
Abstract
NRAS and BRAF mutations occur in congenital melanocytic nevi (CMN), but results are contradictory. Sixty-six prospectively collected CMN patients were analyzed for NRAS Q61 mutations using Sanger sequencing. Negative cases were evaluated for BRAF V600E mutation. NRAS Q61 mutations affected 51 patients (77.3%), and BRAF V600E was found in 5 (7.6%). NRAS Q61 mutation affected 29 (80.6%) of 36 giant, 16 (80.0%) of 20 large, and 5 (62.5%) of 8 medium-size CMN; BRAF mutation affected 1 (5%) of 20 large and 4 (11.4%) of 36 giant CMN. Compared to NRAS, BRAF-mutated nevi show scattered/extensive dermal and subcutaneous nodules (100% BRAF+ vs 34.8% NRAS+) (P = 0.002). Neurocutaneous melanocytosis (NCM) affected 16 (24.2%) of 66 patients, with NRAS Q61 mutation in 12 (75.0%), and BRAF V600E in 2 (12.5%), P = 0.009. Two patients were negative for both mutations (12.5%). In conclusion, although NRAS Q61 mutations predominate, BRAF V600E mutation also affects patients with large/giant CMN (L/GCMN), and with NCM, a novel finding. BRAF V600E is also associated with increased dermal/subcutaneous nodules. These findings open the possibility of BRAF-targeted therapy in some L/GCMN and NCM cases.
Keywords
INTRODUCTION
Congenital melanocytic nevi (CMN) are neural crest–derived proliferations of nevomelanocytes originating in utero. Congenital melanocytic nevi above 10 cm in diameter occur in 1∶20 000 newborns [1]. Those greater than 40 cm (or expected to reach that size in adulthood) affect 1 per 500 000 newborns [2]. Complications of large/giant CMN (L/GCMN) include decreased sweating, xerosis, pruritus, and skin fragility; altered or diminished tissue growth due to the hamartomatous and infiltrative nature of the lesions; higher complexity of surgical removal; and childhood psychological problems secondary to cosmetic issues and stigmatization [2]. Furthermore, patients with L/GCMN also have a small but increased lifetime risk (<5%) of malignant transformation in the nevi [3–5] and they also are at risk for neurocutaneous melanocytosis (NCM), a neurological syndrome with multiple abnormalities [6].
Neurocutaneous melanocytosis, a rare congenital disease, occurs in 7% of patients with L/GCMN, and is characterized by proliferation of nevomelanocytes in the leptomeninges and brain parenchyma [6,7]. Neurocutaneous melanocytosis is also frequently associated with Dandy-Walker malformation and a tethered spinal cord [8]. Although NCM may have a benign behavior, symptomatic NCM usually progresses locally with nevus cell proliferation within the meninges and/or brain, and may even metastasize portending a poor prognosis [7].
Congenital melanocytic nevi have somatic mutations in either NRAS codon Q61 or BRAF codon V600 [9–11], and patients with L/GCMN and NCM exhibit a high frequency of NRAS mutations [11–14]. According to Kinsler and colleagues, the same Q61 NRAS mutation is present in central nervous system (CNS) and affected skin lesions, and patients with multiple cutaneous lesions harbor the same mutation in each lesion, but not in nonlesional skin [13]. On the other hand, BRAF mutations have a higher prevalence in small and medium-size CMN [12], and have been considered to be associated with a more benign clinical phenotype [15,16].
NRAS is a well-characterized oncogene involved in controlling key cell signaling pathways [17,18]. Codon 61, at the guanosine triphosphate–binding site, is crucial for its normal inactivation, and mutations at this site lead to constitutively activate NRAS's guanosine triphosphatase function. Active NRAS acts as a molecular switch controlling signaling of phosphatidylinositol 3-kinase and RAF, and then the activation of the Akt and RAF/MEK/ERK pathways, respectively [19]. BRAF gene encodes a serine/threonine kinase that acts by transducing growth signals from Ras to Mek1/2 [20].
Previously published studies focusing on the association between molecular abnormalities and pathological or clinical phenotype in patients with CMN have certain limitations and deserve to be expanded upon. For example, most of these previous studies were retrospective and lack a corresponding broad clinical evaluation, nevi categorization typically used only the size of the main nevus, and no consideration has been given to the presence of NCM [12]. Kinsler and colleagues [13] did perform a detailed analysis, but the study included a small number of patients and the authors did not search for BRAF mutations.
Our aim was to investigate the association between standardized clinical features in a large number of patients with CMN and L/GCMN, in whom nevus tissue was prospectively collected, with their mutational status of NRAS Q61 and BRAF V600. We also strove to find a possible therapeutic target based on mutational status.
