
Abstract
Electron microscopy (EM) using a “lift technique” (EM-lift) of suspect cells has been used when a question of viral infection is raised by light microscopy and is not otherwise confirmed. We demonstrate how, in this unique circumstance, EM can complement or even supersede immunohistochemistry (IHC) and culture studies. Cases with suspected viral inclusions followed by EM-lift were collected over 25 years; hematoxylin and eosin, IHC, and culture findings were reviewed. Immunohistochemistry results were not available in 15 of the 30 samples found; tissue blocks were obtained in 6 of the samples, and additional IHC studies were performed. Nine cases had viral cultures. The usual clinical question was “rejection versus infection” in a transplant setting (56%). The gastrointestinal tract/liver was most frequently sampled (76%). The EM-lift technique confirmed virus in 18 cases, including adenovirus (58%), cytomegalovirus, herpes, papillomavirus, and parvovirus. Twenty-one cases had informative EM but IHC findings were positive in 8. Both EM-lift and IHC findings were positive in 5 cases and negative in 8 cases. All IHC-positive cases were positive by EM-lift. Of the 6 cases with new IHC, 2 negative cases stained with a newer antibody (EM-positive for adenovirus) and 4 remained negative. Nine had culture findings; 1 was positive, with positive EM-lift. Eight were culture-negative; 4 of these were EM-positive. We conclude that in clinical settings in which virus identification is critical and infection is not otherwise confirmed, the lift technique can be more sensitive than IHC (missed inclusions) and culture studies (often not done) or polymerase chain reaction test, which can be overly sensitive.
INTRODUCTION
Despite the widespread use of immunohistochemical (IHC) stains in pathologic practice, virus identification remains a challenge [1–6]. In our institution, electron microscopy (EM) has been used as a diagnostic tool when a question of viral infection is raised by light microscopic observation and cannot be otherwise confirmed. We have adopted a lift technique for EM [7], with which we have been able to analyze cells that are suspected of harboring viral particles that were previously identified on hematoxylin and eosin (H&E)-stained tissue sections. Our goal was to assess the value of the EM-lift technique in these unique circumstances and also to compare its sensitivity with that of the IHC method and microbiologic studies.
METHODS
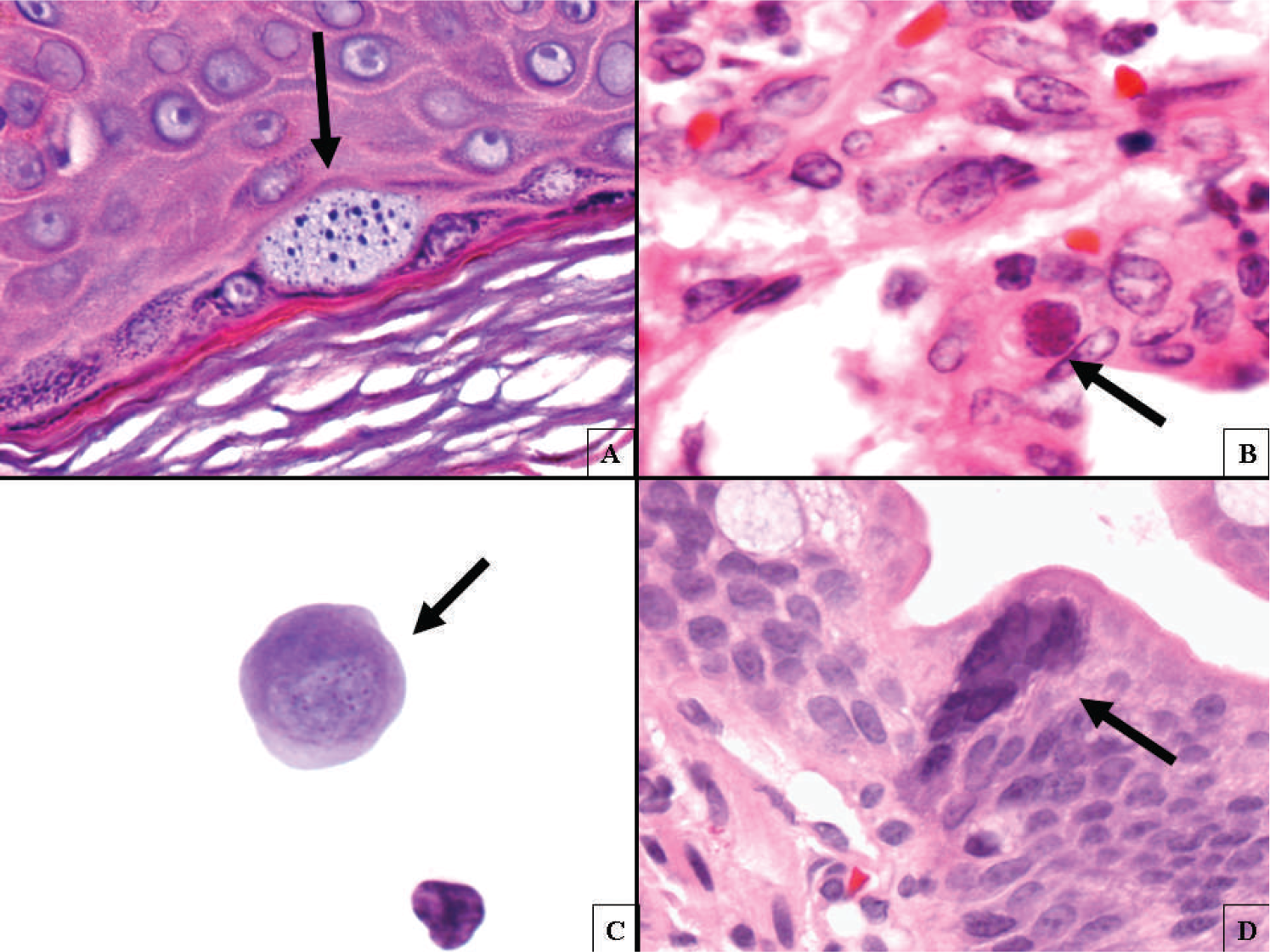
