
Abstract
Our objective was to study histological variations and abnormalities in unclassified sudden infant death (USID), including sudden infant death syndrome (SIDS), in The Netherlands. Two hundred Dutch USID cases between 1984 and 2005 were identified. The histology slides and autopsy reports of 187 cases were available for systematic review, including brain autopsy in 135 cases. An explanation for the cause of death in 19 patients (10.2%) was found. Twelve patients had bronchopneumonia, 3 showed extensive aspiration, 2 had signs of a metabolic disorder, 1 had sepsis, and 1 had meningitis. Frequent nonspecific findings were congestion (66%), edema (47%), small hemorrhages (18%), and lymphoid aggregates (51%) in the lungs; congestion of the liver (23%); and asphyctic bleeding in the kidney (44%), adrenal gland (23%), and thymus (17%). Statistical associations were found for infection with starry sky macrophages in the thymus (P = 0.004), with calcification (P = 0.023), or with debris in the Hassal's corpuscles (P = 0.034). In this study, in 10.2% of cases the histological findings were incompatible with SIDS or USID. Furthermore, several frequent nonspecific histological findings in the thymus that point toward an infection were found.
Keywords
INTRODUCTION
Sudden and unexpected death in infancy (SUDI) includes every infant that dies suddenly and unexpectedly, including cases in which no investigations are done. If investigations do not lead to a diagnosis, the case is considered to represent unclassified sudden infant death (USID). Finally, in case of the sudden and unexpected death of an infant below 1 year in age, with onset of the fatal episode apparently occurring during sleep, with the cause of death remaining unexplained after thorough investigation (including performance of a complete autopsy and review of the circumstances of death and the clinical history), the term sudden infant death syndrome (SIDS) is used [1]. The Netherlands has one of the lowest rates of SIDS incidence worldwide [2] (0.08 per 1000 living births in 2011) [3]. However, a wider age range for SIDS is accepted, from birth to 3 years. Furthermore, autopsy is only performed upon parental consent, unless there is suspicion of a nonnatural cause of death, which results in an autopsy rate of about 60% of cases reported as SIDS in The Netherlands (Wierenga, personal communication). Thus, several cases classified in The Netherlands as SIDS are in fact SUDI and USID according to the internationally accepted definition [1]. Therefore, the incidence of SIDS in The Netherlands might be even lower. A solid parental education system and ongoing collection of environmental data related to new cases by a working group on SIDS of the Dutch Paediatric Society (Landelijke Werkgroep Wiegendood, LWW) are at the root of this success. Still, there continue to be SUDI cases in The Netherlands; these cases have a significant impact on involved health care workers and parents.
Unclassified sudden infant death and particularly SIDS are diagnoses of exclusion. Hence, most histology articles on USID and SIDS give guidelines on how to exclude other causes of death [4,5]. There are common histological observations in SIDS. Petechial hemorrhages occur in 66–95% of SIDS casees, pulmonary congestion in 89% of cases, and pulmonary edema in 63% of cases [2,4,6,7]. In a large (n = 536) 10-year SUDI cohort [8], 63% of cases remained unexplained and were diagnosed as SIDS (n = 337). In that study [8], 70% of SIDS cases showed nonspecific abnormalities such as petechial hemorrhages of the lungs, heart, or thymus; pulmonary congestion; or varying degrees of intraalveolar hemorrhage. Of the explained deaths, the majority were attributed to infectious processes [8]. Bajanowski and colleagues [5] state that 50–80% of SUDI can, after autopsy, be attributed to respiratory tract infections. Mild signs of inflammation in the upper and lower respiratory tract are often encountered [2,4,6] and are allowed in SIDS category I (genuine SIDS) according to the San Diego definition [1]. Furthermore, cases involving marked inflammatory changes or abnormalities not sufficient to be unequivocal causes of death are allowed in SIDS category II [1] (SIDS with mild abnormal findings/disease). In this retrospective study, we reviewed the histological findings of a large multicenter cohort (n = 187) dating from 1984 through 2005, with particular attention paid to signs of inflammation. Since knowledge of causes of death has increased, some cases might retrospectively be attributed to medical causes. Furthermore, we aimed to describe nonspecific histological variations in tissues from Dutch USID cases that might give a clue to the hidden causes of death.