METHODS
Study approval
This prospective study was approved by the University of Pittsburgh Institutional Review Board (#PRO10030357) and is in compliance with the Declaration of Helsinki Principles. The patients' parents or guardians provided written informed consent before participation.
Samples
Clinical data and biospecimens were prospectively collected following a standardized protocol as part of “The Gavin Bailey Tissue Repository for Neural Crest Disorders,” housed at the John D. Rangos Research Center, Children's Hospital of Pittsburgh. Fresh samples were received in RPMI culture medium, from which a portion was frozen at −80° C, a 2nd fragment was fixed in formalin, and another fragment was prepared for tissue culture (data not shown). The tissue fixed in formalin was processed according to the routing histological methodology, paraffin embedded, and sectioned for histological analysis. Hematoxylin and eosin–stained slides were reviewed by a senior pathologist (M.R.M.) to confirm the diagnosis of CMN. Exclusion criteria consisted of inadequate or nonrepresentative samples, or when other types of nevi were diagnosed.
Categorization of cutaneous features and NCM diagnosis
Clinical categorization of the cutaneous features of CMN was performed using recommendations described and validated by Krengel and colleagues [21]. This was done blindly, without knowledge of the presence of NCM or the mutational status of each patient. The following characteristics were evaluated: Projected adult size of CMN: Medium: 1.5–20 cm; Large: 20–40 cm; Giant: more than 40 cm; Multiple medium CMN: ≥3 medium CMN without a single, predominant CMN. CMN location: head, trunk, and extremities. Number of satellite nevi: S0: none; S1: 1–20; S2: 20 to 50; S3 >50; Color heterogeneity: C0, none; C1, moderate; C2, marked. Surface rugosity: R0, none; R1, moderate; R2, marked. Dermal or subcutaneous nodules: N0, none; N1, scattered; N2, extensive. Hairiness: H0, none; H1, notable; H2, marked hypertrichosis.
Diagnostic criteria for NCM were redefined by Kadonaga and Frieden [22] in 1991 as follows: (1) large or multiple congenital nevi in association with meningeal melanosis or melanoma, (2) no evidence of cutaneous melanoma except in patients in whom the examined areas of the meningeal lesions are histologically benign, and (3) no evidence of meningeal melanoma except in patients in whom the examined areas of the cutaneous lesions are histologically benign. Strict adherence to these criteria for definitive diagnosis of NCM requires histological confirmation of leptomeningeal melanocytic deposits. However, a provisional diagnosis can be established in patients using magnetic resonance imaging (MRI) [7]. In the 1st 4–6 months of life, MRI is the modality of choice for evaluation of NCM; the neuroradiological appearance of melanocytic deposits consists of T1 hyperintensity and/or T2 hypointensity, most commonly overlying the temporal structures, cerebellum, and leptomeninges [7,23,24].
The diagnosis of NCM in our study was established using MRI performed in the 1st year of life or by pathological review of melanocytic lesions from the CNS and skin. Patients with NCM had either leptomeningeal deposits featuring characteristic signal for melanin in a discrete or diffuse pattern, or pathological review of melanocytic lesion from the CNS and skin. Patients without NCM had no neurological symptoms and a normal MRI.
DNA extraction and genotyping
DNA was extracted from frozen nevus and/or brain/meningeal tissue using the Qiagen QiaAmp DNA Mini Kit (Valencia, CA, USA) following the manufacturer's instructions. Excess fat was trimmed from lesional nevus tissue, and a sample of approximately 30 mg of lesional tissue from the papillary dermis was used for extraction. Brain/meningeal tissues were selected from highly cellular areas with nevomelanocytes, and a sample of approximately 30 mg of tissue was used for DNA extraction. This procedure yielded about 1.8–3 μg of DNA per sample. For blood, the Qiagen QiaAmp Blood Mini Kit (Valencia) was used and genomic DNA was extracted following the protocol provided in the kit. A 200-μL aliquot of whole blood was used from each sample, yielding 3–8 μg of DNA per sample. For formalin-fixed, paraffin-embedded (FFPE) tissue sections, the Qiagen QiaAmp DNA FFPE Tissue Kit (Valencia) was used for genomic DNA extraction according to the kit protocol. Four to five 10-μm freshly cut sections with a surface area up to 250 mm2 for each sample of FFPE lesional tissue were used; the DNA yield was approximately 0.8–1.4 μg per sample.
NRAS Q61 and BRAF V600 mutation analysis
For Sanger sequencing, polymerase chain reaction (PCR) products were sequenced in both sense and antisense directions using the BigDye Terminator v3.1 cycle sequencing kit on ABI 3130 (Applied Biosystems, Inc, Foster City, CA, USA) according to the manufacturer's instructions. The sequences were analyzed using Mutation Surveyor software (SoftGenetics, LLC, State College, PA, USA).
