
Abstract
Recently, we reported hippocampal and temporal lobe abnormalities in 5 toddlers with sudden unexplained death in childhood (SUDC). The association of these anomalies with a high incidence (40%) of individual/family histories of simple febrile seizures in the cases raised concern that febrile seizures can be associated with death. In a series of 64 toddlers with sudden death, we tested the hypothesis that an SUDC subset is characterized by hippocampal and temporal lobe maldevelopment and an individual and/or family history of simple familial seizures. Cases of sudden and unexplained death in children aged 1.0 to 5.9 years (median 1.7 years) were divided into groups based upon a history of febrile or nonfebrile seizures, familial febrile seizures, and autopsy classification of cause of death. Forty-nine of the 64 cases (77%) were classified as SUDC, of which 40% had an individual/family history of febrile seizures. Of the 26 SUDC cases with available hippocampal sections, 62% (16/26) had hippocampal and temporal lobe anomalies, including 82% (9/11) of cases with an individual/family history of febrile seizures. Cases with these anomalies were all found dead during a sleep period, typically in the prone (87%) position. We conclude that a potential new entity may account for the majority of SUDC in toddlers, defined by sleep-related death in the prone position, individual/family history of febrile seizures, and hippocampal and temporal lobe anomalies. The mechanism of death appears analogous to sudden death in (temporal lobe) epilepsy, with a putative unwitnessed seizure during sleep leading to airway occlusion and death. This study mandates further research into the potential link between simple febrile seizures and death.
Keywords
INTRODUCTION
Sudden unexplained death in childhood (SUDC) is the sudden death of a child older than 1 year of age that remains unexplained after a review of the clinical history and circumstances of death and performance of a complete autopsy with appropriate ancillary testing [1]. SUDC occurs most commonly in toddlers between 1 and 4 years, with an annual incidence of 1.3/100 000 [2]. Recently, we reported developmental abnormalities in the hippocampus and temporal lobe in 5 toddlers with sleep-related SUDC [3]. The hippocampus, situated in the medial temporal lobe, is critical for memory of facts and events, spatial navigation, learning, and cardiorespiratory modulation [4–8]. Because the findings of malformation in the hippocampus and temporal lobe in the 5 SUDC cases were essentially identical to those associated with some cases of temporal lobe epilepsy [9–15] and sudden unexpected death in epilepsy (SUDEP) [16,17], we proposed that these anomalies represented an epileptogenetic focus that, when triggered by fever, trivial infection, or minor head trauma at a susceptible age, resulted in an unwitnessed seizure, cardiopulmonary arrest, and sudden death [3].
In the 5 original SUDC cases with hippocampal anomalies [3], we were impressed with the high incidence of febrile seizures (40%) compared to 2% to 5% in the general pediatric population [18–20]. Moreover, 40% of the children had a family history of febrile seizures compared to the reported general incidence of 24% of family history of febrile seizures in children with febrile seizures [18]. Febrile seizures are convulsions associated with fever in the absence of central nervous system (CNS) infection in a child between 6 months and 6 years of age [18]. Complex febrile seizures are distinguished from simple febrile seizures by prolonged duration (>15 minutes), focality, and/or repetition within 24 hours [18]. Complex febrile seizures are also associated with subsequent development of temporal lobe epilepsy in 2% to 7% of cases [20], whereas simple febrile seizures are considered a benign disorder without morbidity or mortality [18–29]. Our initial report [3] raised concern that an individual and/or family history of simple febrile seizures represents a marker of developmental temporal lobe pathology that increases seizure susceptibility during a febrile illness and is associated with unwitnessed sudden death. Accordingly, in the following expanded retrospective series of 64 toddlers with sudden death, we tested the hypothesis that a subset of SUDC cases is characterized by an individual and/or family history of febrile seizures and hippocampal maldevelopment.
METHODS
Clinical database
Cases and controls were accrued retrospectively through the San Diego SIDS/SUDC Research Project over its first 5-year period (2002 to 2007) [1]. This project has been previously described in detail [1]. Briefly, national and international cases were referred by medical examiners, primary care physicians, or the families themselves upon learning of the project through the SUDC website (http://www.sudc.org). Obstetric, pediatric, hospital, scene investigation, autopsy records, and microscopic sections were reviewed [1]. In addition, the parents completed a detailed questionnaire concerning the child's medical, neurodevelopmental, environmental, and family histories. The research was approved by the Institutional Review Board of Rady Children's Hospital, San Diego, CA. The inclusion criteria for this study were: (1) parental consent, (2) autopsy not restricted to a single organ, and (3) death between 1 and 6 years of age. The pediatric pathologist (H.F.K) classified all deaths as SUDC or non-SUDC (controls). The pediatric neuropathologists (H.C.K., M.G.) reviewed the CNS reports and microscopic slides of all cases, and the hippocampal sections were reviewed in consultation with a third pediatric neuropathologist (D.L.A.).