The Children's Hospital of Pittsburgh Institutional Review Board assigned an exempt-from-review status to this study. Cases with suspected viral inclusions that also had EM studies performed over the past 25 years were collected from archived files in the Department of Pathology, Children's Hospital of Pittsburgh of UPMC. The H&E-stained sections, immunostains, corresponding EM images, and, where available, the results of microbiological studies were reviewed. Electron microscopy evaluation had been done with a lift technique, in which single cells that were suspected of harboring viral inclusions were lifted from the H&E-stained glass slide [7,8]. In brief, after identifying and marking suspicious cells that may harbor virus on the H&E-stained slide (Fig. 1), we noted the area by etching the bottom of the slides and then removed the coverslips. The slides were immersed in xylene (1:1 mixture of xylene and propylene-oxide) and in pure propylene-oxide (Fischer Scientific, Fair Lawn, NJ, USA), respectively. They were then covered with a 1:1 mixture of propylene-oxide and epon-araldite for 15 minutes. This solution was wiped off the slides and a drop of epon-araldite was placed on top of the tissues. The slides were placed in the oven at 80°C for polymerization for 1 hour. The plastic-embedded tissue from the slide was then lifted with a razor blade and a small area containing the suspicious cells was marked and cut out with a razor blade. Using epoxy glue, the tissue was mounted onto a blank EM block, and followed by routine EM processing. We have used only epon-araldite as our epoxy resin component; it is possible that other resin formulations would provide similar results. Viral particles were identified by the shape and size of nucleocapsids.
In 15 cases, IHC results were not available for review, either because they were never done or the slides were not accessible. In 6 cases, tissue blocks were obtained and additional IHC analyses were performed with antiadenovirus, cytomegalovirus (CMV), and herpes simplex virus (HSV) antibodies and with an Epstein-Barr virus-encoded RNA (EBER) probe. The antibodies were purchased from the following companies: antiadenovirus and anti-CMV antibodies from Sigma-Aldrich, St. Louis, MO, USA; anti-HSV antibodies from Dako, Carpinteria, CA, USA; and antivaricella antibodies from Biodesign, Saco, ME, USA. For IHC analysis, the antigens were retrieved by enzymatic digestion with Proteinase XXIV (Sigma-Aldrich) for CMV, varicella virus; and with Trypsin (Sigma-Aldrich) for adenovirus. No antigen retrieval was used for HSV.