METHODS
A multicenter retrospective study was performed to analyze histological variations and abnormalities in organs from USID in The Netherlands, with particular emphasis on infectious causes.
Case collection
First, a computer-based search using the national pathology registry (PALGA) was performed [9]. Secondly, the LWW was asked to provide an anonymous list of all reported cases that were autopsied across The Netherlands between 1996 and 2005. Subsequently, all pathology departments involved, including that of The Netherlands Forensic Institute, were contacted. A total of 200 cases diagnosed as SIDS were identified between 1984 and 2005, from which anonymous pathology reports and histology slides were made available. Furthermore, review of circumstances and clinical history had been performed for the cases dating from 1996 onward, and a statistical epidemiological study in this group has previously been published [10]. Of 103 cases, virology and bacteriology swabs were mentioned in the autopsy report. We did not have access to (pediatric) clinical files, biochemistry results, and data such as feeding habits and time of resuscitation attempt. Neither did we have access to frozen tissue.
Histology review
As this is a multicenter retrospective study extending over a long time frame, there was no common autopsy protocol, resulting in a variation in the availability of slides in individual cases. Thirteen cases were excluded from the study because of lack of slides, leaving 187 cases. In complete cases (n = 166), 1 slide each of liver, spleen, salivary gland, thyroid, pancreas, bone marrow, bladder, and tonsils was available; 2 slides each of kidneys, larynx, and esophagus, thymus, adrenals, and gastrointestinal tract were available; and 3 or more slides of heart, lungs, and the brain (if brain autopsy had been performed) were available (n = 135). Slides were reviewed by 2 of the authors (G.L. and R.K.). In thirteen cases a 2nd pathologist was asked for an expert opinion. Histological findings were divided into 3 classes, as follows: (A) an incidental finding that most likely was unrelated to death; (B) a finding that might have contributed to the demise; and (C) a cause of death. Bronchopneumonia was defined as 3 or more foci in more than 1 slide (Fig. 1), the same definition used by Valdés-Dapena and colleagues [4]. Aspiration was only considered to be the cause of death when it was present in at least 3 slides and accompanied by a lymphocytic infiltrate or by obstruction of a large bronchus. Massive vacuolization of the hepatocytes (Fig. 2) was interpreted as probable fatty acid storage disease when there were no signs of malnutrition or wasting and when vacuolization was also present in other organs [11]. Calcified Hassal's corpuscles were counted as soon as one was encountered; for starry sky macrophages several (>5) had to be seen at low magnification (×4) to create the “starry sky.” Laryngitis required lymphocyte and/or neutrophil influx with edema; denudation was not taken as a hallmark because this might have been caused by resuscitation attempt or postmortem interval. Nephrogenic rests were counted as soon as they were seen. Asphyctic bleeding was defined as extracellular blood, usually in the cortex of the adrenal gland and thymus; punctate spots of blood would be petechiae.