Group classification
The 64 patients were initially divided into 3 broad groups based on autopsy classification: SUDC, nonfebrile seizure controls, and non-SUDC diagnosis. Based on prior findings [3], the SUDC cases were then further divided into 3 groups based upon a history or family history of febrile seizures, thus resulting in a total of 5 groups: group 1—SUDC and an individual history of febrile seizures (with or without a family history of febrile seizures) (n = 12); group 2—SUDC and family history of febrile seizures (but no individual febrile seizures) (n = 7); group 3—SUDC without an individual or family history of febrile seizures (n = 30); group 4—non-SUDC with a history of nonfebrile seizures (n = 4); and group 5—non-SUDC with established causes of death (n = 11). In group 2, we reasoned that a family history of febrile seizures indicates a genetic susceptibility for the presumed entity and that the toddler may have died before having a witnessed febrile seizure.
Characterization of hippocampal anomalies
All brains were examined macroscopically at autopsy, but the number and regions of microscopic sectioning varied across medical examiner offices, such that the hippocampus and temporal lobe were not sectioned microscopically in all cases, given that this study is retrospective. Thirty-four of the 64 (53%) cases in this series had at least one hippocampal section available for review; the histological preparation of the hippocampal sections has been described in detail [3]. All hippocampal slides were reviewed for the entire spectrum of pathology in a blinded fashion, without clinical or general autopsy information [9]. They were scored for the presence or absence of microdysgenetic features (microscopic malformations), e.g., granule cell duplication, excessive dentate gyrus folding, cortical laminar disorganization, “fetal-like” arrangement of cortical neurons, increased neurons in Layer I, neuronal clustering in neocortical Layers II to VI, granular heterotopia, subventricular neuroblasts, hamartia, giant neurons, persistent subpial granule cell layer, and leptomeningeal heterotopias [3,9–17]. They were also scored for the presence or absence of other temporal lobe anomalies, e.g., hippocampal malrotation, malformed gyri, folded subiculum, and white matter heterotopia or excessive single neurons. We also recorded the presence or absence of Ammon's horn sclerosis, i.e., hippocampal atrophy with neuronal loss and gliosis in CA1 and end-folium; pathology may also be found at other mesial temporal lobe structures and/or temporal lobe white matter [12]. Definitions and illustrations of hippocampal/temporal lobe anomalies and Ammon's horn sclerosis are available in published reports [3,9–17]. The previous report by us of the series of 5 toddlers with macroscopic and microscopic findings in the hippocampus and temporal lobe provides an “atlas” of the temporal lobe pathology in all of the reported cases here for reference [3].
Controls for hippocampal histopathology
Analysis of microdysgenesis in the hippocampus/temporal lobe requires control groups for comparison, as it is occasionally reported in otherwise normal brains at autopsy [9]. For controls, we used non-SUDC cases in which the cause of death was established, i.e., nonfebrile seizures (group 4) and miscellaneous established causes of death without seizures (group 5) that were part of the national SUDC registry in San Diego; all control cases that came to this registry during the time-frame of the study and met the above inclusion criteria were used. To increase the control sample size, we also used control cases from an archival database of human hippocampal/temporal lobe sections developed by us from the autopsy services of our pediatric hospitals [3]. The age of the archival patients ranged from 1 to 5 years, with a median of 2.5 years [3]. Group 6 (n = 3) consists of archival cases with a history of nonfebrile seizures and group 7 (n = 11) consists of archival cases with an established cause of death and no history of seizures.
Statistical analysis
Groups were compared using Fisher exact tests for categorical outcomes and analysis of variance for continuous outcomes. In all analyses, P < 0.05 was considered significant; marginally significant trends, however, were also noted in this small sample. No adjustment for multiple testing was made due to small sample size and the exploratory nature of several analyses. Tests of the hypothesis that a subset of SUDC cases is characterized by an individual and/or family history of febrile seizures and hippocampal maldevelopment should be considered hypothesis confirming; all other results, e.g., on sleep characteristics and illness, should be considered hypothesis-generating.
RESULTS
Classification of cases
Sixty-four cases of sudden death in toddlers in the San Diego SIDS/SUDC Research Project met our entry criteria. This series of 64 cases includes the 5 original cases reported with macroscopic asymmetry of the hippocampus [3], as well as 2 non-SUDC cases that were published separately [21]. Of the total 64 cases, 49 (77%) were classified as SUDC and 15 (23%) with known causes of death established at autopsy (Table 1). The latter group consisted of: (1) miscellaneous disorders (11/64 [17%] of cases) and (2) nonfebrile seizure disorders (4/64 [6%] of cases). The miscellaneous causes of death were: meningitis and neurogenic pulmonary edema (n = 3) [21]; myocarditis (n = 2); aortic stenosis (n = 1); long QT syndrome with KCNQ1 mutation (n = 1); histiocytoid cardiomyopathy (n = 1); foreign body aspiration (n = 1); probable fatty acid deficiency (n = 1); and central motor system disorder of unknown type (n = 1). In 3 cases of nonfebrile seizure disorders (group 4), the seizure was observed at the time of death and led to a fatal cardiopulmonary arrest; in the 4th case, the toddler had repetitive atypical seizures, last witnessed within 2 weeks of death, and SUDEP was suspected. There were no significant differences at death in age, sex, or race of the SUDC cases (groups 1 to 3) compared to the non-SUDC groups (groups 4 and 5) (Table 1). There were no significant differences in the incidence of cerebral edema and intrathoracic petechiae among the 5 groups.
