
Abstract
Many 3rd-trimester stillbirths are unexplained, including the time course of the illness. Histologic acute thymic involution (ATI), when graded, correlates with duration of acute illness (grade 0, <12 hours; grade 4, >72 hours). Histologic brain injury is also common in stillbirth. We investigated ATI in unexplained stillbirth and correlated it with neuropathologic injury by identifying 58 autopsies of unexplained, 3rd-trimester stillborns (preterm, n = 24; term, n = 34) that included brain examination and graded ATI from 0 (resting state) to 4 (pronounced lymphodepletion). Gray matter injury (GMI) and white matter injury (WMI) were classified as older, recent, or absent, and ATI was correlated with GMI, WMI, thymic weight, and clinical data. Nine cases (16%) had ATI grade 0–1; 19 (33%), grade 2; 24 (41%), grade 3; and 6 (10%), grade 4. Older GMI and WMI were present in 39 (67%) and 10 (17%) stillborns, respectively. Higher ATI grade correlated significantly with older GMI (P < 0.001) and WMI (P = 0.014). The ATI grade was higher in the small-for-gestational stillborns compared with the appropriate- or large-for-gestational stillborns (P = 0.017) but did not correlate significantly with gestational age or other clinical or demographic factors evaluated. The ATI grades 2–4 were found in 84% of the stillborns, consistent with onset of acute illness between 24 and >72 hours before demise. Higher ATI grade correlated significantly with older brain injury, suggesting similar time of onset and shared underlying pathophysiologic events, the specific nature of which remains unclear.
INTRODUCTION
The evaluation of stillbirth includes detailed and meticulous fetal autopsy and placental examination [1–3]; however, many stillbirths remain unexplained despite thorough investigation, particularly in late pregnancy [4]. Causality in stillbirth is difficult to determine because, although many medical conditions and placental pathologies have been linked to stillbirth, most cannot be classified as unequivocal causes of death [2]. The biologic pathways and molecular mechanisms leading to stillbirth are uncertain, and so is the understanding of time course of illness. Histologic acute thymic involution (ATI) can occur in response to any form of acute stress, and it has been shown to correlate with duration of acute illness in neonatal and pediatric cases, making it a useful parameter in the estimation of such timing [5,6].
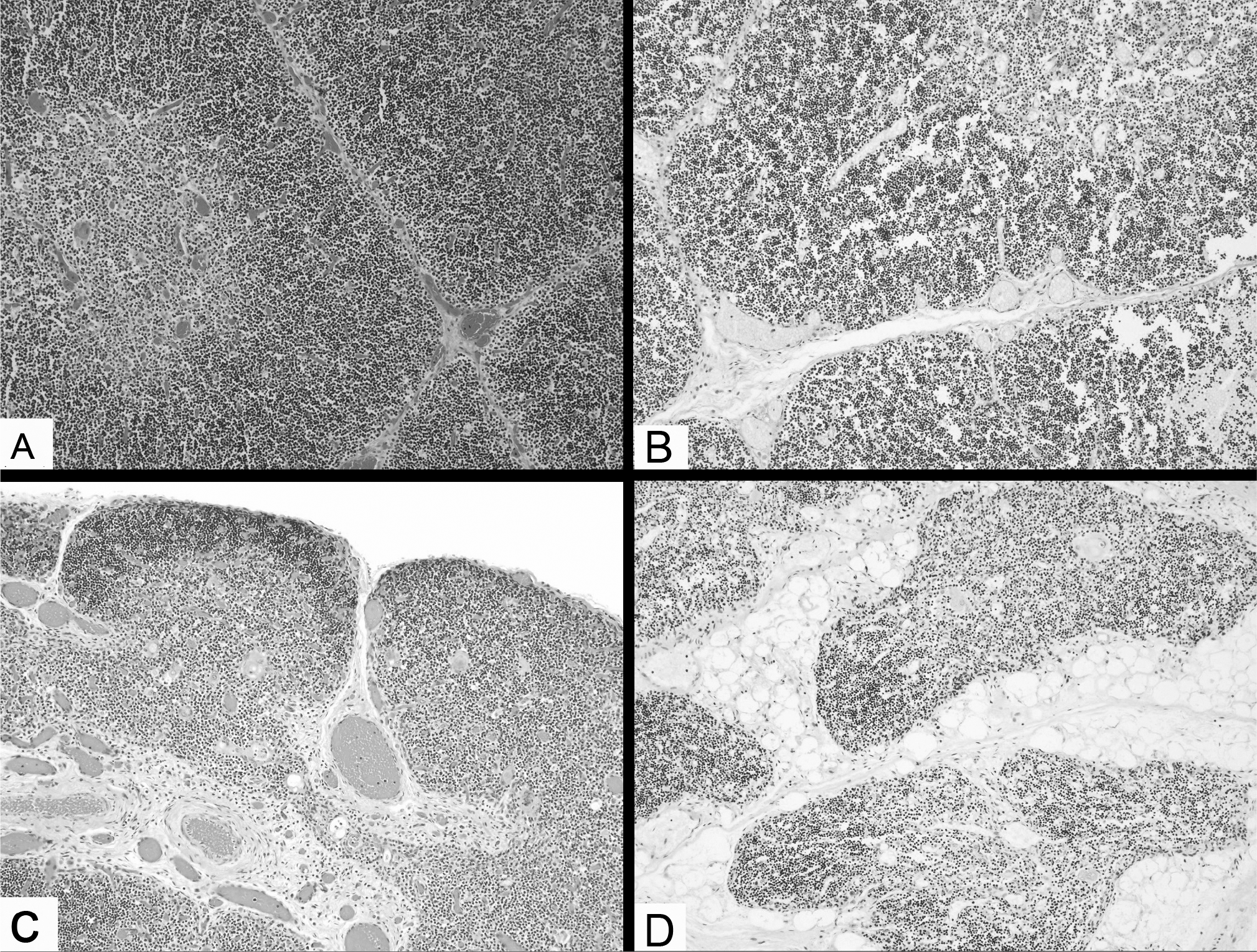
Van Baarlen and colleagues [5] graded ATI on a 5-point scale based on the appearance of cortical macrophages (starry sky pattern), increase in interlobular interstitium, and lymphodepletion of the cortex and estimated the duration of acute illness in time intervals of 12 hours, with ATI grade 0 correlating significantly with disease duration of 0–12 hours, and ATI grades 2, 3, and 4 correlating significantly with disease duration of 24–48, 48–72, and >72 hours, respectively. They also noted that thymic histology did not undergo further change after 72 hours of onset of ATI, limiting the use of ATI grading in cases with longer disease duration [5]. Evaluation of the thymus is an established part of the fetal autopsy, and although it is known by perinatal pathologists that these thymic changes are frequently present in stillborns [1,7], there are only infrequent reports investigating ATI and its associations in stillbirth [8,9].