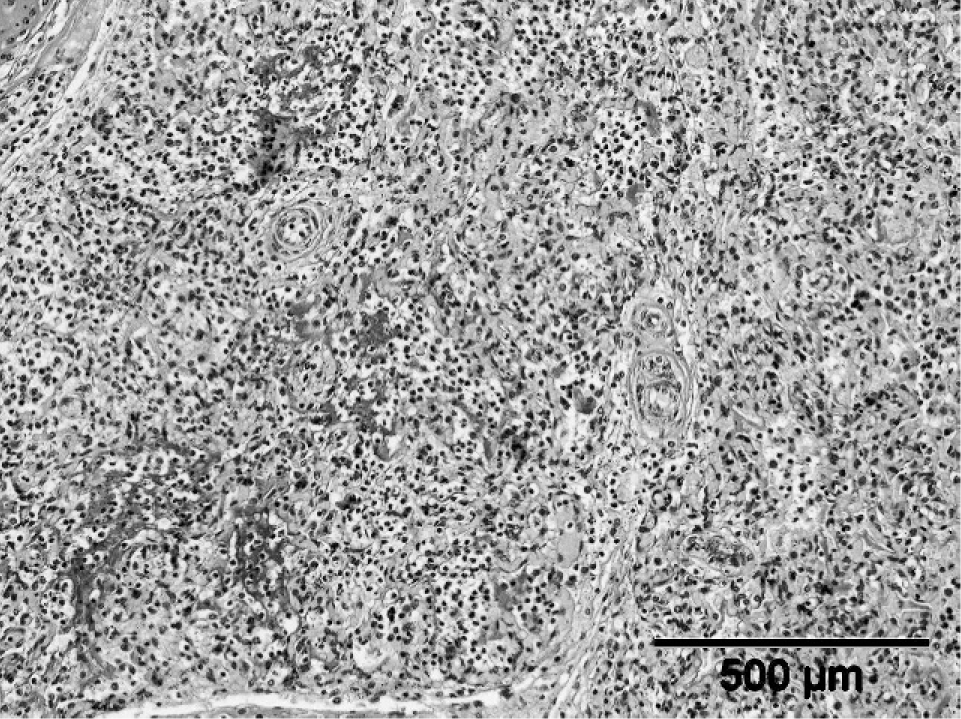
Typical example of bronchopneumonia.
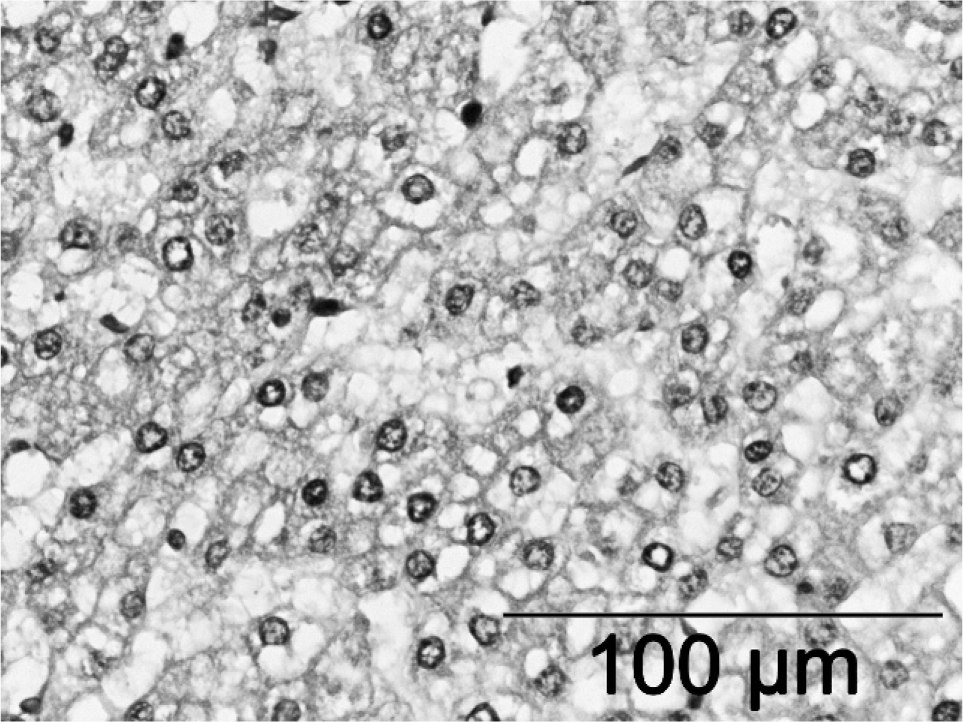
Liver with vacuolization indicative of storage disease.
Statistics
The histological findings were correlated. For statistical analysis cross-tabulations using SPSS for Windows, version 11.0.1 (SPSS Inc, Chicago, IL, USA) were made. Fisher exact test was used for the P-value.