Demographics of SUDC vs non-SUDC controls
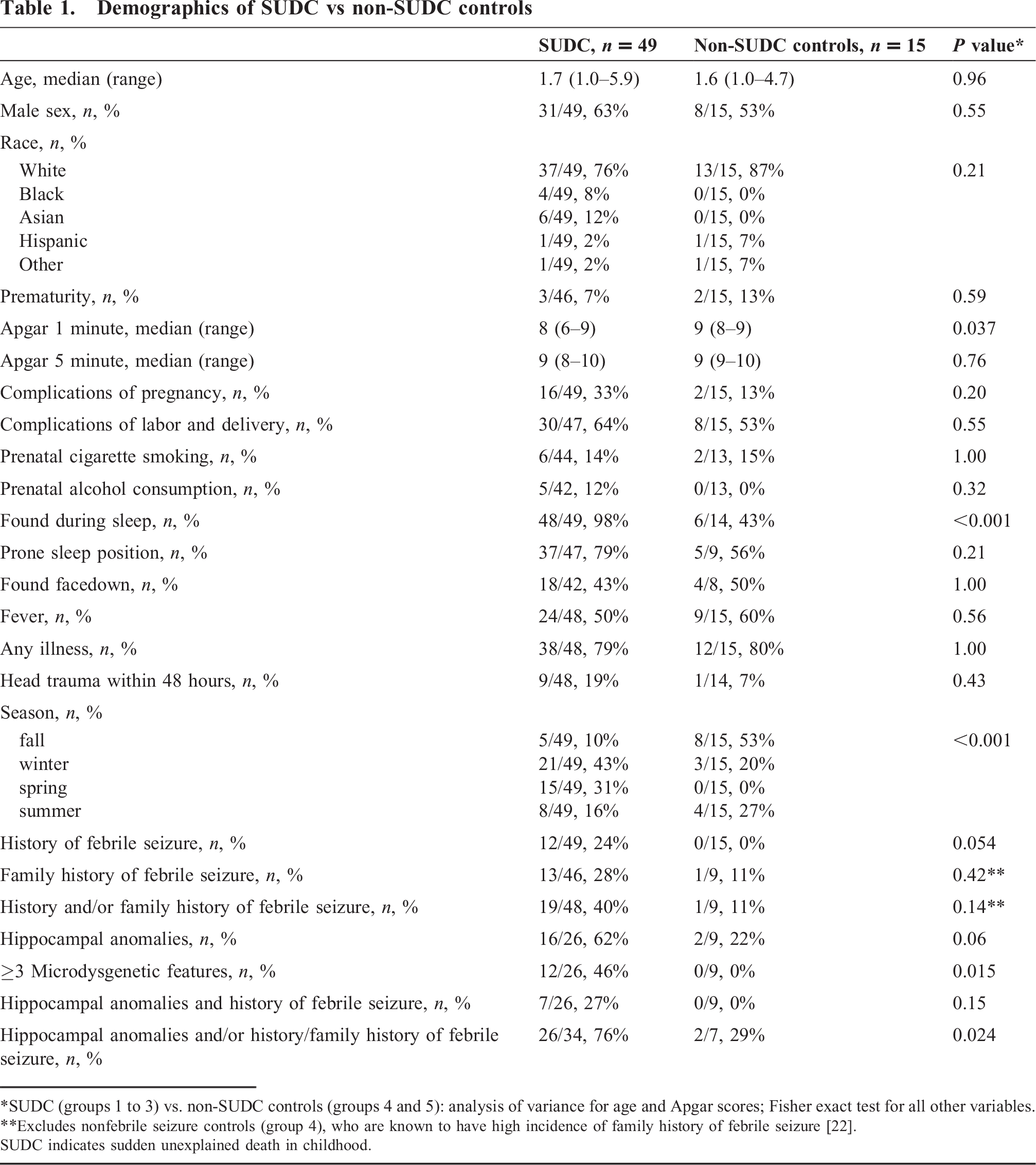
SUDC (groups 1 to 3) vs. non-SUDC controls (groups 4 and 5): analysis of variance for age and Apgar scores; Fisher exact test for all other variables.
Excludes nonfebrile seizure controls (group 4), who are known to have high incidence of family history of febrile seizure [22].
SUDC indicates sudden unexplained death in childhood.