After incubation of the primary antibody for 30 minutes at room temperature, diaminobenzidine (DAB) (ScyTek Laboratories, Inc., Logan, UT, USA) staining was carried out with the avidin-biotin-linked peroxidase system. (ABC Kit, Vector Laboratories, Burlingame, CA, USA). All sections were counterstained with hematoxylin. In situ hybridization for Epstein-Barr virus early RNA (EBER) was performed. Formalin-fixed, paraffin-embedded tissues were probed using the Micro-probe System (Fischer Scientific, Pittsburgh, PA, USA) and a 30-base biotinylated oligonucleotide probe [9]. Positive and negative controls were run in each batch and deemed adequate. Repeat IHC analyses were done using the same methods previously described with primary antibodies purchased from the same companies. Culture study data, where available, were extracted from the patients' charts.
RESULTS
Thirty cases were identified. The age of patients ranged from 19 days to 16 years. The most frequent clinical indication for the procedure was to “rule out viral infection” in a transplant setting (56%). The gastrointestinal tract and liver were most frequently sampled (76%). Electron microscopy results were positive in 18/30 cases and 5 virus types were identified: adenovirus, CMV, herpes, papillomavirus, and parvovirus (Fig. 2). Adenovirus was the most common type found (58%). Twenty-one cases had both EM-lift and IHC results available for comparison; 38% showed positive EM results but negative ICH results. In 24% of cases, both methods had positive findings, confirming