Ethical approval
The project protocol was approved by the medical ethical committees of the Erasmus MC and 3 collaborating hospitals. All committees agreed that whenever the parents had given approval for investigation into the cause of death of their child (an autopsy), they had implicitly agreed to participate in this study, as this was a further investigation into the cause of death. Because forensic pediatric autopsies are done without parental consent, inclusion of the forensic cases in this study was done after approval of the parents, public prosecutor, or the Attorney General.
RESULTS
Approximately 43% of all alleged Dutch SIDS cases reported to the death certificate office between 1996 and 2005 were reviewed (n = 187) (Table 1). Not all cases reported to the Dutch authorities as SIDS fulfilled the San Diego criteria. By definition this group should be called USID. Every case was classified into 1 of the 3 classes described in the “Methods” section based on the most relevant histological findings (Table 2). In 90 of 187 cases (48.1%) a histological abnormality was encountered; in 19 cases (10.2%) this finding could explain death. Seven of the 135 cases with a brain autopsy had an abnormal finding in the brain (5.2%). Only 166 cases presented here had a full autopsy, of which 135 included brain autopsy. Of the 135 cases with a brain autopsy 3 were less than 1 week of age and 21 were over 1 year of age. This leaves 111 cases that fulfill the pathological part of the San Diego criteria of SIDS [1]. Of these, 63 (56.7%) had no abnormal findings, 33 (29.7%) had an incidental finding, 8 (7.2%) had a finding that might have contributed to death, and 7 (6.3%) had a finding that explained death. Of the 41 cases under 1 year of age with incomplete autopsies, 22 (53.6%) had no abnormal findings, 9 (21.9%) had an incidental finding, 5 (12.2%) had a finding that might have contributed to death, and 5 (12.2%) had a finding that explained death. All 3 cases that died in their 1st week of life were explained by massive aspiration, bronchopneumonia, and meningitis, respectively. The other 32 cases were over 1 year of age; 12 (37.5%) of these had no abnormal findings, 12 (37.5%) had incidental abnormalities, 4 (12.5%) had findings that might contribute to death, and 4 (12.5%) had a finding that explained death. There was no significant difference in subclassification of infants below and over 1 year of age (Table 3). Common findings that did not have an influence on categorization are depicted in Table 4.
Percentage of Dutch cases [3] included in the present studies

Specific findings a
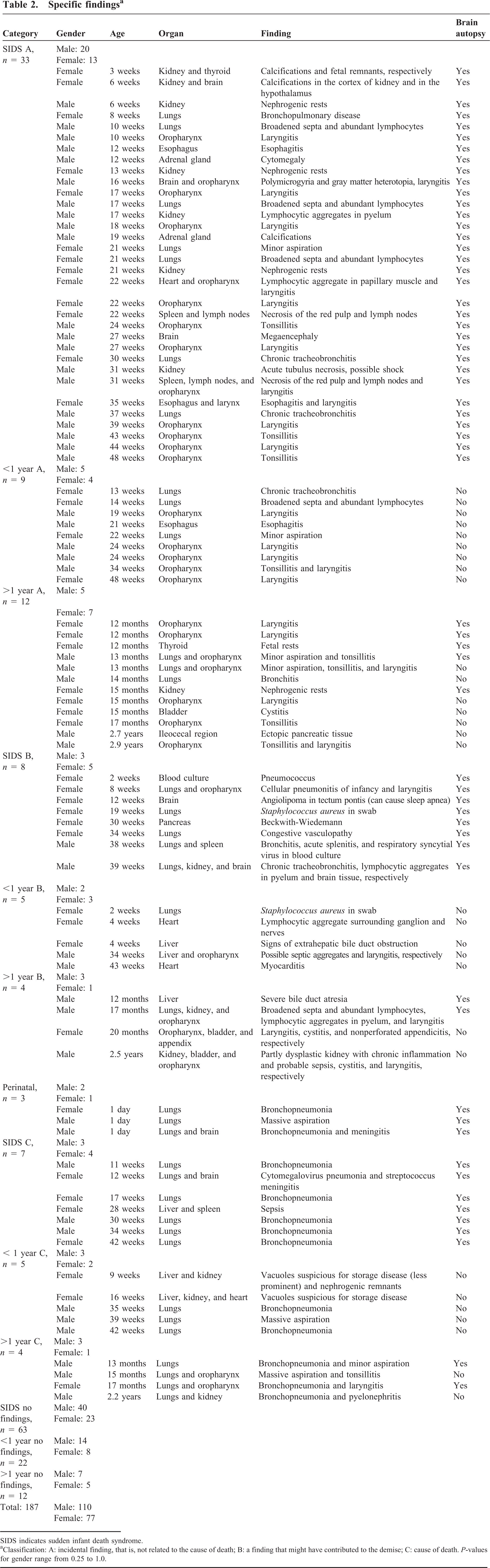
SIDS indicates sudden infant death syndrome.