Because NRAS and BRAF mutations are known to be mutually exclusive in CMN, only samples negative for NRAS Q61 mutations were analyzed for BRAF V600E using PCR.
BRAF c.1799T>A mutations, including V600E and V600K, were detected using PCR mutation-specific primers by amplification refractory mutation system (ARMS), according to the procedure of Ellison and colleagues [25]. Approximately 200 ng of genomic DNA extracted from frozen tissues/blood/FFPE tissues was used as template per reaction, and PCR products were subject to electrophoresis on 1% agarose gel for evaluation of positive amplification. Appropriate positive and negative controls were run for each PCR.
Using given amounts of mutated DNA as standards, the mutation detection sensitivity for each of the applied sequencing techniques for the BRAF and NRAS mutations is as follows: NRAS exon 2 and 3 screening by Sanger, 15% of alleles; and by ARMS for BRAF 1799T>A, 1% of alleles.
Statistical analysis
Statistical analysis was performed using SPSS 21.0 (SPSS, Chicago, IL, USA). The results were expressed as mean ± SD or total number and percentage. One-way analyses of variance were used to compare age, nevus size, and number of nevi between 3 groups (NRAS-mutated, BRAF-mutated, and negative for both mutations) and Student t-test for independent samples to compare between 2 groups (NRAS- and BRAF-mutated cases). Chi-square or Fisher's exact test was used to study association between mutational status or NCM diagnosis and nevus clinical categorization. The significance level was set as P ≤ 0.05.
RESULTS
Sample characteristics, NRAS Q61 and BRAF V600 mutation analysis