Gray matter injury (GMI) and white matter injury (WMI) are also frequent findings in 3rd-trimester stillbirth [10–12]. We have previously reported brain injury in 88% of 51 cases of unexplained 3rd-trimester stillbirth, with the most common form of brain injury being karyorrhectic neurons [12]. The documentation of neuropathologic injury preceding the period immediately before demise may also be useful in the understanding of the time course and mechanism of acute illness in stillbirth.
In this study, we report the distribution of thymic weights and histologic grades of ATI in a series of 58 autopsies of unexplained, 3rd-trimester stillbirths. This study correlates ATI with clinical and demographic features, including gestational age, birth weight, and small-for-gestational age (SGA) compared with appropriate-for-gestational age/large-for-gestational age (AGA/LGA) stillborns. This study further compares histologic ATI grade with histologic GMI and WMI.
MATERIALS AND METHODS
Records of autopsies performed at Hutzel Women's Hospital, Detroit, MI, from 2006 to 2013 were searched to identify singleton stillborn fetuses delivered at 28 weeks estimated gestational age (EGA) or later with complete autopsies, including brain examination, and documented intrauterine fetal demise at the time of the mother's hospital admission. Fetuses with conditions considered unequivocal causes of death, such as placental abruption or ruptured vasa previa, were excluded, as were fetuses with severe anomalies or genetic syndromes. Fetuses delivered to legal minors were also excluded, in accordance with the exclusion criteria approved by the institutional review board.
Fifty-eight autopsies fulfilling the inclusion criteria were identified, which were divided into 3 subgroups based on EGA (preterm, 28 to <32 weeks EGA; preterm, 32 to <37 weeks EGA; and term, 37–41 weeks EGA). Fetuses were classified as SGA or LGA if the weight was less than the 10th percentile or greater than the 90th percentile for the EGA, respectively [13]; this was based on the birth weight, which has been shown to be more accurate than the weight obtained at time of autopsy [14]. The medical records of Hutzel Women's Hospital were reviewed for each case.
All autopsies were performed by 2 perinatal pathologists (F.Q. and S.M.J.), and the brain was examined jointly by the perinatal pathologists and a neuropathologist (W.J.K.). All autopsies were performed in a manner consistent with established guidelines [1]. Specifically, the thymus was removed in toto and weighed, and a section was taken for microscopic examination. Histologic ATI was graded on a scale of 5, as previously described by van Baarlen and colleagues [5] (Fig. 1). Grade 0 was defined as the resting state with clear corticomedullary distinction, high density of lymphocytes in the cortex, and closely packed thymic lobules separated only by delicate connective tissue septa. Grade 1 was defined as identical to grade 0, except for the presence of some lymphophagocytosis in the cortex. Grade 2 was defined by more-pronounced lymphophagocytosis (starry sky pattern), and there could also be early signs of shrinkage of the cortex and early separation of the thymic lobules. Grade 3 was defined by loss of cortical medullary distinction at low magnification, advanced lymphophagocytosis with irregular narrowing of the cortex, and increasing separation of thymic lobules. Grade 4 was defined by more-pronounced lymphodepletion of the cortex and loss of distinction between the cortex and medulla, higher lymphocyte density in the medulla than in the cortex, and prominence of interstitium and blood vessels with advanced shrinkage and separation of thymic lobules. Autolysis hampered assessment of the changes seen with ATI grade 1 (early lymphophagocytosis); therefore, grades 0–1 were combined for analysis. The histology sections were independently reviewed by the perinatal pathologists without knowledge of the clinical history or neuropathologic findings. In cases of discordance, the histology was jointly reviewed to reach agreement.