Classification: A: incidental finding, that is, not related to the cause of death; B: a finding that might have contributed to the demise; C: cause of death. P-values for gender range from 0.25 to 1.0.
Subclassification of findings over different age groups a
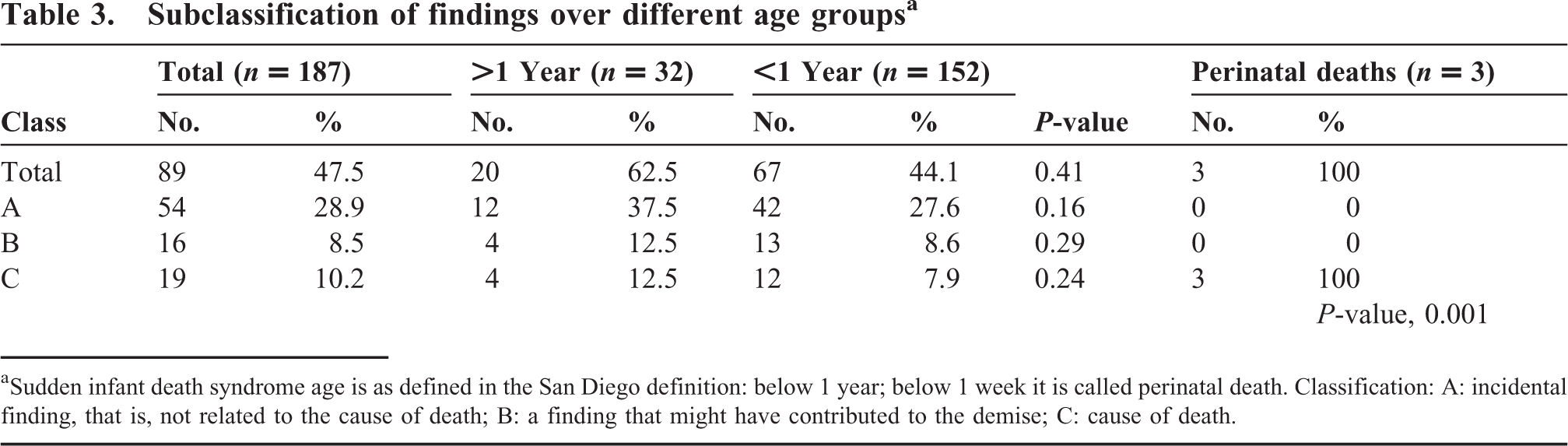
Sudden infant death syndrome age is as defined in the San Diego definition: below 1 year; below 1 week it is called perinatal death. Classification: A: incidental finding, that is, not related to the cause of death; B: a finding that might have contributed to the demise; C: cause of death.
