
Abstract
Postmortem evaluation following an in utero fetal demise is essential for determining cause of death and counseling regarding future pregnancies. Severe maceration and fetal size along with patient desires may limit the physician's ability to perform a complete autopsy. In the cases presented, we demonstrate the utility of postmortem ultrasonography as an adjunct to traditional autopsy following fetal demise.
INTRODUCTION
Examination of the stillborn fetus may provide patients and physicians with essential information regarding cause and pathogenesis of death. The willingness of parents to permit an unrestricted pathologic examination; the skill, interest, and experience of the examining pathologist, and the state of preservation of the fetus often limit the autopsy as a diagnostic procedure.
After fetal death, tissues undergo maceration and sterile autolytic enzymatic degradation. Histologic examination of the severely macerated fetus may yield little more than documentation that the tissues were autolyzed. The anatomic integrity of organs and organ systems, such as heart, lungs, gastrointestinal tract, and skeletal system, usually remains sufficiently intact to confirm appropriate or malformed anatomic relationships. Conventional autopsy approach to the examination of the central nervous system in cases of 1st and early 2nd trimester death with maceration rarely yields relevant clinical information. Due to these limitations, pathologists often rely on in utero neuroimaging studies, such as ultrasonography, to obtain information when evaluating central nervous system abnormalities at autopsy.
In this setting, postmortem (PM) ultrasonography may further evaluate in utero findings and allow for the identification of previously unrecognized malformations. Here we report 2 cases where PM ultrasonography following in utero fetal demise proved to be a valuable adjunct to the standard autopsy.
METHODS
Due to concerns for further maceration with delay, fetuses were fixed in formalin prior to undergoing ultrasonography. In each case, we obtained images of the intact fetus using a 12 megahertz linear array transducer with a GE Logiq 9 ultrasound unit (GE Healthcare, Fairfield, CT, USA). Each fetus was immersed in a water bath, and the transducer was placed at variable depths to optimize fetal imaging. Ultrasonography was performed in real time by the radiologist with the pathologist present for the scan, immediately followed by interpretation and discussion of the findings with the radiologist and pathologist. Additionally, a maternal fetal medicine specialist reviewed images after complete autopsy. Despite both fetuses being intact, imaging was focused on the fetal brain. In each case, the radiologist and pathologist felt ultrasonography served the greatest utility in evaluating cranial structures.
CASES
The 1st case was a female fetus of a 26-year-old multiparous female G4P2012 who presented at 16 weeks of gestation. A sonogram confirmed a missed abortion measuring 11 weeks by crown-rump-length. The mother underwent a spontaneous abortion prior to any further in utero evaluations. The fetus was obtained by the pathology department 12 hours after delivery and underwent fixation upon receipt to prevent further tissue degeneration.
At autopsy, foot length confirmed the antemortem estimate of fetal age [1]. The fetus had cyclopia, a proboscis, and arrhinia suggestive of holoprosencephaly (Fig. 1) and bilateral ectrodactly with 3 fingers on the right hand and 2 on the left (“lobster claw malformation”). X-ray examination demonstrated normal forearm bones. There was polysyndactyly of the left foot with 7 toes (duplication and fusion of toes 2 and 3) and partial syndactyly of the right foot involving toes 1 and 2.