The brain was sectioned following formalin fixation, and sections examined included frontal lobe, occipitoparietal lobe, temporal lobe with hippocampus, basal ganglia and thalamus, cerebellum, pons, and other brainstem levels (midbrain and medulla). The classification of GMI and WMI used in this study was based on those previously used in studies of brain injury in stillbirth [10–12]. The GMI was classified as older (neuronal necrosis with karyorrhexis, commonly in the subiculum or basis pontis), recent (red neurons without older GMI), or absent. The WMI was classified as older (periventricular leukomalacia with necrosis or gliosis), recent (reactive glial changes or edema without older WMI), or absent. The brains could have either GMI or WMI, both GMI and WMI, or neither GMI or WMI Injury was classified as recent only in the absence of older injury because GMI and WMI appear to be ongoing processes with older injury frequently accompanied by more-recent injury. Hemorrhages were limited predominantly to a few fresh petechial hemorrhages, subarachnoid hemorrhages, or germinal matrix hemorrhages and were not considered in the analysis. None of the autopsies included spinal cord examination.
Neuropathologic findings were previously reported in 51 of the 58 stillborns (88%), along with placental findings and detailed criteria for diagnosis of placental lesions [12]. Placentas from the additional 7 patients were available for gross and microscopic examinations.
Data were analyzed using SPSS Statistics for Windows version 20 (IBM Corporation, Armonk, NY, USA). Normally distributed, continuous data were analyzed using analysis of variance (ANOVA) with Student-Newman-Keuls post hoc tests and Student t-tests. Nonnormally distributed, continuous data were analyzed using nonparametric Kruskal-Wallis ANOVA, Mann-Whitney U-tests corrected for multiple comparisons, and Spearman rank-correlation coefficient. Categorical data were analyzed with Pearson chi-square test and Fisher exact test. All significance tests were 2-tailed, and a P < 0.05 was considered statistically significant.
RESULTS
Of the 58 cases identified, 9 (16%) had ATI grade 0–1; 19 (33%), grade 2; 24 (41%), grade 3; and 6 (10%), grade 4. Grading of the ATI was only minimally hampered by autolysis, with the exception of the identification of early lymphophagocytosis in ATI grade 1, resulting in the combination of grades 0 and 1 for analysis. In general, across the ATI grades, the starry sky pattern was inconspicuous, and grading was based predominantly on narrowing of the cortex and separation of the lobules by interstitial connective tissue (Fig. 1). The inconspicuous nature of the starry-sky aspect may be due, in part, to autolytic changes but may also reflect the immaturity of the study population.
Correlation of ATI grade with EGA and clinical and demographic factors
Twenty-four fetuses (41%) were term (37–41 weeks EGA), and 34 (59%) were preterm (17 fetuses, 28 to <32 weeks EGA; 17 fetuses, 32 to <37 weeks EGA). There was no significant difference in ATI grade among the EGA subgroups (P was not significant [NS], Kruskal-Wallis test; data not shown). The comparison of clinical and demographic factors in the EGA subgroups is shown in Table 1. Diabetes was more common in the term fetuses compared with the preterm fetuses (P = 0.010); otherwise, there was no significant difference in maternal age, gravity, parity, frequency of hypertensive disorders in pregnancy, SGA fetuses, or fetal gender among the EGA subgroups. Comparison of ATI grade in SGA vs AGA/LGA stillborns demonstrated higher ATI grade in the SGA stillborns (P = 0.017) (Table 2). Correlation of other clinical and demographic factors with ATI grade did not reveal significant differences (Table 3). Fifty (86%) of the mothers stated their race as African American, 5 (9%) declined to specify a race, and the remaining 3 (5%) gave their races as white, Hispanic, or Middle Eastern. Prenatal body mass index was not evaluated in this study because that information was not available for most of the mothers.
Clinical and demographic characteristics and thymic weight in the estimated gestational age (EGA) subgroups
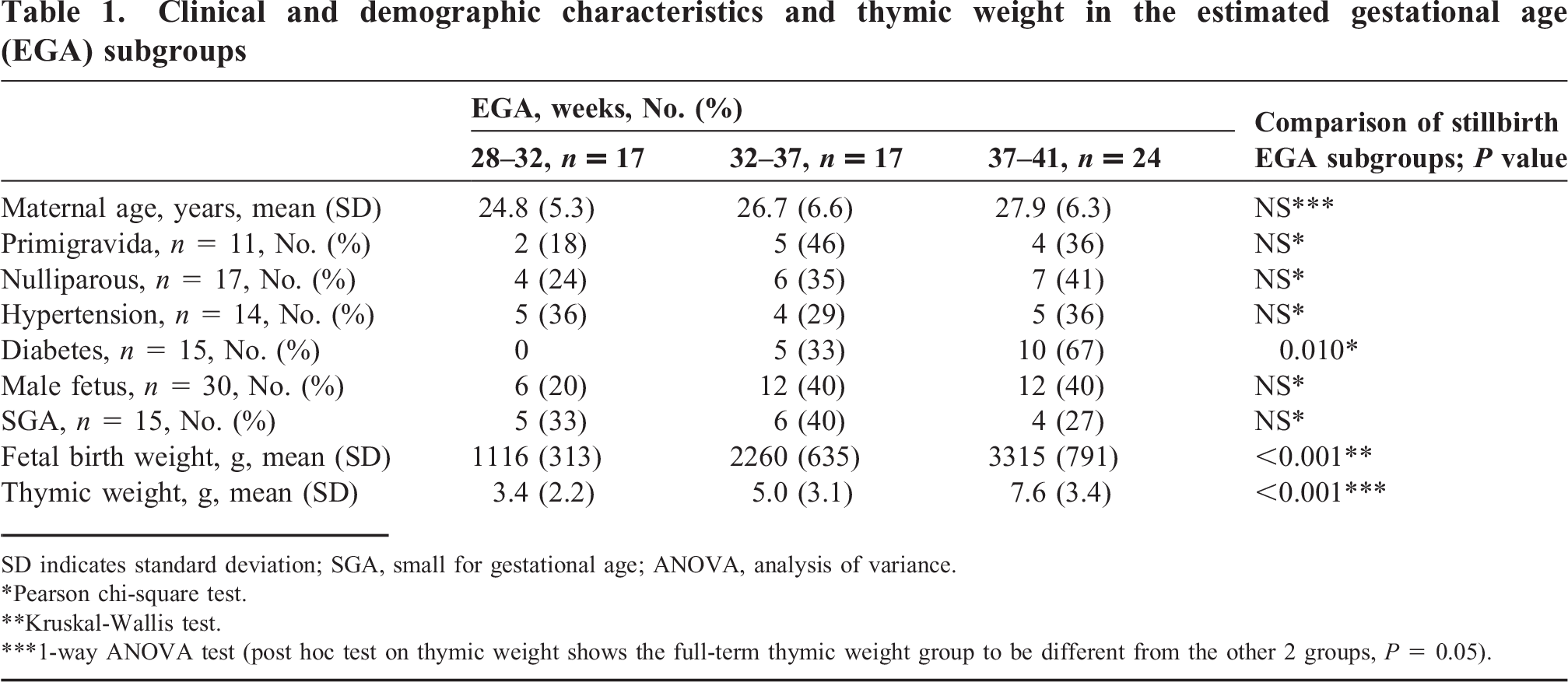
SD indicates standard deviation; SGA, small for gestational age; ANOVA, analysis of variance.