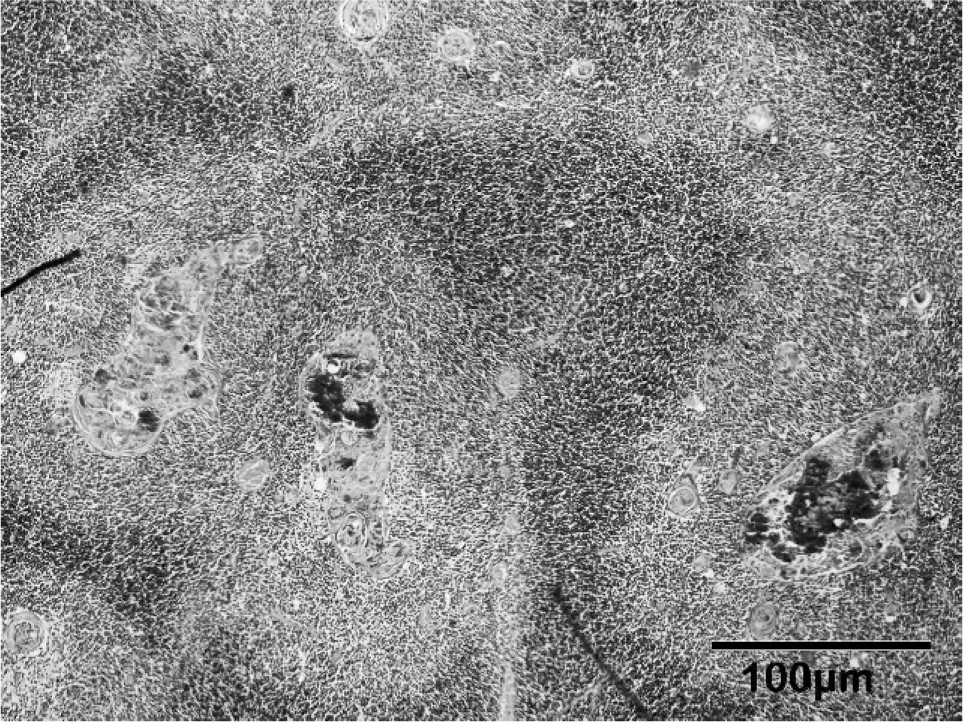
Frequently encountered histological findings that were regarded insufficient to contribute to cause of death, arranged per organ. Total number of cases investigated is 187. P-value is calculated with 2-sided Fisher exact test
Tonsillitis and laryngitis were inclusion criteria for class A, which explains their P-values.
Correlations of histological findings
Calcified Hassal's corpuscles (Fig. 3) were significantly associated with bronchopneumonia (P = 0.023) but not with infection in general (pooled lung infection, laryngitis, and tonsillitis). Notably, calcified Hassal's corpuscles were only found in cases that died below the age of 18 months (P = 0.004). Infection in general was associated with debris in the Hassal's corpuscles (P = 0.034) and with starry sky macrophages in the thymus (P = 0.004). Starry sky macrophages were not associated with debris in Hassal's corpuscles or calcification. Except for calcified Hassal's corpuscles, none of the common findings had an association with any of the categories (Table 4).
Thymus with calcified Hassal's corpuscles.
DISCUSSION
We conducted a histology review on 187 USID cases, including 111 cases that fulfill the international pathological investigation criteria for SIDS. A study on the epidemiologic data of current cases was published previously [10]. In The Netherlands an age range from birth to 3 years is accepted for SIDS. This range was defined in 1996 when the LWW was founded, 8 years before the internationally accepted San Diego definition was established. The LWW database was used in this study to gather cases, resulting in a higher percentage of cases reviewed from 1996 onward than had been reviewed prior to that year (Table 1). Physicians who report a SIDS case to the death certificate office are asked to also report the case to the LWW, but this is not mandatory. The LWW collects all information known about the cases reported to them and interviews the parents or legal custodians. Twice yearly all members of the LWW gather to categorize the recent cases. In about 40% of the cases an autopsy is lacking, because parents do not consent to one. New Dutch legislation is on its way that makes circumstance investigation, microbiological screening, radiological screening, and an autopsy mandatory for all children who die of unknown cause while below 14 years of age.