SUDC and febrile seizures
More SUDC compared to non-SUDC cases had a history of febrile seizures (24% vs. 0%) and were found dead after a sleep period (98% vs. 43%) (Table 1). Table 2 breaks the SUDC cases into the 3 groups based on history of febrile seizure to further characterize these subsets of SUDC. Groups 1 and 2 were more likely to be found dead in the prone sleep position (100% vs. 66%) and group 1 was less likely to have a fever (P = 0.032). The complications of pregnancy were typically mild, including gestational diabetes, vaginal bleeding at any trimester, and premature onset of labor treated with tocolytics; no single complication characterized all cases.
Analysis of demographic and hippocampal variables among SUDC cases with an individual and/or family history of febrile seizures, and SUDC cases with no individual or family history of febrile seizures
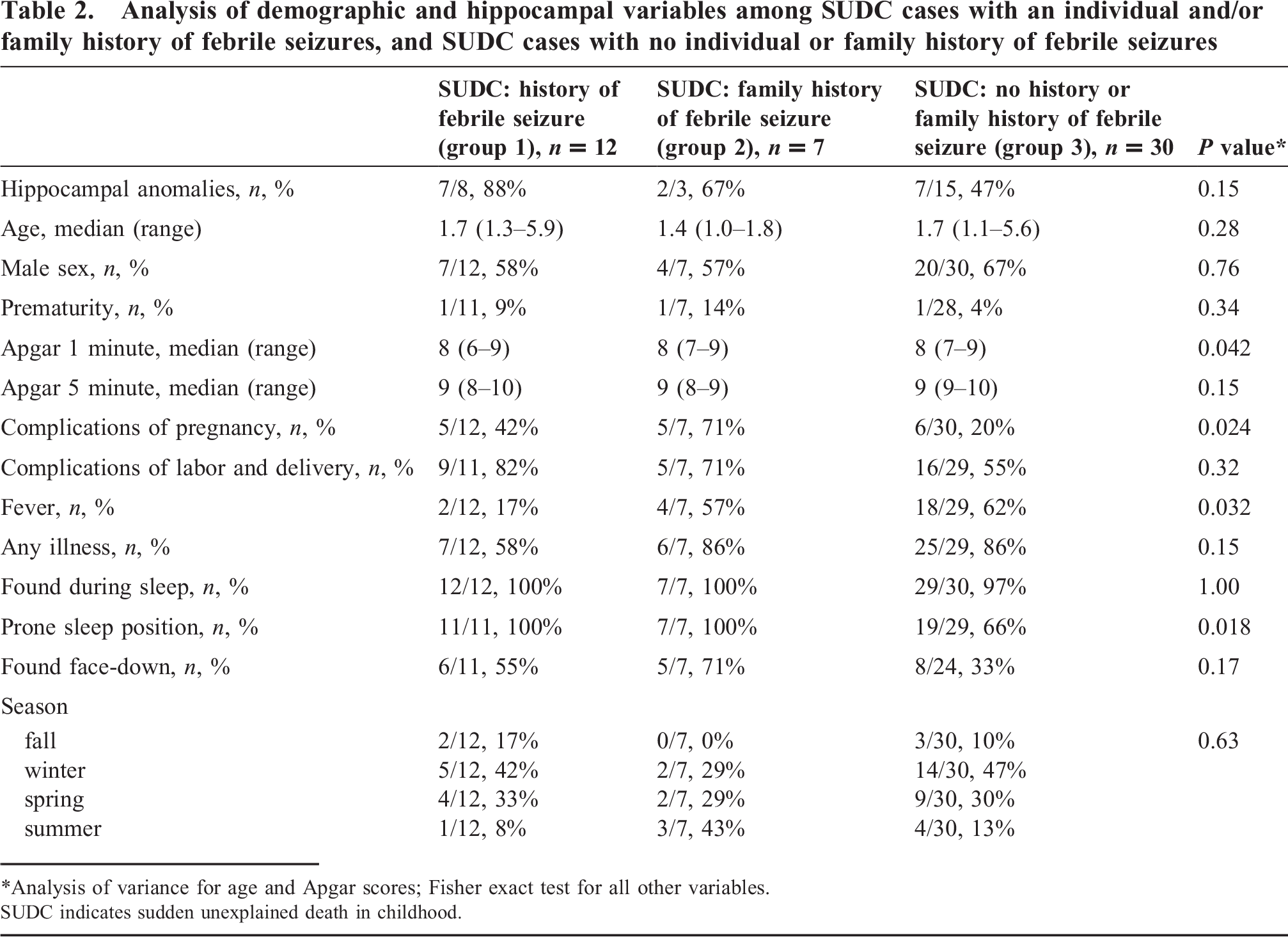
Analysis of variance for age and Apgar scores; Fisher exact test for all other variables. SUDC indicates sudden unexplained death in childhood.