Pearson chi-square test.
Kruskal-Wallis test.
1-way ANOVA test (post hoc test on thymic weight shows the full-term thymic weight group to be different from the other 2 groups, P = 0.05).
Comparison of acute thymic involution (ATI) grade in small-for-gestational-age (SGA) versus appropriate-for-gestational-age/large-for-gestational-age (AGA/LGA) stillborns
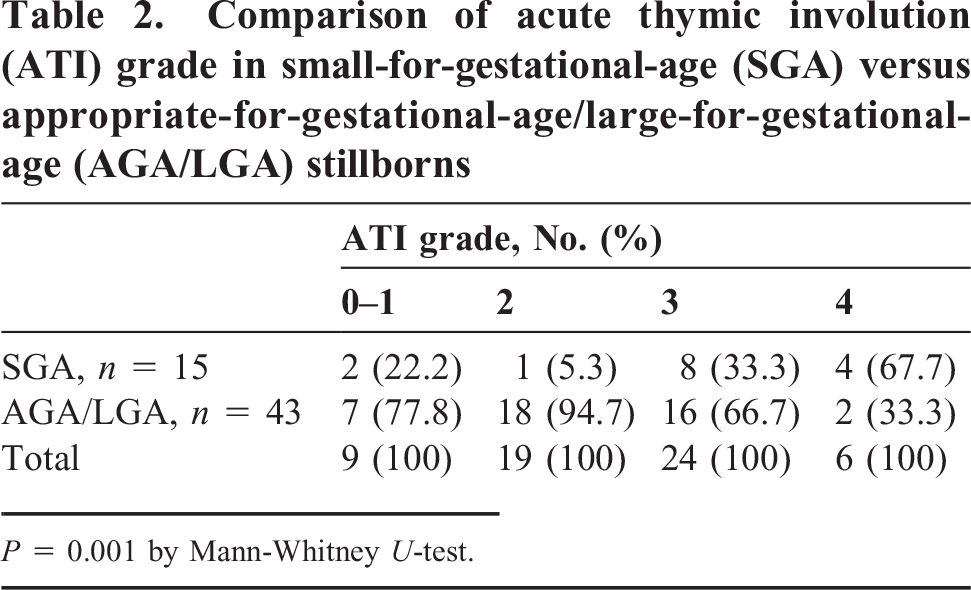
P = 0.001 by Mann-Whitney U-test.
Correlation of clinical and demographic characteristics and thymic weight with acute thymic involution (ATI) grade
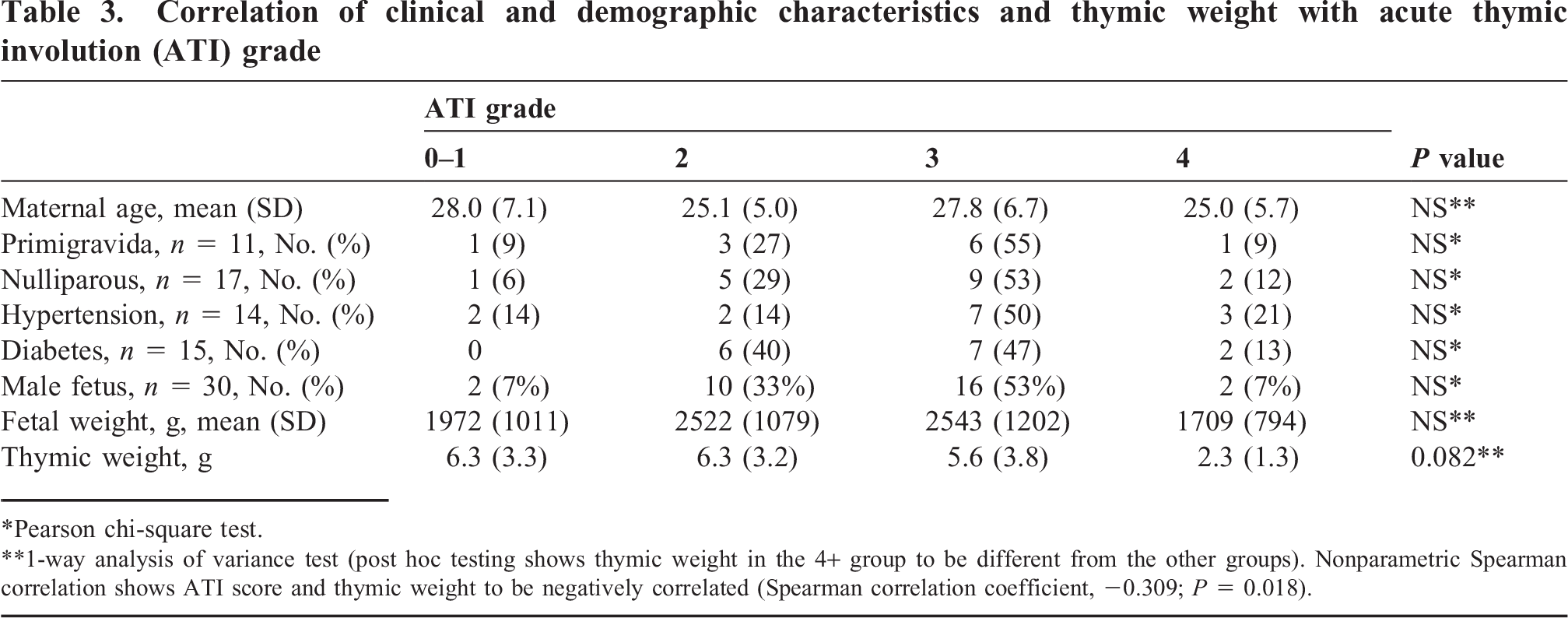
Pearson chi-square test.
1-way analysis of variance test (post hoc testing shows thymic weight in the 4+ group to be different from the other groups). Nonparametric Spearman correlation shows ATI score and thymic weight to be negatively correlated (Spearman correlation coefficient, −0.309; P = 0.018).
Correlation of ATI grade with fetal and thymic weight
Average fetal birth and thymic weights showed an expected increase with increasing EGA (Table 1). The thymic weight decreased with increasing ATI grade, and although not statistically significant, there was a trend (P = 0.082) (Table 3). Post hoc testing showed the thymic weight in the ATI grade-4 group to be different from the other groups, and nonparametric Spearman correlation showed score and weight to be negatively correlated (Spearman correlation coefficient −0.309) (P = 0.018).
Correlation of ATI grade with neuropathologic injury