virus, and in 38% both methods were negative. All cases that were positive for viral inclusions by IHC were also positive by EM-lift. Of the 6 cases with additional IHC analysis, 2 originally negative cases stained positive with a newer antibody (both cases were EM-positive for adenovirus). The remaining 4 cases had negative findings (Table 1). Culture studies were available in 9 cases, and only 1 was positive for virus; this case had positive EM-lift. Eight cases were culture-negative; 4 were positive for virus by EM-lift and 4 were negative for EM-lift (Table 2). Microbiological tests other than cultures included a positive CMV antigenemia test. In this case, the corresponding EM showed the presence of CMV viral particles. There was 1 case with a low positive polymerase chain reaction (PCR) test result for hepatitis B virus. This case had negative findings on immunostains and EM-lift.
Electron microscopy lift technique is more sensitive than the immunochemistry method in identifying virus in this small series

Six cases had additional immunochemistry analysis with newer antibody. Two cases that originally had negative findings stained positive with a newer antibody (EM-lift was positive for adenovirus) and the remaining 4 cases were negative.
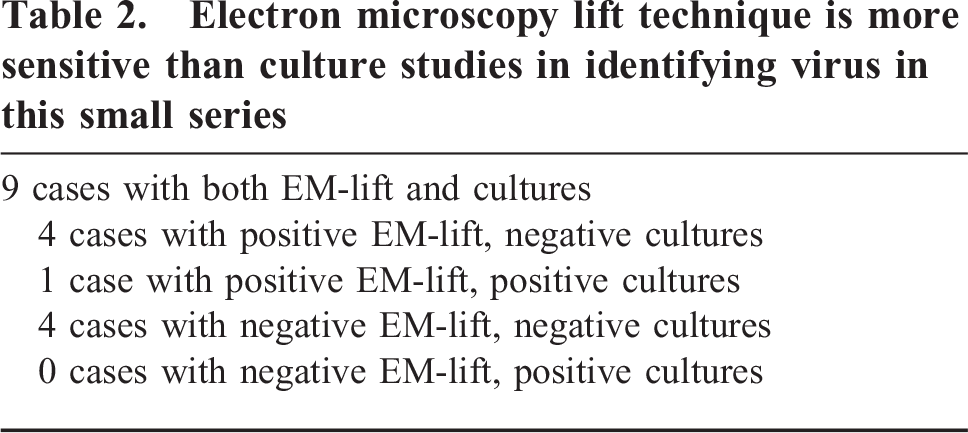
Electron microscopy lift technique is more sensitive than culture studies in identifying virus in this small series
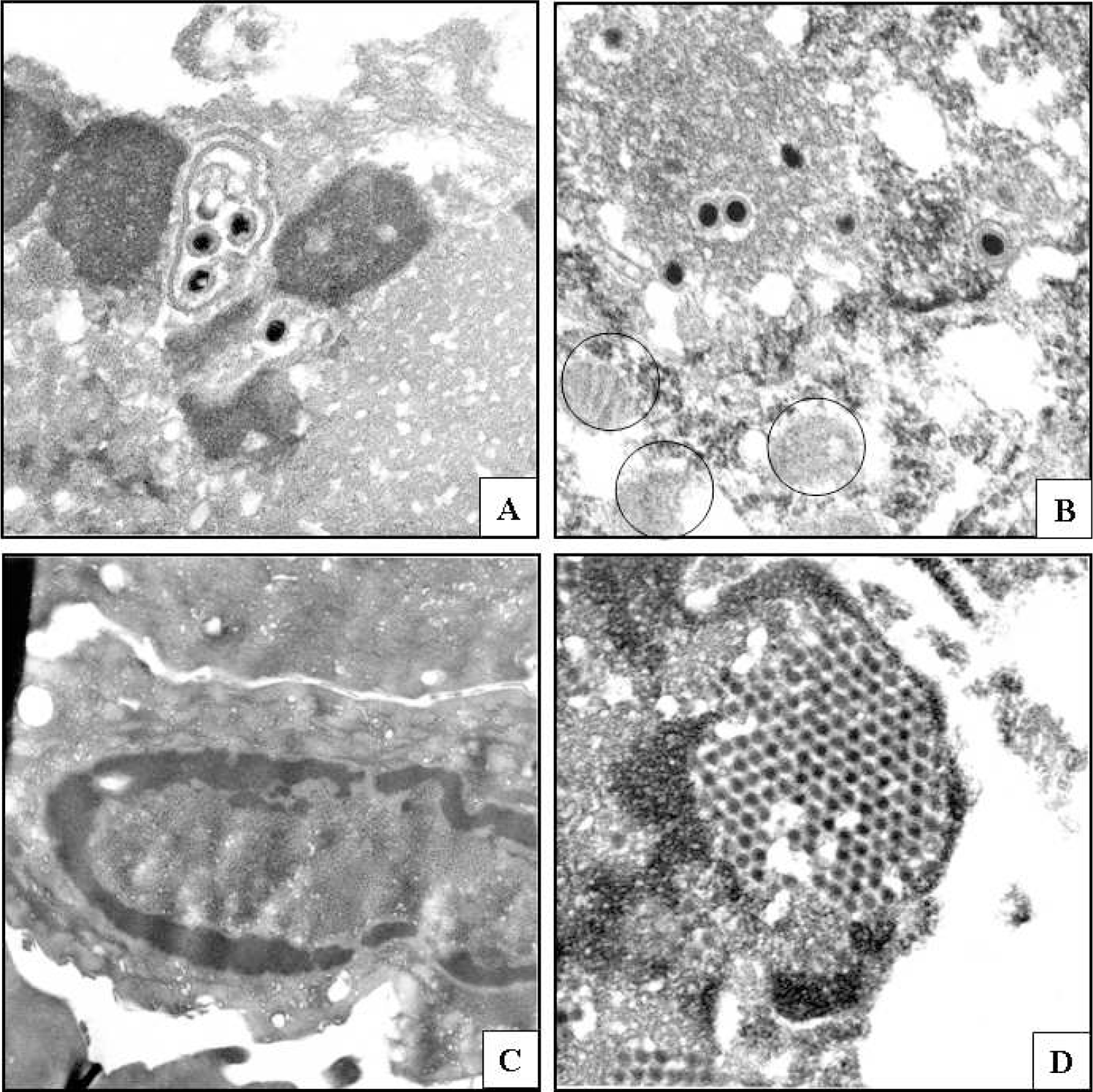
Electron micrographs of suspicious cells prepared by lift technique and showing viral particles.