Of the 12 cases with a history of febrile seizures (group 1), the median age of onset of febrile seizures was 15 months (range, 9 to 24 months); the median number of febrile seizures was 1.5 (range, 1 to 6). The median period between the last seizure and death was 4 months (range, 3 weeks to 2 years). In all 12 cases, the febrile seizures were simple, generalized, and lasted less than 15 minutes. All toddlers were evaluated at the time of the first febrile seizure in acute care settings, and a simplex febrile seizure was diagnosed. One toddler was referred for an electroencephalogram, which was interpreted as normal (including upon retrospective review). No neuroimaging studies were performed, and none of the toddlers was treated with antiseizure medication. One toddler in group 1 had attention deficit disorder and mild motor delay, and a second toddler also had motor delay; the other toddlers in this group were neurologically normal.
SUDC and hippocampal pathology
SUDC cases had more hippocampal anomalies compared to non-SUDC cases (62% vs. 22%) (Table 1), especially SUDC cases with a history of individual febrile seizures (group 1) or a family history of febrile seizures (group 2) (Table 2). Seven of the 15 (47%) SUDC cases without an individual or family history of febrile seizure (group 3) and with available hippocampal sections demonstrated hippocampal maldevelopment, in addition to 88% (7/8) in group 1 and 67% (2/3) in group 2 (Table 2). Cases with macroscopic asymmetry of the hippocampus at autopsy were present in all of the SUDC groups, but in none of the non-SUDC cases (Table 3). The SUDC groups had more hippocampal/temporal lobe abnormalities (primarily group 1, P < 0.001) and presence of ≥3 individual hippocampal anomalies (primarily groups 1 and 2, P < 0.001) compared to the control groups (Table 3). The microdysgenetic features that were significantly common to the SUDC groups were dentate gyral anomalies (primarily groups 1 and 2, P = 0.010) and granular nodular heterotopia (primarily group 2, P = 0.040) (Table 3).
Analysis of hippocampal features among SUDC cases with an individual and/or family history of febrile seizures, SUDC cases with no individual or family history of febrile seizures, and non-SUDC controls and archives
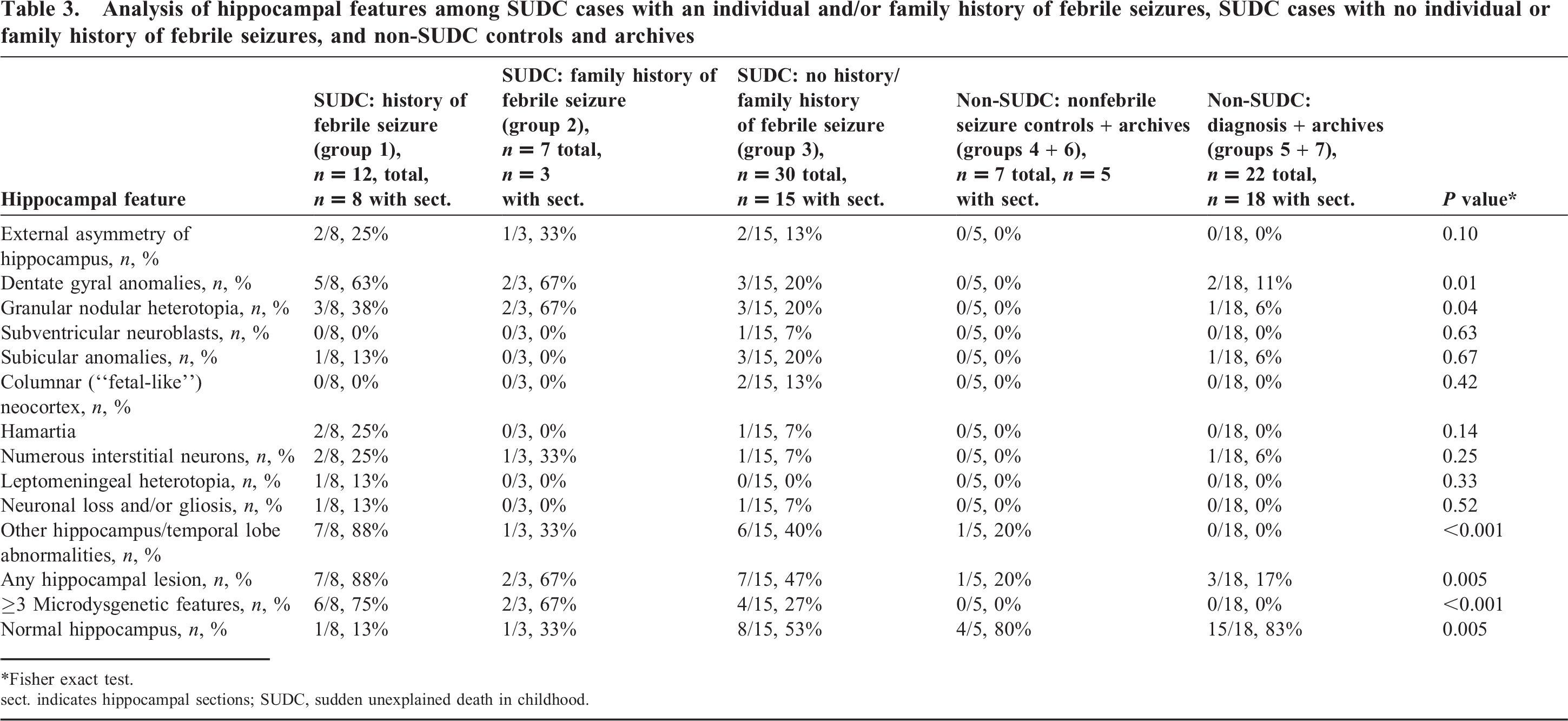
Fisher exact test.