Thirty-nine fetuses (67%) exhibited older GMIs, 8 (14%) recent GMIs, and 11 (19%) no GMIs. Ten fetuses (17%) exhibited older WMIs, 15 (26%) recent WMIs, and 33 (57%) no WMIs. The correlation of GMI and WMI is shown in Table 4. The GMI was seen more frequently than the WMI was, and there were no fetuses with older WMIs that did not also exhibit older GMIs. Only 6 fetuses (18%) exhibited neither GMI nor WMI.
Correlation of gray matter injury (GMI) with white matter injury (WMI)

The correlation of ATI grade with GMI (Table 5) demonstrated higher ATI grade in the presence of older GMIs (P < 0.001) (Kruskal-Wallis test). Specifically, 28 of the 30 stillborns (93%) with ATI grade 3 or 4 had older GMI, compared to 1 of 9 (11%) stillborns with ATI grade 0–1. Per Mann-Whitney testing, ATI grade in the older GMI group was significantly different compared with the absent GMI (P < 0.001) and recent GMI groups (P = 0.001), but there was no significant difference in ATI grade in the absent compared to recent GMI groups. Each of the 6 stillborns with ATI grade 4 exhibited older GMIs (Table 5).
Comparison of acute thymic involution (ATI) grade with gray matter injury (GMI)
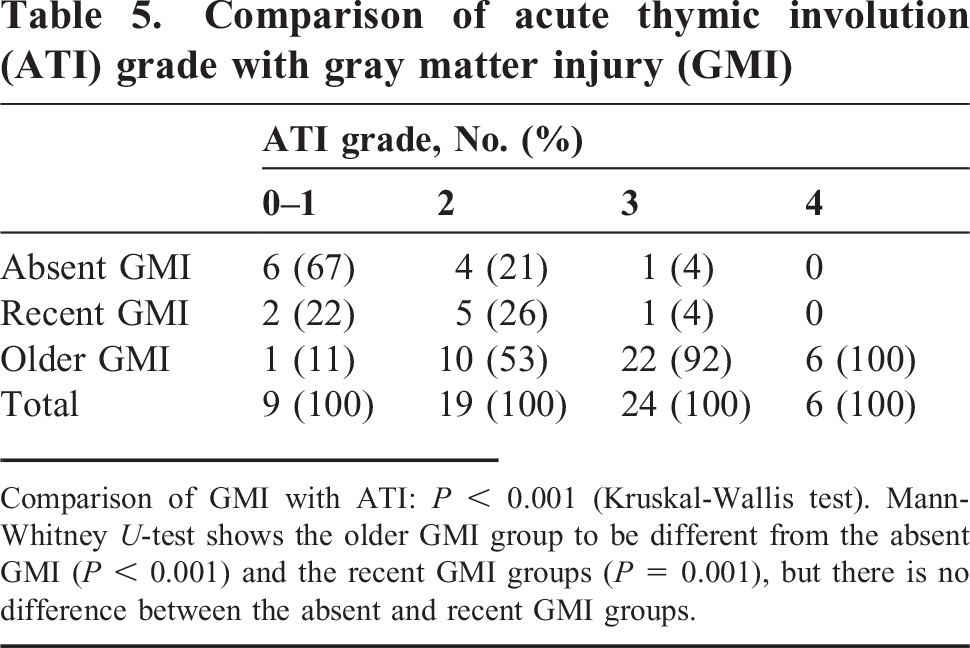
Comparison of GMI with ATI: P < 0.001 (Kruskal-Wallis test). Mann-Whitney U-test shows the older GMI group to be different from the absent GMI (P < 0.001) and the recent GMI groups (P = 0.001), but there is no difference between the absent and recent GMI groups.