We studied a total of 66 patients, 8 with medium, 21 with large, and 36 with giant CMN. For one patient we had only a melanocytic lesion from the brain and no clinical data. At the time of initial surgery, the patient age ranged from 6 months to 18 years, with 51 patients (78.5%) younger than 3 years of age. Forty (60.6%) were female and 26 (30.4%) were male. There were 48 Caucasians (72.7%) and 15 Asians (22.7%), and information about race was not available for 3 patients. The main nevus size ranged from 6 to 80 cm (mean 31.5 cm) and satellite nevi ranged from 0 to 300 (mean 58.9).
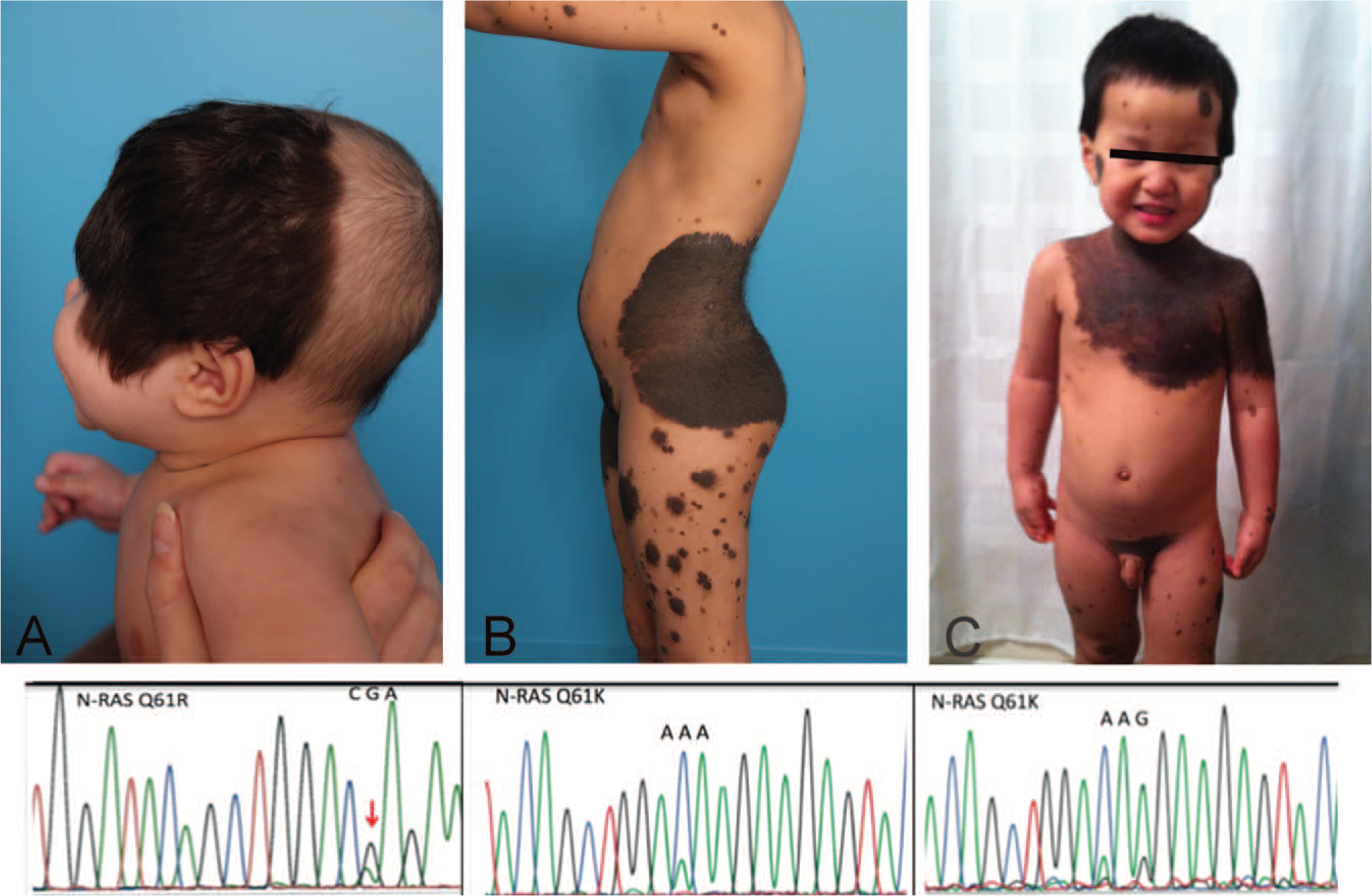
NRAS mutations were detected in 51 (77.3%) and BRAF mutations in 5 cases (7.6%). Ten cases (15.2%) were negative for both mutations. NRAS mutation types were NRAS p.Q61R, c.182A>G in 14 cases and NRAS p.Q61K, c.181C>A in 34 cases; 3 other cases had 2 nucleotide substitutions at codon 61 (c.181C>A, and c.183A->G) resulting in p. Q61K amino acid change (Fig. 1).
One patient with NRAS Q61K carrying 2 nucleotide substitutions (Q61K c.181C>A and c.183A>G) had symptomatic NCM, whereas the other one had a giant CMN, a nonmelanocytic tumor (mouth choristoma), and history of melanoma in a grandmother.
Five patients whose melanocytic lesions were positive for NRAS Q61 mutation and 2 patients with melanocytic lesions positive for BRAF V600E mutation were negative for the same mutation in DNA extracted from peripheral blood.
Association of NRAS and BRAF mutations with clinical features and nevus categorization