In this review we found an explanation for the death in 19 cases (10.2%) that were previously classified as USID cases. Although this may be considered a high percentage, we believe this might still be an underestimate. First, because this is a retrospective multicenter study covering the whole of The Netherlands over a large time frame, and, thus, autopsies were not performed uniformly. Second, not all slides from each case were available for review. Third, a full autopsy, including brain autopsy, was only done in 135 cases, as a result of the fact that a separate consent has to be given for brain autopsy. Finally, in only 103 cases were virology and bacteriology swabs taken. All cases that died before the age of 7 days were explained by severe infections and massive aspiration (Table 2, perinatal deaths). No statistical difference was found between cases below or over 1 year in age (Table 3). This indicates similar modes of death in both age groups. Of the 187 cases reported here, 35 (18.7%) were over 1 year of age. This yields approximately 7 times more sudden unexplained deaths in childhood (SUDC) than would be expected when looking at the incidences of SIDS and SUDC reported by Krous and colleagues [12]. They state that there were 56 SIDS cases per 100 000 living births in the United States in 2001 compared to 1.5 SUDC cases per 100 000 living births (2.7%). In 2001 the incidence of SIDS in The Netherlands was 17.5 per 100 000 living births [3]. This might indicate that in the United States infants below 1 year of age die of something Dutch infants do not die of and that the Dutch deaths in children over 1 year of age require better investigation.
Most of the newly explained cases had bronchopneumonia (n = 12), which some might consider SIDS II, according to the San Diego definition [13]. However, bronchopneumonia has also been reported [4,5,8,14] as a common cause of unexpected death in young children. In adults it is one of the most common clinically unsuspected causes of death found at autopsy [15]. Valdés-Dapena and colleagues [4], who reviewed 757 SIDS cases, found bronchopneumonia to be the cause of death when it was present in 3 or more foci in more than 1slide. We used the same criteria and regarded bronchopneumonia as a cause of death, not compatible with USID and particularly SIDS. Two cases showed massive intracytoplasmatic vacuolization of the hepatocytes in the liver and also in the tubules of the kidney and in one case the cardiomyocytes of the heart. Because the findings were present in multiple organs and there were no signs of malnutrition or wasting, we interpreted this as probable fatty acid storage disorder [11], which has been regarded as a cause of sudden death in a subgroup of USID previously [16]. Unfortunately, we did not have frozen tissue with which to confirm our suspicion with DNA tests. Both patients died before these diseases were incorporated in the national neonatal screening program in 2007 [17]. The reasons why the cases with signs of sepsis and meningitis were previously considered to represent SIDS are unknown. Two cases with positive lung swabs for Staphylococcus aureus were both less than 3 months of age and were reported by their parents to be sleepy and/or feverish. The positive swabs might previously have been dismissed because of lack of histological reaction. However, it is known that the endotoxins produced by S aureus can rapidly lead to death, and this has previously been considered as a possible cause of death [8,18]. We do not have information on the exact strands of S aureus in these 2 cases; therefore, we have regarded this as a finding that might have contributed to the demise (classification B).
Several nonspecific findings were frequently encountered. Even though a control population was not available, an effort was made to correlate these findings to other histological findings, known environmental risk factors, and demographic factors. Only an association between infectious disease and starry sky macrophages, calcification, and/or debris of the Hassal's corpuscles in the thymus was found. Starry sky macrophages are a well-known finding in stress and sudden death [4,19], and Hassal's corpuscles with debris have been found in children with severe infections or secondary immune deficiency caused by malnutrition [20]. Valdés-Dapena and colleagues [4] state that prominent Hassal's corpuscles are signs of stress or chronic disease. Calcifications were not mentioned. Lymphoid aggregates of the lungs had been described in SIDS cases before [4,5,14,21]. They have also been described in adult smokers [22]. However, we did not find an association between parental smoking, a known risk factor for USID [10], and lymphoid aggregates in the infants. It has been hypothesized [5] that these lymphoid aggregates are signs of a viral infection. In at least 103 of the present cases viral screening had been performed and no association was found. Emery and Dinsdale [23] stated that lymphoreticular aggregates are not present at birth but develop from 1 week of age and are universally present at 5 years of age. This indicates a role in immune development, which is consistent with the finding of Krous and colleagues [21], who found significantly more lymphoid aggregates in their control group compared to SIDS cases, while the mean age of the SIDS cases was 88 days and that of the controls was 210 days. In addition, Valdés-Dapena and colleagues [4] state that pulmonary lymphocyte aggregates are a normal finding in infants. The exact pathophysiology of the lymphoid aggregates remains unaccounted for.