The correlation of ATI grade with WMI (Table 6) also demonstrated higher ATI grade in the presence of older WMI (P = 0.014) (Kruskal-Wallis Test). Specifically, 9 of the 30 stillborns with ATI grade 3 or 4 had older WMI, compared to 0 of 9 stillborns with ATI grade 0–1. Per Mann-Whitney testing, ATI grade in the older WMI group was significantly different compared with the absent WMI group (P = 0.009), but there was no significant difference in the ATI grade in the absent compared with the recent WMI group or between the recent and the older WMI group. Three of the 6 stillborns with ATI grade 4 exhibited older WMIs, and 2 exhibited absent WMIs (Table 6).
Comparison of acute thymic involution (ATI) grade with white matter injury (WMI)
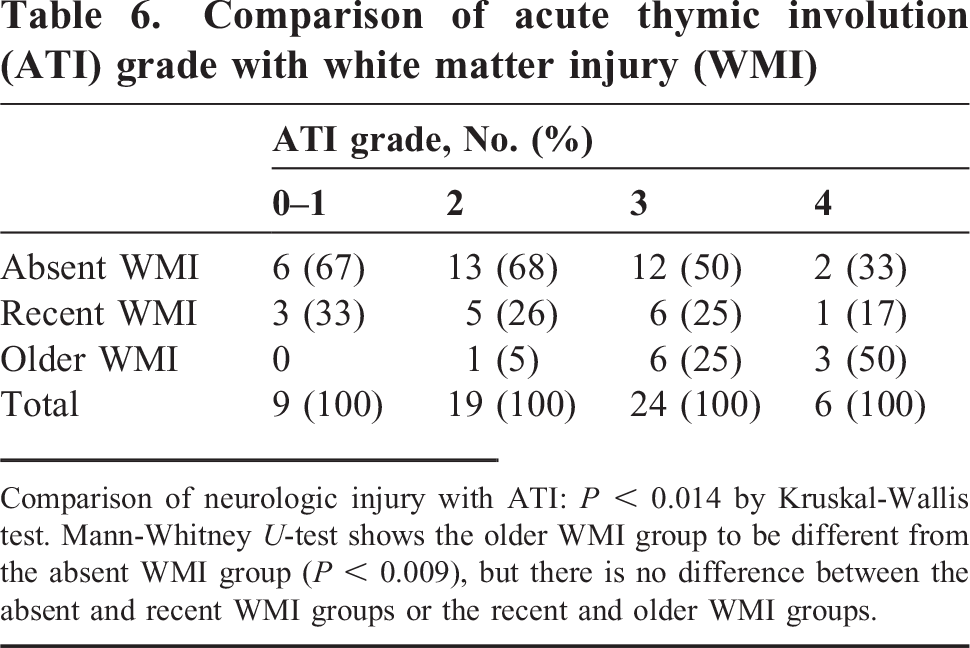
Comparison of neurologic injury with ATI: P < 0.014 by Kruskal-Wallis test. Mann-Whitney U-test shows the older WMI group to be different from the absent WMI group (P < 0.009), but there is no difference between the absent and recent WMI groups or the recent and older WMI groups.
Placental pathology
The placental findings were previously reported in 51 of the 58 stillborns and included predominantly mixed and relatively mild lesions, and no significant correlation between placental lesions and brain injury was demonstrated [12]. No severe or high-grade placental inflammatory lesions were seen in the additional 7 cases in this current series. Acute maternal inflammatory lesions were seen in 14 placentas (grade 1, n = 11; grade 2, n = 3); only 3 of these had accompanying acute fetal inflammatory response (acute funisitis or acute chorionic vasculitis). Chronic chorioamnionitis was present in 18 placentas, villitis of unknown etiology in 8 (high grade in 1), and chronic deciduitis in 13; these chronic inflammatory lesions were frequently seen in combination, and 27 placentas had one or more chronic inflammatory lesions. Villous or vascular lesions associated with maternal vascular underperfusion were seen in 30 placentas, including 6 with severe lesions (5 with extensive infarcts, in each case involving >30% of the placenta, and 1 with distal villous hypoplasia). Villous or vascular lesions associated with fetal thrombo-occlusive disease were seen in 9 placentas, including 7 with severe lesions (6 with large vessel thrombi and 1 with fetal thrombotic vasculopathy). Two of the 58 placentas had narrow umbilical cords, 2 had marginal cord insertion, and 1 had a single umbilical artery and a loose true knot. Three stillborns had a history of nuchal cord. Cord length and coiling were not evaluated in this study because, frequently in our institution, <30 cm cord is received with the placenta.