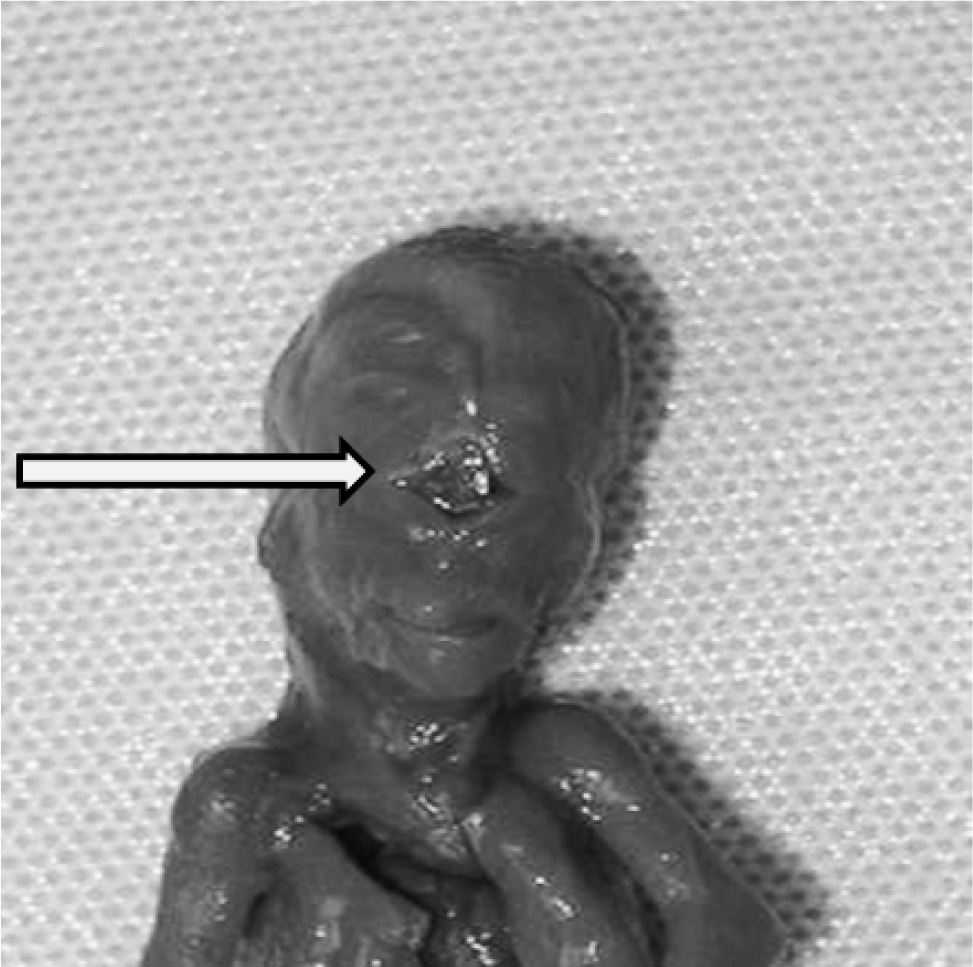
Case 1: Autopsy image of fetal face demonstrating cyclopia (arrow), a proboscis, and arrhinia.
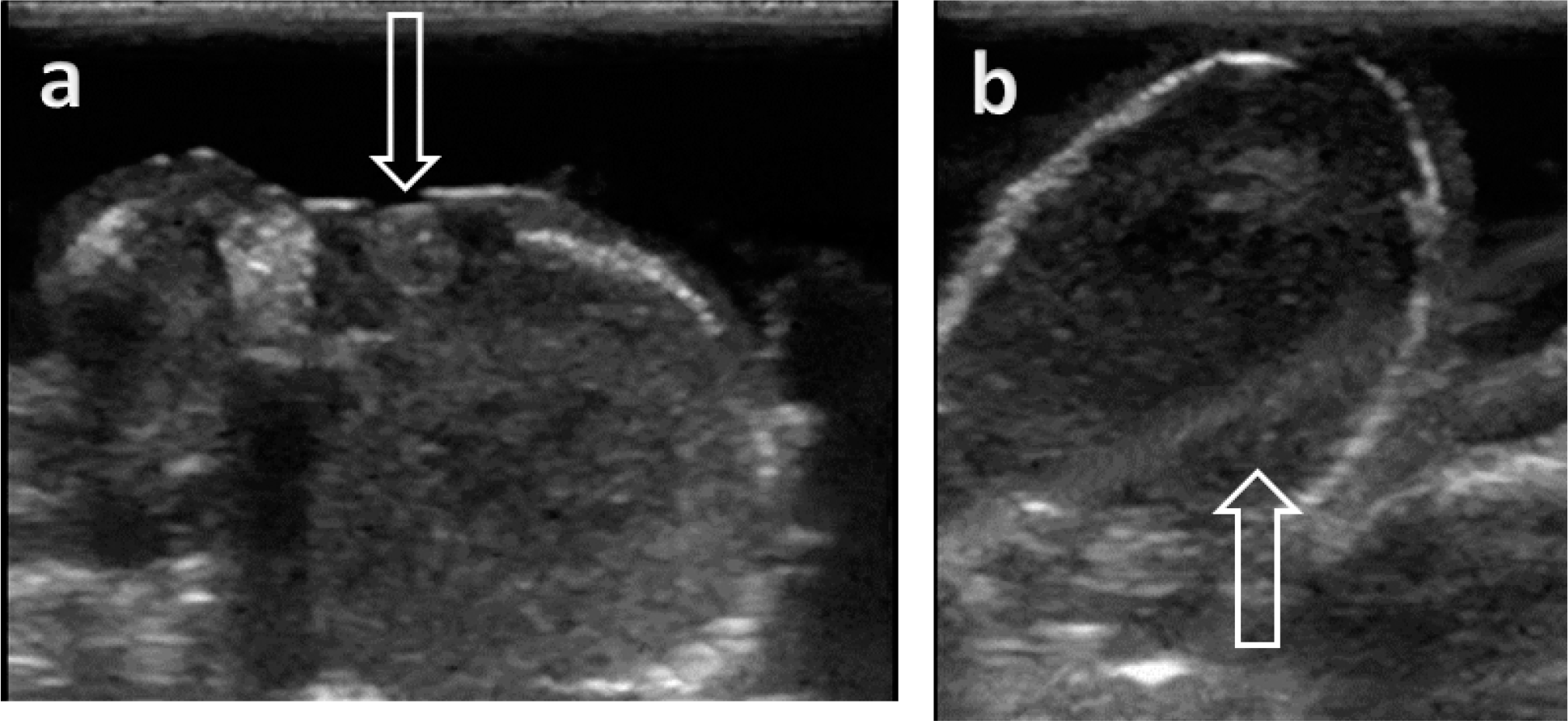
Postmortem ultrasonography examination of the intact cranium demonstrated holoprosencephaly with single undivided brain and a clearly visible single globe (Fig. 2A,B). Due to prior fixation, the timing of ultrasonography depended on availability of both teams and not fetal tissue degeneration. Ultrasonography occurred greater than 36 hours after delivery with full autopsy after completion of imaging. Upon removal of the brain, an underdeveloped anterior cranial fossa was observed, as is usually seen with holoprosencephaly (compared to the normal base of skull seen in case 2), and extensive maceration precluded further anatomic or histologic examination. Final analysis of placental tissue revealed a karyotype of 