In conclusion, in 10.2% of the reviewed Dutch USID cases an explanation for the cause of death, mainly an infectious one, was found. All cases below 7 days of age could be explained by infection and massive aspiration. No statistical difference was encountered in cases below and over 1 year, which points to shared mechanisms of death in these 2 age groups. We found that debris in the Hassal's corpuscles and starry sky macrophages in the thymus are significantly associated with infection in general and that calcified Hassal's corpuscles are associated with bronchopneumonia specifically. There-fore, when they are encountered, extra effort must be made in excluding an infection. Finally, a standardized autopsy protocol including brain autopsy is mandatory to exclude any other possible cause of death, leaving SIDS status as it should be: diagnosis by exclusion.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank the “Landelijke Werkgroep Wiegendood” (LWW), especially Guus de Jonge, Monique l'Hoir, and Adele Engelberts, for their help in case collection, and Michael den Bakker, Jan den Hollander, and Pieter Zondervan, Department of Pathology, Erasmus MC, for their expert opinions. The following pathologists are acknowledged for supplying cases: Mulder A.H., Ziekenhuis Rijnstate, Arnhem; Boorsma R., Laboratorium voor de Volksgezondheid Friesland, Leeuwarden; van der Linde J.C., Jeroen Bosch Ziekenhuis, Den Bosch; Blok P., Ziekenhuis Leyenburg, Den Haag; van der Hulsbergen-Kaa C.A., UMC St Radboud, Nijmegen; Timmer A., UMC Groningen, Groningen; Schoots S.J.F., Samenwerkende Ziekenhuizen Oost Groningen, Winschoten; ten Kate F.J., Academisch Medisch Centrum, Amsterdam; Westenend P.J., Pathologisch laboratorium voor Dordrecht en Omstreken, Dordrecht; Kwee W.S., St Jansgasthuis and Laurentius Ziekenhuis, Roermond and Weert; Willebrand D., Streeklaboratorium voor de Volksgezondheid, Haarlem; Breeuwsma R.N., Medisch Centrum Alkmaar, Alkmaar; Brinkhuis M., Laboratorium voor Pathologie Oost Nederland, Enschede; Vandevijver N.M.A., Atrium Medisch Centrum, Heerlen; Nijhuis E.W.P., Onze Lieve Vrouwe Gasthuis, Amsterdam; Baldewijns M., Academisch Ziekenhuis Maastricht, Maastricht; van Dijk C.M., Groene Hart Ziekenhuis, Gouda; de Ruijter T.E.G., Amphia Ziekenhuis, Breda; Meijers J.H.C., Stichting Pathan, Rotterdam; van Lijnschoten I., Stichting PAMM, Eindhoven; Schapers R.F.M., Pathologisch Laboratorium Noord-Limburg, Venlo; Wauters C.C.A.P., Canisius-Wilhelmina Ziekenhuis, Nijmegen; Seldenrijk C.A., Antonius Ziekenhuis, Nieuwegein; Ooms E.C.M., Haa***glanden, Den Haag; Beerman H., Maasstadziekenhuis, Rotterdam; Smits J.G., Streeklaboratorium Zeeland, Middelburg; Dutrieux R.P., Zaans Medisch Centrum, Zaandam; Croonen A.M., Lab Klinische Pathologie Centraal Brabant, Tilburg; van der Loo E.M., Reinier de Graaf Gasthuis, Delft; Arends J.W., Deventer Ziekenhuizen, Deventer; van Houten W.A., Laboratorium voor Pathologie Stichting Sazinon, Hoogeveen.