sect. indicates hippocampal sections; SUDC, sudden unexplained death in childhood.
Table 4 divides the SUDC cases by presence of hippocampal anomalies. This analysis is exploratory and hypothesis generating. Compared to SUDC cases with no hippocampal pathology, SUDC cases with hippocampal pathology were more likely to be found in the prone position (87% vs. 50%, P = 0.080) (Table 4). In 5 of the 16 SUDC cases with hippocampal anomalies (31%), we identified minor developmental abnormalities elsewhere in the brain, consisting of dysplasia of the inferior olive (n = 3), fetal-like cortex (outside the temporal lobe) (n = 2), and heterotopia (n = 1) and excessive interstitial neurons (n = 1) in the cerebral white matter (n = 1), and heterotopia in the periaqueductal gray matter (n = 1). In contrast, 2 of the 10 (20%) SUDC cases without hippocampal anomalies demonstrated minor anomalies elsewhere in the brain, i.e., heterotopia (n = 1) and excessive interstitial neurons (n = 2) in the cerebral white matter (n = 2), and no olivary anomalies. Two of the 16 SUDC cases (13%) with hippocampal anomalies also demonstrated focal scars in the cerebral or cerebellar cortex, consistent with remote hypoxic-ischemic injury, perhaps secondary to previous febrile seizures; none of the SUDC cases without hippocampal abnormalities demonstrated such findings.
Division of SUDC cases into those with hippocampal anomalies and those without hippocampal anomalies (of those with available hippocampal sections, n = 26)
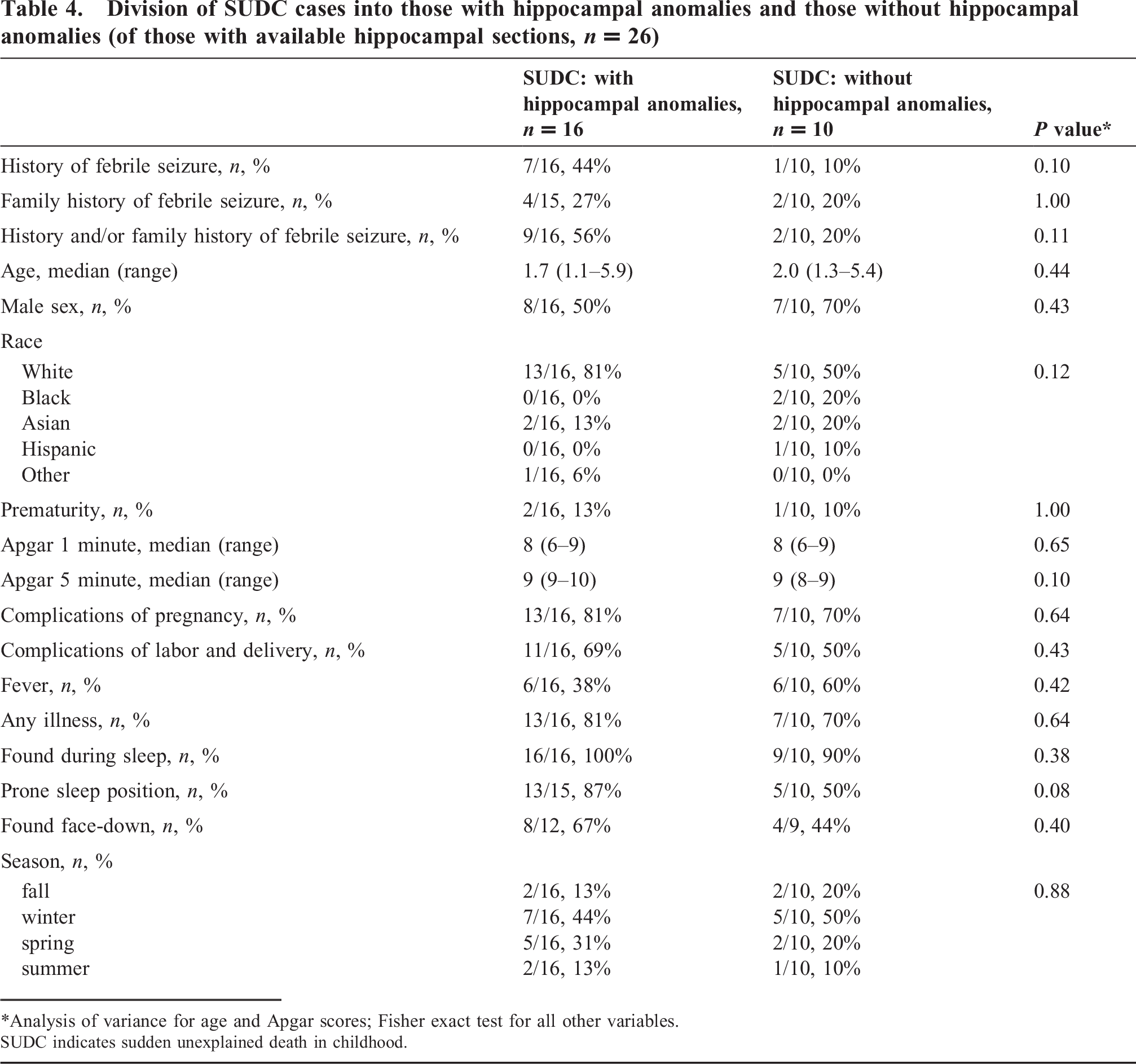
Analysis of variance for age and Apgar scores; Fisher exact test for all other variables. SUDC indicates sudden unexplained death in childhood.
DISCUSSION
In this series of 64 toddlers with sudden and unexpected death, SUDC is the leading category of death, accounting for 77% of cases. We have confirmed the hypothesis that a subset of SUDC cases is characterized by an individual and/or family history of febrile seizures and hippocampal maldevelopment. We have also explored other sleep-related characteristics of SUDC. Embedded within SUDC, we discovered a potential new entity that accounts for approximately 62% (16/26) of SUDC in toddlers, defined by unwitnessed, sleep-related, sudden death and hippocampal/temporal lobe maldevelopment and characterized by an individual and/or family history of febrile seizures and prone sleep position, often face-down, at discovery. We suggest the following name for this potential entity: “Sudden Unexplained Death in Childhood Associated with Hippocampal Anomalies and Febrile Seizures in Toddlers” or SUDC-HAFST. Hippocampal/temporal lobe maldevelopment is the defining