Findings pertinent to cause of death
Although none of the stillborns in this series had an unequivocal cause of death, the placental findings, autopsy findings, and maternal medical conditions during pregnancy were examined to identify possible or probable causes of death based on INCODE (initial causes of fetal death) [3]. Fourteen mothers had hypertensive disease during pregnancy, and 15 had diabetes during pregnancy, but these conditions were not considered possible or probable causes of death if they are well controlled and seen in isolation [3]. In the 28 to <32 weeks EGA subgroup, 7 of 17 cases had possible or probable causes of death identified as follows: 3 mothers had hypertensive disease with associated SGA stillborns, 2 of those also had extensive placental infarcts, and 1 had thrombi of large fetal vessels in the placenta; 1 additional mother had hypertensive disease and abnormal development of villous parenchyma (distal villous hypoplasia); 2 additional SGA stillborns had extensive placental infarcts, and 1 also had anhydramnios; and 1 stillborn had histologic acute chorioamnionitis and funisitis. In the 32 to <37 week EGA subgroup, 5 of 17 cases had possible or probable causes of death identified as follows: 1 mother had hypertensive disease with an associated SGA stillborn; 1 mother had an SGA stillborn and oligohydramnios, also complicated by histologic acute chorioamnionitis and funisitis; 2 mothers had diabetes during pregnancy, 1 described clinically as poorly controlled, and the second with fetal islet cell hyperplasia, and the latter case was also complicated by histologic acute chorioamnionitis and acute chorion vasculitis; and 1 stillborn had thrombi of large fetal vessels in the placenta. In the 37 to <41 week EGA subgroup, 13 of 24 cases had possible or probable causes of death identified as follows: 2 mothers had hypertensive disease associated with SGA stillborns, 1 also had extensive placental infarcts; 6 mothers had diabetes during pregnancy that was described clinically as poorly controlled or was associated with diabetic ketoacidosis, fetal islet cell hyperplasia, or an LGA stillborn; 4 stillborns had thrombi of large fetal vessels in the placenta, and 1 SGA stillborn had fetal thrombotic vasculopathy. None of the mothers had a record of heritable thrombophilia, antiphospholipid syndrome, or other documented maternal or fetal hematologic condition, and none had uncontrolled asthma, a clinically symptomatic thyroid disorder, renal disease, or other medically significant condition. None of the mothers or stillborns had infections proven by cultures or polymerase chain reaction.
DISCUSSION
This retrospective study demonstrated ATI grades 2–4 in 49 of 58 (84%) of the stillborns, consistent with onset of acute illness more than 24 hours before demise and aiding in ruling out the possibility of a catastrophic event of sudden onset as a cause of death. It is notable that only 6 (10%) of the stillborns had ATI grade 4, indicating that the duration of acute illness in most stillborns was less than 72 hours. The nature of this acute illness is not known, and it could be any pathophysiologic process severe enough to cause ATI and was possibly superimposed on chronic illness of longer duration or on cumulative injury requiring multiple days' duration to result in death. If SGA is considered a surrogate for fetal growth restriction that results from chronic processes, then the finding of ATI grades 2–4 in 13 of 15 SGA stillborns but ATI grade 4 in only 4 of them supports an acute process of <72 hours duration superimposed on a chronic pathologic process. Higher histologic ATI grade also correlated significantly with older GMIs and WMIs, but although each of the 6 stillborns with ATI grade 4 had older GMIs, only 3 of them had older WMIs, and 2 had no WMIs. This suggests that GMI and WMI might have different pathways and tissue-specific susceptibility/sensitivity to various injuries. Fetal death has multiple etiologies and can include different pathophysiologic pathways, and histologic ATI and brain injury are not specific for any single cause of stillbirth.
The histologic grading of ATI in this current study is based on that of van Baarlen and colleagues [5], who evaluated thymic weight and histologic changes in 234 patients, ranging from 20 weeks EGA to 17 years old, who died following a short period of acute illness of known duration. They demonstrated that histologic grading of the thymus was the best parameter to estimate the duration of acute illness in individual cases. Noting that thymic weight is highly age dependent, they concluded that weight was of little value in the assessment of the duration of acute illness; however, they did demonstrate that thymic weight was significantly less in ATI grade 4 compared with lower grades, similar to the findings in this study. Because the study group used by van Baarlen and colleagues [5] did not include stillborns, its use in the setting of stillbirth must be viewed with caution, and it should not be considered the gold standard for timing of ATI in stillbirth.
In one of the few studies evaluating ATI in a series of stillborns, Agapitos and colleagues [8] evaluated thymic changes in 300 cases of perinatal death, including 121 stillborns (“normally formed macerated stillborns”), and classified involutional changes as starry-sky pattern or as intense lymphocyte depletion. They found intense involutional changes in 34 stillborns, starry-sky pattern in 30, and a healthy thymus in the remaining 57 cases [8]. Their findings are similar to ours in that most of the stillborns showed ATI, but their findings differ in that a higher percentage of stillborns in their study showed a healthy thymus. They also reported a correlation between thymic weight and histologic features but no correlation between thymic histologic features and EGA, also in accordance with our findings [8]. Another recent series of 10 fetuses and neonates expiring close to the time of delivery, including some with intrapartum demise, found ATI grades 2–4 in 7 cases, also similar to the findings in our study [15].