Table 1 shows the association between clinical features and nevus characteristics with NRAS/BRAF mutational status. NRAS Q61 mutations were found in 5 (62.2%) of 8 medium, 15 (76.2%) of 21 large, and 29 (80.6%) of 36 giant CMN (P = 0.698). BRAF mutations were identified in 1 (4.8%) of 21 large and 4 (11.1%) of 36 giant CMN. There were no BRAF mutations found in medium CMN.
Association of NRAS and BRAF mutations with clinical features and nevus categorization (n = 66) a
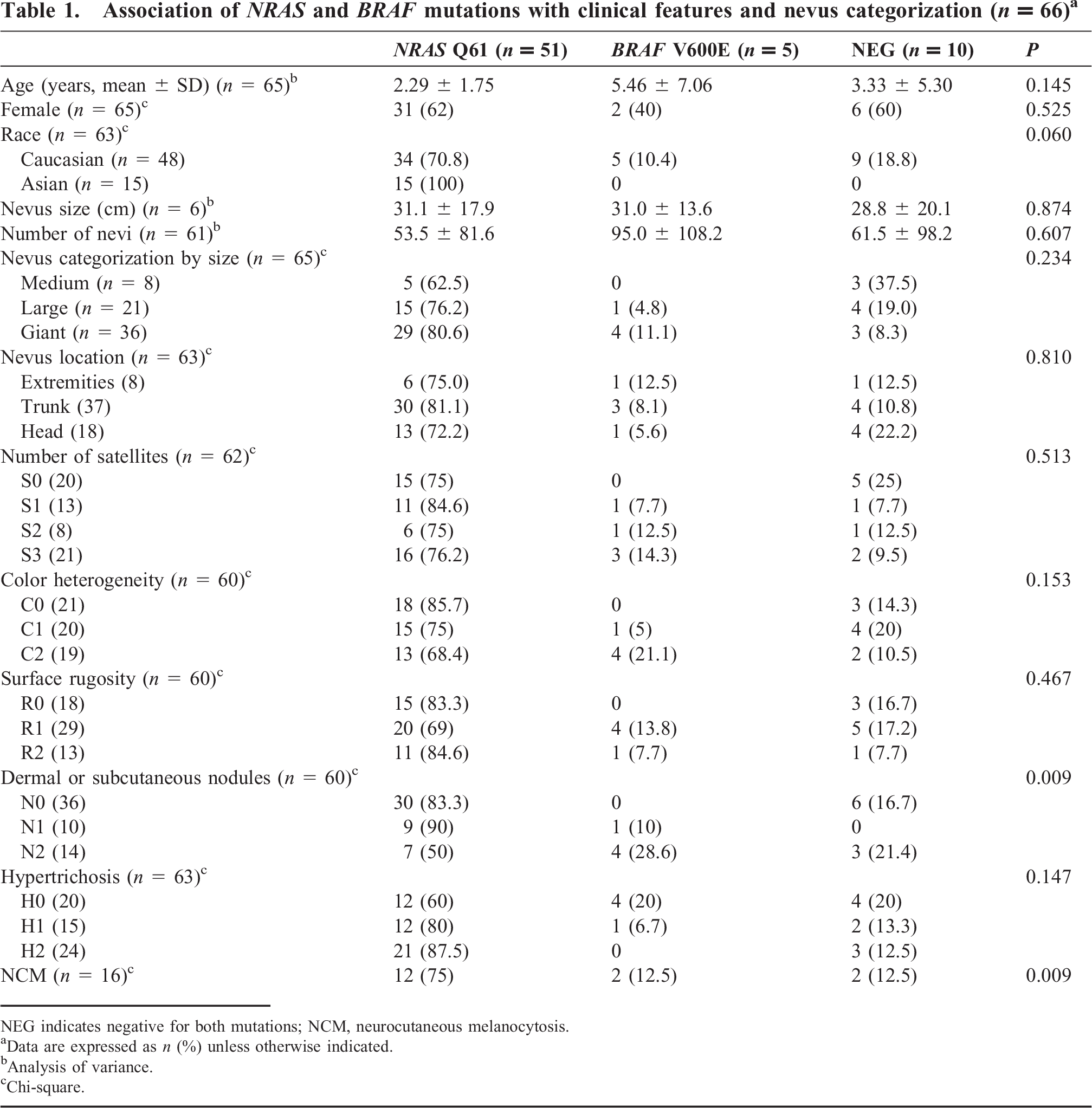
NEG indicates negative for both mutations; NCM, neurocutaneous melanocytosis.
Data are expressed as n (%) unless otherwise indicated.
Analysis of variance.
Chi-square.
All 5 nevi with BRAF mutations showed dermal/subcutaneous nodules (Figs. 2,3) compared with only 32% of NRAS-mutated nevi (P = 0.002). Fifty percent of nevi with dermal/subcutaneous nodules had NRAS mutations, and a BRAF mutation was identified in 28.6% (Table 1). Hypertrichosis was more prevalent in NRAS- (Fig. 1) than in BRAF-mutated nevi (Fig. 2, Right; P = 0.041). There is no statistically significant difference between NRAS and BRAF mutational status in regard to nevus size, number, location, color heterogeneity, or surface rugosity.
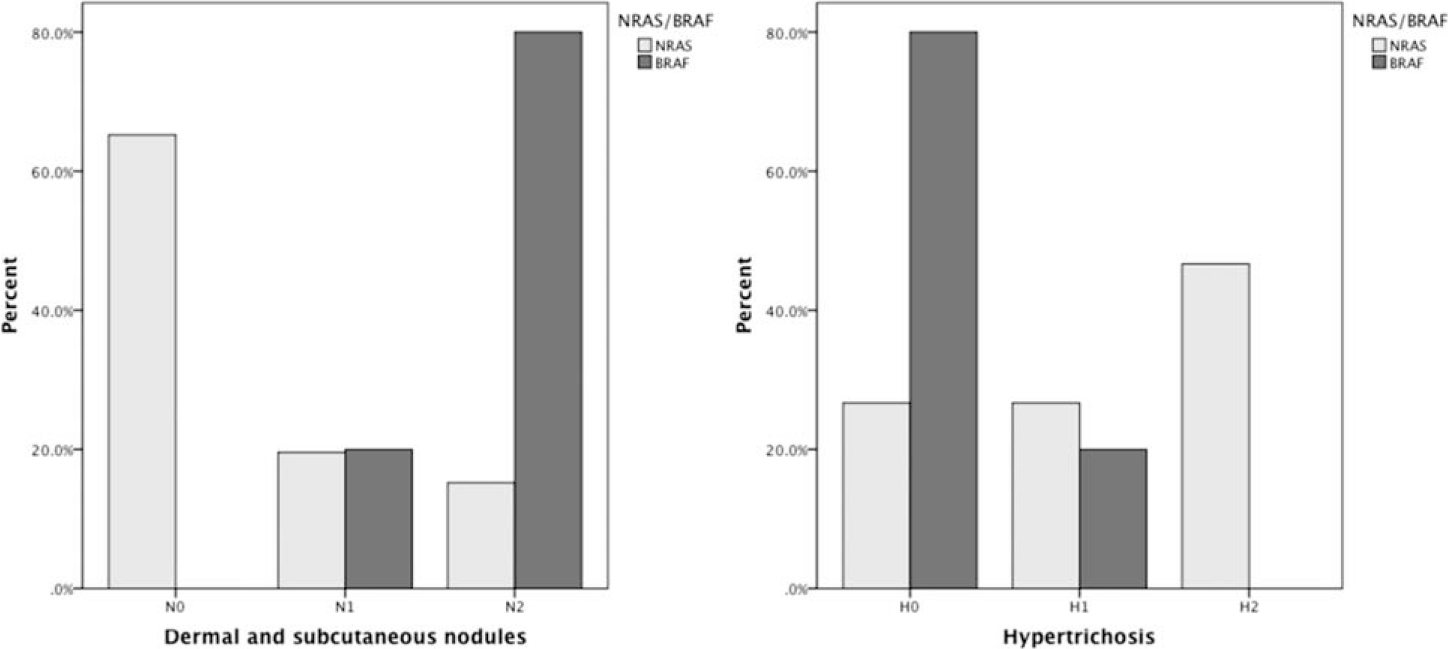
Left: percentage of patients with no (N0), scattered (N1) or extensive (N2) dermal and subcutaneous nodules by NRAS or BRAF mutation. Chi-square test; P = 0.002. Right: percentage of patients with no (H0), notable (H1) or marked (H2) hypertrichosis by NRAS or BRAF mutation. Chi-square test; P = 0.041.

All 5 patients with BRAF V600E mutation showing scattered/extensive dermal or subcutaneous nodules within their large/giant congenital melanocytic nevi.
Association of NRAS/BRAF mutational status, clinical features, and nevus categorization with NCM