feature of the putative new entity, and individual and/or family histories of febrile seizures are important risk factors for sudden death in association with this underlying pathology. Indeed, this study heightens concern that individual and/or family histories of simple febrile seizures represent a marker of an extremely rare but fatal outcome in affected toddlers, in contrast to the widespread consensus that such seizures are benign and without mortality [18–20]. The question arises: Why has the potential association between simple febrile seizures and death not been previously recognized? One possibility is the prolonged temporal relationship between witnessed febrile seizures and death, given that the median period between a febrile seizure and death in the present study was 4 months and as long as 2 years. An additional possibility is the extreme rarity of this potential new entity, as it represents only part of the minimal overall annual incidence of SUDC in toddlers (1.3/100 000) [2]. Our ability to detect SUDC-HAFST likely reflects the nature of a centralized registry in which multiple SUDC cases were received for review over a half-decade from the United States, Canada, and Europe.
The finding of temporal lobe anomalies in SUDC, in conjunction with analogy to temporal lobe epilepsy and SUDEP, suggests the possibility that affected toddlers experience an unwitnessed, sleep-related seizure that originates in the anomalous epileptogenetic focus in the hippocampus, resulting in upper airway occlusion/cardiac arrhythmia/hypotension, and fatal cardiopulmonary arrest. The hippocampus is a critical component of limbic circuits that modulate heart rate, blood pressure, and breathing according to behavioral state [3,6–8]. It projects directly to brainstem and hypothalamic regions critical for cardiovascular and respiratory control, including the ventrolateral medulla that contains neurons essential for respiratory drive [3,6–8]. In SUDEP (in which epilepsy is defined as a history of witnessed nonfebrile seizures), hippocampal microdysgenesis and AHS have been reported, including in children [15–17]. It is postulated that SUDEP associated with temporal lobe epilepsy is due to seizure-related, hippocampal hyperexcitability and downstream effects upon cardiorespiratory pathways [6–8,15–17,23–25]. Of note, ictal arrhythmias are postulated to cause SUDEP in some young adults [26]. In addition, infants and young children with partial epileptic seizures and temporal lobe pathology experience ictal autonomic symptoms, including apnea, hyperventilation, and bradycardia [27]. We propose here analogous mechanisms in SUDC-HAFST.