Toti and colleagues [9] studied histologic ATI in 20 fetuses and 10 neonates with histologic chorioamnionitis, reporting that histologic chorioamnionitis induces thymic modifications and shrinkage. Glavina-Durdov and colleagues [6] examined histologic ATI in 100 neonates dying in the intensive care unit and found not only that ATI grade correlated with duration of acute illness but also that placental inflammation and infection as a cause of death were connected to advanced histologic ATI. In live-born, very low birth weight, preterm infants, radiographic studies have shown that a small thymus is associated with histologic chorioamnionitis [16] and is predictive of bronchopulmonary dysplasia [17]. Sonographic studies have demonstrated small thymic size to correlate with postnatal infection in preterm neonates [18], histologic acute placental inflammation in preterm labor [19], and preterm premature rupture of membranes [20]. That ATI is nonspecific is supported by its identification with inflammation in the above studies, and now, seemingly, with hypoxia/ischemia in the current study.
The type and frequency of brain injury observed in the stillborns in this current series is similar to that described in other series of 3rd-trimester stillborns [10,11]. The cause of the brain injury is not clear, and hypoxia/ischemia and infection/cytokines have been proposed as the basis for brain injury in the perinatal period [21]; however, hypoxia/ischemia is favored by many investigators based on associated placental lesions and fetal growth restriction [10,22–26]. The timing of the brain injury in humans is difficult to determine; therefore, the brain lesions in this series were divided into the broad classification of older and recent. Karyorrhectic neurons most likely indicate injury at least 1–2 days old [10,27]. Although the difficulty in interpreting neuropathologic findings by their timing and temporal relationships [27] and the absence of a good animal model for the study of human fetal brain injury in the setting of specific placental lesions have been noted [10], insights can be gained from animal studies. Classic studies performed on monkeys by Myers [28] led him to suggest that most perinatal brain damage in humans was the result of prolonged partial asphyxia, with the degree of injury correlating with the degree of insult, and with visible damage occurring possibly as early as the first half hour of injury. In studies of reduced uterine blood flow performed in sheep, early neuronal injury could by identified as early as 6–12 hours following the insult [29]. These studies suggest that the recent GMIs described in our study may have occurred very close to the time of fetal demise, possibly within hours. That GMI and WMI may have different pathways is supported by experiments in mice [30]; however, in multiple animal models, hypoperfusion led to both GMI and WMI [31]. The difficulty in interpreting and timing neuropathologic findings is also complicated by the possibility that the injury was the result of a combination of insults or that the insults might be intermittent, allowing for periods of recovery and repair. Correlation of brain injury with other autopsy findings, such as thymic involution, may allow insight into not only events preceding fetal demise but also their timing.
In this study, we demonstrate a correlation between ATI grades 3 or 4 (consistent with a duration of acute illness >48 hours) and older GMIs (karyorrhectic neurons), which supports a duration of injury of approximately the same length of time for those older GMIs. Few studies explored the possibility of a relationship between brain injury and ATI, and those that did were performed in neonates [32,33]. Neonates who died with cerebral WMIs were shown to be more likely to have ATI than were those dying without WMIs [32]. A radiographic study in living preterm neonates showed that those with early onset postnatal ATIs were more likely to develop WMIs, as defined by an echolucency, suggesting the possibility that the ATI and neonatal WMI are not independent phenomena but have common antecedents [33].
Most mothers in our study were African-American (86%), and although this study highlights morbidity associated with African-American mothers, the conclusions may apply only to this ethnic group. There is a higher rate of stillbirth in African-Americans than in whites [34–36]. Although the explanation for that difference is not known, possible reasons include disparity in socioeconomic status, limited access to medical care, and higher rates of maternal medical disorders, including hypertension and obesity [34]. Further study is required to determine whether the high frequencies of ATI and brain injury reported in this study are related to ethnicity.
Weaknesses of this study include the lack of a control group and knowledge by the pathologists that all cases were from stillborns, potentially leading to bias in the search for subtle lesions. Cases with unequivocal causes of death could potentially supply a control group, and an area of future research could involve comparison of findings in unexplained stillbirths to those from stillbirths with unequivocal causes of death, perhaps shedding light on common pathways of tissue injury and providing information about tissue-specific patterns of injury. Timing of injury in human stillbirth is difficult, and data collected from animal studies or from studies of live-born neonates, such as the criteria of van Baarlen and colleagues [5] for timing of ATI, may not apply as well in human stillbirth. Another weakness involves the autolytic changes seen with stillbirth, potentially hampering histologic evaluation; however, because all autopsies included brain examination, severely macerated fetuses were excluded. Strengths include the blinding of the pathologists reviewing the thymic histology to other autopsy findings, as well as the examination of all cases in a standard fashion by the same team of experienced pathologists, resulting in consistency of tissue sampling and the application of well-defined criteria for microscopic diagnosis.
In conclusion, in this retrospective study of 3rd-trimester stillborns predominantly from African-American mothers, we found ATI grades 2–4 in 84% of the cases, consistent with the onset of acute illness >24 hours before demise, as based on the criteria of van Baarlen and colleagues [5] for timing of ATIs. The finding of ATI aids in the exclusion of an isolated catastrophic event of sudden onset as a cause of death; however, the ATI may result from an acute process superimposed on an underlying chronic illness of longer duration or on cumulative injuries requiring multiple days' duration to result in death. Fifteen (26%) of the stillborns were SGA, and they demonstrated higher ATI grades than did the AGA/LGA stillborns, but only 4 (27%) of the SGA stillborns demonstrated ATI grade 4, supporting an acute process of <72 hours' duration superimposed on a chronic pathologic process. The significant correlation of higher histologic ATI grade with older histologic GMIs and WMIs, suggests that these lesions may have a similar time of onset and shared pathophysiologic processes, the nature of which remains unclear. Fetal death has multiple etiologies and can include different pathophysiologic pathways, and histologic ATI and brain injury are not specific for any single cause of stillbirth.