DISCUSSION
Virus infection, when unidentified, could carry serious clinical consequences in many clinical settings involving immunocompromised patients [10–12]. Therefore, identification of virus is essential. Methods of virus identification include culture studies, PCR, serology, and identification of virus in tissue samples by pathologists ([7,8,11–16]). The latter is frequently performed in our institution because approximately 60% of our biopsy load involves children who receive transplants. In these cases, the most frequently asked clinical question is whether the biopsy shows rejection versus infection, especially viral infection.
Review of H&E-stained slides in many cases helps identify virus immediately because of the unique features of viral inclusions. However, there are cases in which the inclusions are less characteristic, and thus cannot be unequivocally diagnosed. Because the pathology practice has been dominated by IHC to substantiate the diagnosis, the usual order of diagnostic workup in these cases is that the H&E review is followed by confirmatory immunostaining with targeted antiviral antibodies or in situ probes. This 2-step method successfully identifies the virus in a large number of cases. However, there are circumstances in which the suspicious cell or cells identified by H&E review are no longer present in the deeper sections used for IHC; in these instances, the immunostaining is of no practical use.
To identify virus rapidly in these cases, we have used a lift technique that prepares the same tissue that was previously reviewed by the pathologist, for transmission EM study [7,8]. According to our retrospective study, this combination of techniques offers rapid and reliable virus identification. Of 30 cases reviewed, 18 showed confirmatory EM-lift results. None of the 12 EM-lift–negative cases showed positive cultures or positive IHC results. It is puzzling what theses suspicious cells of negative cases represent. One possible explanation is drying artifact, which is known to produce nuclear changes mimicking viral cytopathic effect. Another explanation may be a fibrillary effect, most likely due to fixation [17]. When the EM-lift technique was compared with the IHC technique, 8 EM-lift–positive cases initially showed negative IHC results, and no single case that showed positive IHC results had negative EM-lift results. Thus, EM-lift was more sensitive than IHC (Table 1).
We were able to repeat IHC with newer antibodies in 6 of the 8 IHC cases with negative finding that had positive findings by EM-lift. Two of the 6 cases became positive (both were cases of adenovirus infection) and 4 remained negative for virus (Table 1). Although only a limited number of cases had culture data, the EM-lift study was superior to culture studies in identifying virus. Of 30 cases, 9 had culture data available; 1 had positive findings by both EM-lift and culture study. However, of the remaining 8 negative culture cases, 4 showed positive EM-lift studies (Table 2). In addition, the EM-lift method is fast, with the shortest turnaround time of 2 days. The EM-lift images were sharp and easily interpretable, irrespective of virus type (Fig. 2) or organ from which the samples had been obtained. Although we have much less experience with viruses having helical symmetry, it is possible that identification of viruses exhibiting helical (e.g., mumps, measles) rather than icosahedral symmetry may not be as accurate.
In summary, EM combined with the lift technique is a valuable and unique diagnostic tool for pathologists to identify virus, especially in circumstances in which the rapid diagnosis of virus infection is critical and other diagnostic tests are not available. In these unique circumstances, this combination of techniques not only generates reproducible results with fast turnaround time, but also seems slightly more sensitive than IHC and culture studies. Although EM-lift appears to be more sensitive than IHC, improved antibodies and in situ probes specific to fixed viral epitopes will likely close this narrow gap.
With this technique one can also confirm the presence of inflammatory response to virus, which is not possible with either culture studies or PCR tests, which in general are extremely sensitive. Also, this technique can be performed very rapidly. This is especially important in cases of positive adenovirus test results in small bowel transplant settings, in which enteric adenovirus often does not induce tissue damage or host response and the patients do not require any change of treatment.
Footnotes
ACKNOWLEDGMENTS
The authors are grateful to the late Rocco Agostini, whose technical and diagnostic EM expertise was invaluable in all cases reviewed in this study. We thank Dr Ron Jaffe for his help in data interpretation and his critical review of the manuscript. We also thank Connie Riga, who performed the additional immunohistochemical stainings.