47, XX, +13. The hand anomalies observed in this case are seen in about 5% of cases of trisomy 13 [2]. Trisomy 13 accounts for 25% of all holoprosencephaly cases and up to 75% of those associated with aneuploidy [3,4].
Case 1: Postmortem fetal brain.
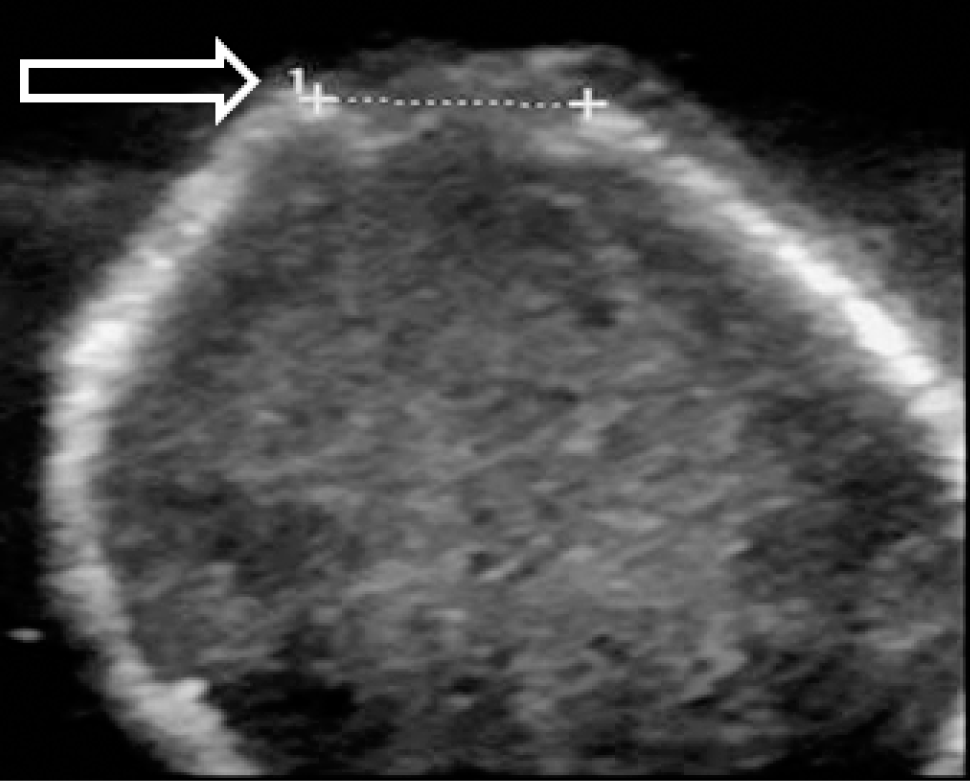
The 2nd case was a male fetus of a 31-year-old multiparous female at 17 weeks of gestation. The patient was referred to our facility due to suspected cystic hygroma. Upon presentation, she was diagnosed with fetal demise, measuring 13 weeks by crown-rump-length. At the time of diagnosis of fetal death, an occipital skull defect suggestive of an encephalocele was noted on the in utero sonographic images (Fig. 3). Amniocentesis for chromosome analysis was performed at the time of this ultrasound as part of a further investigation into the cause of death due to a high suspicion for genetic abnormality.