Forty-four patients were evaluated with MRI in their 1st year of life and 16 of the 44 were diagnosed with NCM. NRAS Q61 mutations (K or R) were detected in 12 (75.5%) of these 16, and 2 (12.5%) of 16 showed BRAF V600E mutation (P = 0.009). Two patients were negative for both mutations.
Clinical features, nevus categorization, NRAS and BRAF mutational status of patients with and without NCM are shown in Table 2. There is no association between mutational status and NCM diagnosis (P = 0.499). Patients with NCM, compared to patients without NCM, had increased nevus rugosity and more satellites. However, hypertrichosis is less prevalent in patients with NCM (Table 2).
Clinical characterization and NRAS/BRAF mutations status of patients with magnetic resonance imaging with and without neurocutaneous melanocytosis (NCM) (n = 44) a
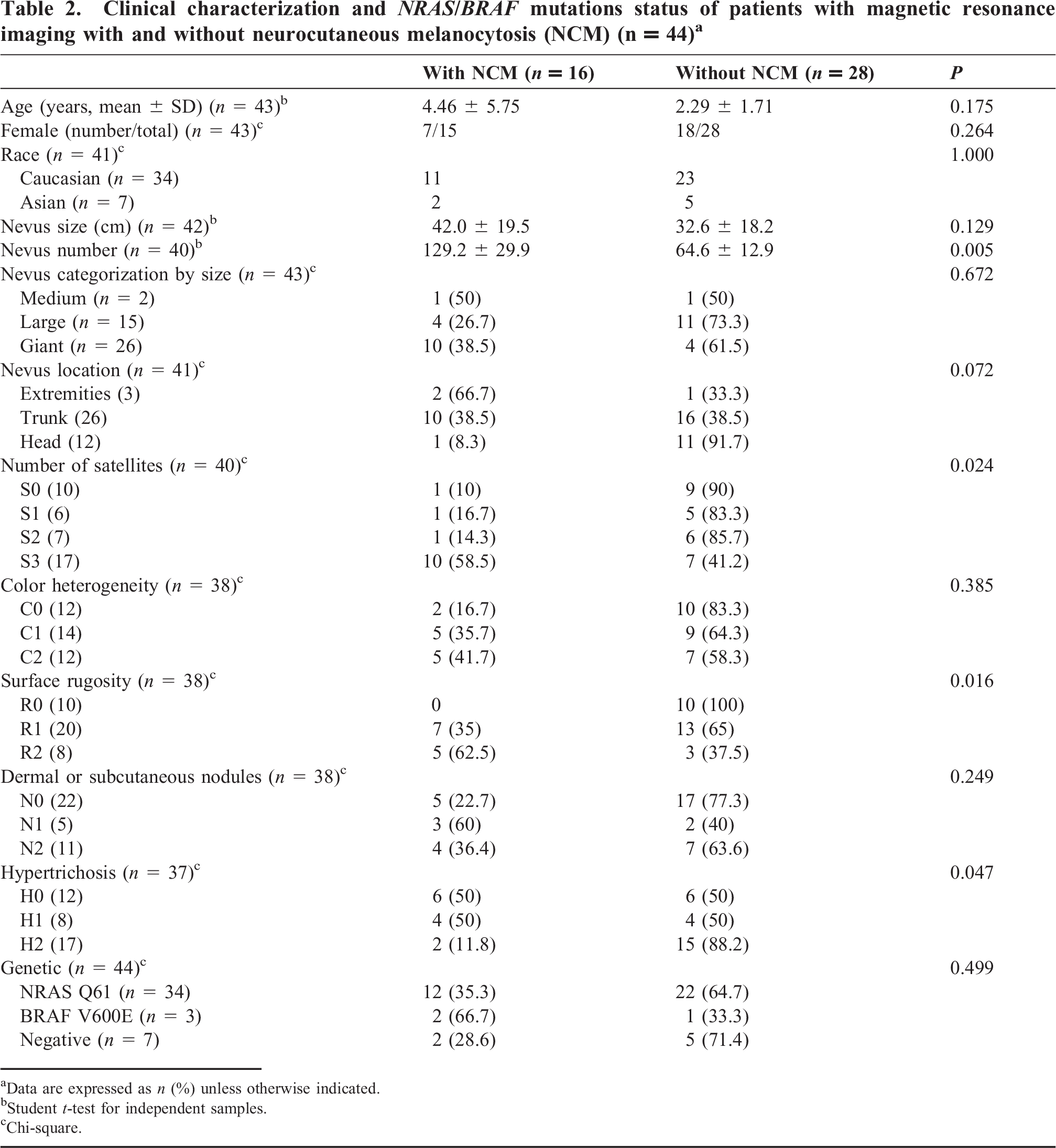
Data are expressed as n (%) unless otherwise indicated.
Student t-test for independent samples.
Chi-square.
DISCUSSION
Our results, based on a prospective study of a large sample of patients, show that BRAF mutations are associated with L/GCMN as well as NCM. Our findings agreed with a recently published study showing that mutations in codon 61 of NRAS are highly prevalent in L/GCMN [12] and NCM patients [13]. However, to the best of our knowledge, BRAF V600E mutations have not been previously documented in patients with NCM. Recently, Muñoz-Hidalgo and colleagues [26] reported a case with 2 meningeal melanocytomas carrying BRAF V600E mutation, associated with PTEN and NF2 deletions. Nevertheless, their patient did not fulfill diagnostic criteria of NCM, showing only a nevus of Ota associated with ipsilateral