The major clues to deciphering the pathogenesis of sudden death in SUDC-HAFST are the association of death with a sleep period and prone sleep position, as 100% of our cases were found dead after a sleep period, and almost all in the prone position, often face-down. Major risk factors for SUDEP are also nocturnal sleep and prone sleep position [28], including in children [29]. In general, seizures are well recognized to occur frequently during the night and/or sleep due, at least in part, to sleep-induced changes in neuronal excitability and synchrony, leading to reduced seizure threshold [30]. The prone position in SUDEP may cause obstruction of the nose and mouth due to pressure of the bed clothing [29]. We speculate that a terminal and fatal seizure leads to death in SUDC-HAFST due to seizure-induced upper airway occlusion, augmented by airway compression in the prone (face-down) position. Experimental rat data in reduced preparations indicate the generation of obstructive apnea by (fictive) seizures, thereby supporting a causal role for obstructive apnea in seizure-induced sudden death [31]. The relationship of SUDC to winter is similar to that in sudden infant death syndrome (SIDS) and may reflect increased respiratory tract infections at this time, a potential triggering factor.
Microdysgenesis and temporal lobe anomalies in SUDC-HAFST reflect aberrant neuronal proliferation, migration, and differentiation during the formation and development of the hippocampus in the fetal period [9,10,12,13]. Of note, microdysgenesis is not specific for epilepsy, as it has been reported in otherwise normal brains and brains of patients with other neurological entities [3,9,32,33]. In addition, subtle changes, e.g., dispersion of dentate neurons, can reflect seizure effects on postnatal neuronal development [9]. Nevertheless, microdysgenesis is more common in brains associated with epilepsy [9–16], as well as in the brains of the SUDC cases with an individual and/or family history of febrile seizures in this series. The increased incidence of complicated pregnancies in groups 1 and 2 underscores the possibility that adverse environmental factors during gestation contribute to the maldevelopment of the temporal lobe. The association of minor anomalies elsewhere in the brain in 25% of the SUDC cases with hippocampal anomalies supports the developmental origin of the hippocampal pathology. Neuroimaging reports of hippocampal asymmetry in patients with a history of febrile seizures and in family members without febrile seizures support the idea of underlying hippocampal maldevelopment in genetically susceptible individuals [34–37]. Febrile seizures with or without hippocampal anomalies and/or temporal lobe epilepsy have been associated with various gene mutations [38]. None of these known gene mutations, however, is associated with sudden death in early life, and thus, it is likely that SUDC-HAFST represents a new genetic disorder. Genetic analysis of the affected families in this study is in progress.
An additional major finding in this study is that 31% of SUDC cases without individual and/or family histories of febrile seizures and/or hippocampal anomalies represent a group that necessitates further study in its own right. The question arises whether these toddler cases share the same etiology and pathogenesis as infants dying with the SIDS but who die beyond the 1-year “cut-off” of its operational definition [39]. Indeed, SIDS is defined as the sudden death of an infant less than 12 months of age that remains unexplained after a complete autopsy and death scene investigation [39]. Although prone sleep position is associated with SIDS [39], febrile seizures and hippocampal anomalies are not [40,41]. Furthermore, this group exhibited high rates of fever and illness, comparable to the non-SUDC controls, an unhealthy population; minor illness is also a risk factor for SIDS. Future analysis of this SUDC group is needed relative to SIDS. The demonstration of overlapping neuropathologic abnormalities in SUDC and SIDS cases, e.g., serotonergic brainstem abnormalities [42], would help clarify the relationship of these groups to each other.
In summary, this study suggests that simple febrile seizures may not be totally benign, but rather can be associated with a putative new entity, so-called SUDC-HAFST. This entity is characterized by sleep-related, unwitnessed, sudden death in a toddler in the prone position, individual/family history of febrile seizures, and hippocampal anomalies. We emphasize that this study reports only retrospective findings in a clinicopathologic series; it needs confirmation in a larger, independent dataset with systematic and standardized sectioning of the temporal lobe in a prospective study, if possible. Thus, our study is hypothesis generating and its goal is to make the medical community aware of the possibility that febrile seizures are not always benign. In this regard, a recent large study found a 5-fold higher risk of sudden unexpected death during the 2 years after a first febrile seizure (11 deaths per 100 000 children), although the absolute risk was considered to be very low [43]. While the risk for death after simple febrile seizures was not increased, there was excess mortality during 2 years after complex seizures [43], partly explained by pre-existing neurologic abnormalities and subsequent epilepsy. Although our cases presented as simple febrile seizures, they are “complex” in the sense that many of them have underlying hippocampal and temporal lobe pathology that is similar to that described in temporal lobe epilepsy. Further research is needed to establish the incidence, cause(s), and prevention of the putative new entity of SUDC-HAFST.
Footnotes
ACKNOWLEDGMENTS
We appreciate the dedicated participation of the SUDC parents in this study. We are also grateful for the help of the medical examiners in the autopsy review of the SUDC cases. We thank Drs Joseph J. Volpe and Holcombe E. Grier for invaluable comments in the course of the study and manuscript preparation, and we thank Mr Richard A. Belliveau for help with the preparation of the manuscript.