Case 2: Transverse sonographic image of fetal brain in utero with suspected posterior encephalocele (arrow).
After induction and delivery, pathology received an intact fetus 16 hours after delivery. As in case 1, formal fixation occurred upon receipt of the fetus to prevent further tissue degeneration. Autopsy revealed a macerated fetus with foot length consistent with a gestational age of 12–13 weeks [1]. The fetus had upslanting palpebral fissures, an enlarged tongue, a flattened nose, a right foot syndactyly, a plantar crease of the left foot, and underdevelopment of the external genitalia. Any further evaluation was precluded by severe maceration.
The back of the head was examined closely in light of the prenatal observations of possible encephalocele. Autopsy demonstrated a flattened macerated head, loosened skin, and widely separated cranial bones without evidence of an encephalocele or any other process, such as a cystic hygroma (Fig. 5). Radiology and pathology completed PM ultrasonography more than 24 hours after delivery. Comparison of the in utero and PM ultrasound images revealed the extent to which the bones of the occipital skull were separated and what appeared to be associated soft-tissue edema, thereby facilitating a more complete correlation with the prenatal findings and query of a possible occipital defect (Figs. 3,4). Autopsy showed a normal skull base but did not permit anatomic or histologic evaluation of brain due to maceration. A PM diagnosis of trisomy 21 was made by a fluorescent in situ hybridization aneuploidy screen on PM, paraffin-embedded formalin-fixed tissue due to failure of amniocytes to grow in culture.
Case 2: Postmortem transverse sonographic image of fetal brain with widely spaced sutures (arrow) and no evidence of encephalocele.
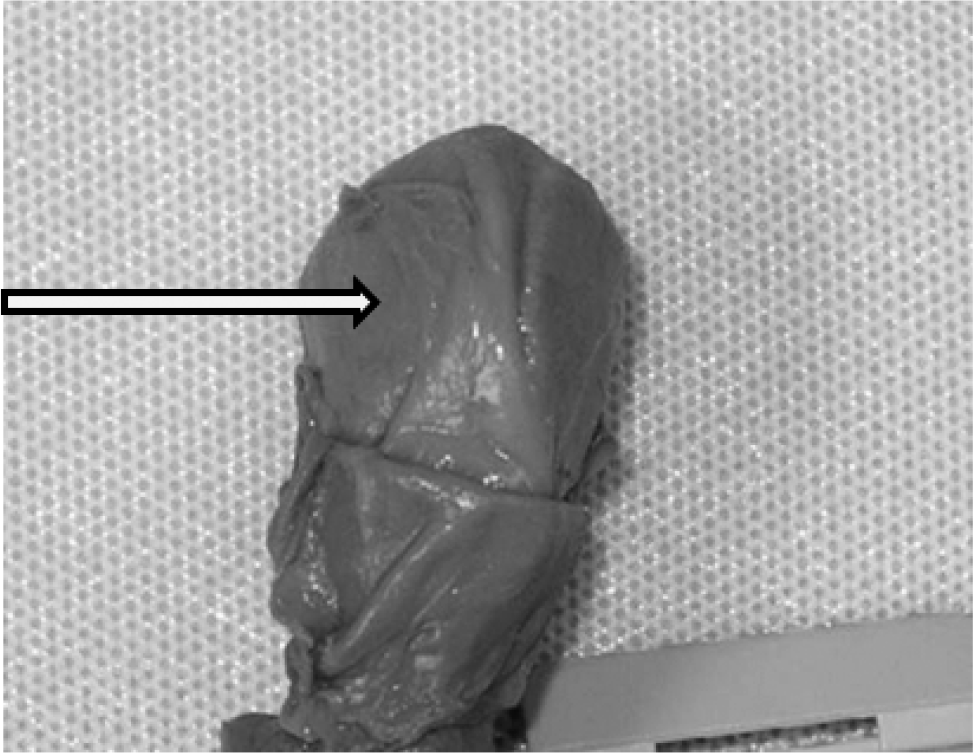
Case 2: Autopsy image of fetal occiput demonstrating widely spaced sutures (arrow).