melanocytomas (benign tumors). Schäfer and colleagues [27] also reported a 47-year-old patient with multifocal brain melanomas, apparently metastatic, and BRAF V600E mutation. Treatment with vemurafenib was followed by complete resolution of the leptomeningeal melanomatosis [27]. Although neither of the 2 above-mentioned reports includes patients with bona fide NCM, our findings support the notion that BRAF V600E–mutated NCM patients may benefit from targeting this signaling pathway. We also present further evidence that BRAF mutations are also associated with nevomelanocytic proliferations involving the CNS.
Gerami and Paller [16] have hypothesized that the ability of NRAS mutations to stimulate 2 different pathways concurrently, namely ERK and PI3K/AKT, confers a more ominous character to NRAS-mutated lesions. This is in contrast to activation of only the ERK signaling pathway by activated BRAF. We may accept this notion as a theoretical explanation, although our findings show that BRAF mutations are also associated with an aggressive nevomelanocytic proliferation in children with L/GCMN.
The role played by mutations or polymorphisms in other genes also deserves attention. Kinsler and colleagues [28] have shown that the germline MC1R genotype modifies the growth (expressed as size and multiplicity) of CMN. It would be interesting to investigate whether MC1R variations could modify the expression of the NRAS/BRAF mutation, leading to increased proliferation of nevomelanocytes and NCM. Our extensive genetic analysis has accumulated data that support a possible role for other polymorphisms influencing the NRAS phenotype (unpublished results).
