidities over many years. It is therefore important that the reader keeps in mind that adiposity and inflammation are complicated processes that most likely initiate a cascade of additional factors that result in overt disease.
Adiposity measurements obtained with a computed tomography scan or dual x-ray absorptiometry provide more exact estimations of subcutaneous, visceral, or overall adiposity and possibly result in more precise findings, perhaps leading to stronger associations. However, these 2 methods are expensive due to the specialized equipment involved, expose the subjects to ionizing radiation, and are less applicable in a clinical setting. In contrast, the surrogates of adiposity used in this study had been previously validated23–27 and were obtained with trained and certified research assistants supporting the clinical implication of these results. Waist circumference measurements are almost as easily obtained as a measurement of body mass or height and seem to be more sensitive to detecting increased inflammation. Therefore, our study further contributes to the notion that pediatric clinicians should not only screen for obesity using BMI, but they should screen for abdominal obesity (WC >90th percentile) due to the association between abdominal adiposity and insulin resistance, cardiovascular disease, metabolic syndrome, and inflammation.34,36,37
A limitation of this study was the lack of control in day to day variation in the concentration of these cytokines, or other conditions such as illness that could confound measurements of cytokines in our sample. However, the cytokine values reported were within ranges of previously published studies,9,15,17,19–20 except from the IL-6 values, which were in the low end of the published ranges.19,29 Another factor influencing the results could be pubertal development. Control for differences in these cytokines due to sexual maturation was attempted by selecting a sample of youth who were between stages 2 and 4, but differences could be expected even among these stages. The similar number of normal weight and overweight subjects, as described by BMI percentile, provided the opportunity to make inferences about the association between these cytokines with weight status, but this may have also limited the results with respect to SSF and WC. Finally, there could be other confounding factors in the studied relationships that may have not been controlled.
Conclusions
Our results suggest that in youth, a proinflammatory profile was more associated with SSF and WC than with a BMI percentile indicating obesity. Regression analyses suggest that SSF seems to be the adiposity surrogate associated with most of these cytokines, although the degree of association was low with the exception of adiponectin. In contrast, ANOVA analyses suggest that WC percentile was a better surrogate to distinguish differences in cytokines between youth who have central/trunk obesity and those who do not. The similarity in the amount of variance in the regression models for adiponectin (∼30%) explained by the 3 surrogates provides evidence that no one surrogate of adiposity may be more important than the others to predict circulating adiponectin, although this may not be true for other cytokines. Therefore, to gain a better understanding of the relationship between childhood obesity and inflammatory state leading to insulin resistance and other comorbidities, pediatric researchers and health care providers should routinely estimate central adiposity by measuring WC.