DISCUSSION
These cases illustrate the value of ultrasonography of the central nervous system after early fetal loss. In both cases, the time interval between in utero death and its clinical recognition was more than 4 weeks. The length of time between death and autopsy led to severe maceration, limiting anatomic and histologic evaluation of the fetal brain. In each case, PM ultrasonography served as an adjunct to traditional autopsy.
Ultrasonography confirmed the presence of holoprosencephaly based on external examination in case 1. In the 2nd case, a lack of identifiable anatomic abnormalities in combination with the PM ultrasound findings clarified and correlated the antenatal and postnatal findings.
Prior reports have described PM imaging as an adjunct to autopsy [5–7]. Radiographs can be utilized in examining skeletal development and dysplasias [8]. Postmortem computed tomography (CT) allows visualization of fractures and 3-dimensional reconstruction of anatomy. Griffiths and colleagues found that magnetic resonance imaging (MRI) of the central nervous system agreed with autopsy in 28 of 32 cases in which both procedures were performed [6]. Thayyil and colleagues reviewed the current evidence and practical issues associated with PM imaging by MRI and CT noting that these methods are particularly useful in the PM evaluation of the central nervous system [9]. The same group found a concordance of minimally invasive autopsy (including postnatal MRI, blood sampling, clinical history review, and external evaluation) and conventional autopsy of 94.9% (95% CI 91.7–97.0) among 277 cases of fetal demise [5].
In the 2 cases presented here, we found ultrasonography a useful adjunct rather than a replacement of the standard autopsy. Postmortem ultrasonography of the central nervous system can clarify a diagnosis in cases of early fetal death accompanied by severe maceration. Although whole body PM MRI and CT may be superior to ultrasonography for fetal evaluation, cost and the need for technical support may limit their routine use. Ultrasonography has lower cost and is widely available in most hospital settings. This imaging method can optimize PM diagnostic information and correlate ante- and postnatal observations, given the routine use of ultrasonography for a prenatal screening. In cases in which autopsy is restricted due to time, personal, or religious reasons, ultrasonography may also be used for directed biopsies of abnormal tissues (eg, polycystic kidneys) [10].
The diagnosis and management of missed abortion and fetal death are difficult for the patient and practitioners involved. The emotional nature of the diagnosis and treatment, financial cost, and religious beliefs may prevent consent to traditional autopsy or genetic evaluation. In these cases, minimally invasive autopsy, including ultrasonography, may offer information regarding etiology of demise and can guide recurrence risk counseling. Each of the cases presented here highlights the value of a comprehensive PM evaluation regardless of fetal size or maceration. Postmortem ultrasonography may resolve prenatal diagnostic questions and the status of central nervous system phenotypes. Postmortem phenotypic refinement through imaging can refine the search for genetic syndromes and chromosomal abnormalities. Confirming the presence of holoprosencephaly (case 1) and focusing the differential diagnosis (case 2) guided further testing and patient counseling. Similar to PM skeletal surveys, PM ultrasonography should be viewed as an adjunct to PM evaluation that can be offered to patients as an inexpensive and noninvasive method of obtaining supplemental information regarding the cause of death. Future research investigating the most appropriate methods for PM ultrasonography, including performance pre- vs post-formalin fixation would further increase the utility of this diagnostic tool.
Footnotes
ACKNOWLEDGMENT
The authors wish to thank Professor John M. Opitz for his critical review of this manuscript.