The patients' racial background seems to also contribute to variations among NRAS and BRAF mutations. All Asian patients in our study showed NRAS Q61 mutations, in keeping with the reported absence of BRAF V600E mutations in GCMN in a Chinese population [11].
In contrast with the reported higher prevalence of BRAF mutation in medium-size CMN [10,12], we did not find statistically significant differences between medium-size CMN and L/GCMN regarding BRAF/NRAS mutational status. These seemingly discrepant results could be explained by our use of the system of Krengel and colleagues [21], a more objective and reproducible approach to assess nevus size, and by the relatively larger medium-size CMN (all have projected adult size >10 cm, M2 by the system of Krengel and colleagues) and our small number of medium-size CMN (only 8 cases in our sample).
Another surprising and novel observation in our study was the significant association between scattered/extensive dermal/subcutaneous nodules and BRAF mutations. Although NRAS- and BRAF-mutated nevi share many clinical characteristics, this genotype/phenotype difference is puzzling. No clear explanation is available. However, this could be related to the mechanism by which oncogene-induced senescence occurs in nevus cells of these 2 genotypes. Although BRAF V600E mutation is known to contribute to the initial steps of melanomagenesis, it is also known to induce a senescence-like cell cycle arrest [20], supporting the notion of a model where BRAF V600E mutation is not frequently sufficient to fully induce nevus cells into a more aggressive phenotype, probably requiring additional mutations or polymorphisms to achieve this effect. In contrast, NRAS Q61 may be capable of initiating melanomagenesis and lead to escape of oncogene-induced senescence, possibly by interactions with more than 1 signaling pathway [16]. It is possible that BRAF mutation generates a more vigorous proliferation response before senescence pathways are activated, and therefore leads to a robust cell cycle arrest. Mutated NRAS, on the other hand, probably triggers a more sustained proliferation, which is extensive but less vigorous than BRAF's. More studies are required to prove this contention. However, given our 5 patients with scattered/extensive dermal/subcutaneous nodularity, 2 of whom also have NCM, this mutation cannot be longer considered a less aggressive genetic change, but only a less frequent one. Furthermore, our findings prove that NRAS mutations cannot be considered exclusive of L/GCMN and NCM. The possibility of finding additional gene mutations/polymorphisms contributing to phenotypes in the spectrum of L/GCMN and NCM remains open and in need of investigation.
An additional and puzzling phenotypic difference observed between BRAF- and NRAS-mutated nevi is the degree of nevus hairiness: NRAS-mutated nevi featured more hypertrichosis, again suggesting a difference in the molecular pathways affected by NRAS and BRAF mutations.
In regard to NCM, a subgroup of our patients had undergone MRI examination, and we compared differences between patients with and without NCM. In keeping with findings reported by Marghoob and colleagues [29], increased numbers of satellites were associated with MRI evidence of NCM in our patients. In addition, we documented increased nevus rugosity and decreased hairiness associated with NCM. This associative analysis was possible only by using Krengel and colleagues' standardized evaluation [21], whose expert consensus-based recommendations lead to a reproducible methodology, making our results comparable with those of potential future studies.
Potential limitations to our studies include variations in sensitivity of detecting DNA mutations by Sanger analysis or other methodologies, because cases found negative for NRAS and BRAF mutations could carry NRAS-mutated DNA below the level of Sanger sequencing detection. In addition, these cases could have mutations in others genes less obviously related to melanocytic differentiation and proliferation, an area in which we are currently working. However, because our genetic associative studies used only cases with confirmed NRAS or BRAF mutations, these limitations do not compromise our conclusions.
Several conclusions can be reached. First and most important is the demonstration of BRAF V600E mutation, instead of NRAS Q61, in some patients with NCM, which has not been previously reported. Second, BRAF V600E somatic mosaicism is definitely also associated with L/GCMN. Therefore, NRAS mutations should not be considered exclusive of L/GCMN or NCM, and BRAF mutations cannot be taken as responsible for a more benign disease. Our findings also open the possibility to target BRAF in the therapeutic approach for some patients with NCM and L/GCMN. Another novel finding is that nevi with BRAF V600E mutation had more dermal/subcutaneous nodules and less hypertrichosis than those with NRAS Q61 mutation. Finally, our findings agree with the reported lack of BRAF V600E mutation in Asians, underscoring the role that racial background plays in segregating mutational groups.
Recent studies have suggested that BRAF mutations occurring predominantly in small and medium-size nevi lead to a more benign type of nevus-associated disease. Our prospective analysis reveals, for the 1st time, that BRAF mutations are also associated with aggressive disease, including NCM and L/GCMN with prominent and scattered/extensive nodularity. These findings open the possibility for therapy using BRAF inhibitors in some NCM patients.