
Abstract
Deposition of the complement split product C4d is a phenomenon studied extensively as a marker for complement activation in antibody-mediated transplant rejection. C4d also is observed in placental disease processes including spontaneous abortion, infarct, and villitis of unknown origins. Massive chronic intervillositis is a rare placental abnormality associated with increased risk of growth restriction, fetal death, and recurrent fetal loss. In this study, we evaluated C4d immunostaining in placentas with accumulation of intervillous monocytes with and without villitis. Archived placentas from Kosair Children's Hospital (Louisville, KY) and Seattle Children's Hospital (Seattle, WA) were selected and divided into 4 groups, 16 cases of intervillositis with complicated pregnancy, 15 cases of uncomplicated intervillositis, 20 cases of complicated villitis, and 13 cases of uncomplicated villitis, all with varying degrees of monocytic cells in the intervillous space. Representative specimen blocks were immunohistochemically stained for C4d. The percentage of positive staining of the microvillous surface of the syncytiotrophoblast was scored by five pathologists, and the following consensus score was determined: 0 = 0% to 5%; 1 = 5% to 25%; 2 = 25% to 75%; and 3 ≥ 75%. C4d immunostain localized to the microvillous border of syncytiotrophoblast in many of the placentas. C4d staining was more strongly associated with intervillositis than with villitis (odds ratio: 6.3; confidence interval: 2.1–18.7; P = 0.001).
INTRODUCTION
C4d is the stable product of classic complement activation that can be detected in tissue by immunohistochemistry and is routinely used to evaluate humoral immunity in human allograft transplantation. Chronic massive intervillositis is a pathological lesion of the placenta characterized by massive numbers of monocytes in the intervillous space, that has been associated with fetal death, intrauterine growth retardation, and recurrence in subsequent pregnancies [1–6]. Smaller numbers of intervillous monocytes may be observed in the placenta and are of unknown clinical significance. Variable intensity of intervillous monocytes is associated with lymphohistiocytic villitis [7]. One of the present authors (E.R.), in a study of C4d staining of placentas with villitis, noted the intense staining of the syncytiotrophoblast in a placenta with massive chronic intervillositis [8]. Because the placenta can express paternal alloantigens on the syncytiotrophoblast surface, although not allogeneic histocompatibility antigens, a reasonable hypothesis is that massive chronic intervillositis is evidence of complement activation due to antibodies to paternal antigens on the syncytiotrophoblast microvillous surface [9,10]. Independent evidence suggests that complement activation produces cytokines that result in increased monocyte adherence to syncytiotrophoblast [11]. As a first step in testing this hypothesis, we immunohistochemically stained placentas with intervillous monocytes for C4d.
METHODS
This study was conducted at Seattle Children's Hospital, Seattle, WA, and Kosair Children's Hospital, Louisville, KY, with approval of both of the institutional review boards.
At Kosair Children's Hospital, placentas from multiple hospitals in the city were examined, and the results were entered into a CoPath database (Cerner, Kansas City, MO, USA). This database was searched both in the diagnosis and microscopic description fields for the term “intervillositis.” All cases with any degree of intervillositis but without villitis were included. Cases with villitis with intervillositis were too numerous to include all cases; therefore, 8 cases of complicated pregnancies and 11 cases of uncomplicated pregnancies with this diagnosis were included. In addition, a separate autopsy database was searched for perinatal deaths attributed to villitis to add three cases with complicated outcome. At Seattle Children's Hospital, the search terms “intervillositis” and “chronic villitis” were queried in the pathology database, yielding 14 cases. A representative slide of the placental parenchyma was selected from each case for C4d staining of that tissue block using a rabbit polyclonal antibody to C4d and processed on a Benchmark Ultra stainer (Ventana Medical Systems, Tucson, AZ, USA). Each institution stained that institution's slides with their routine antigen retrieval protocols.
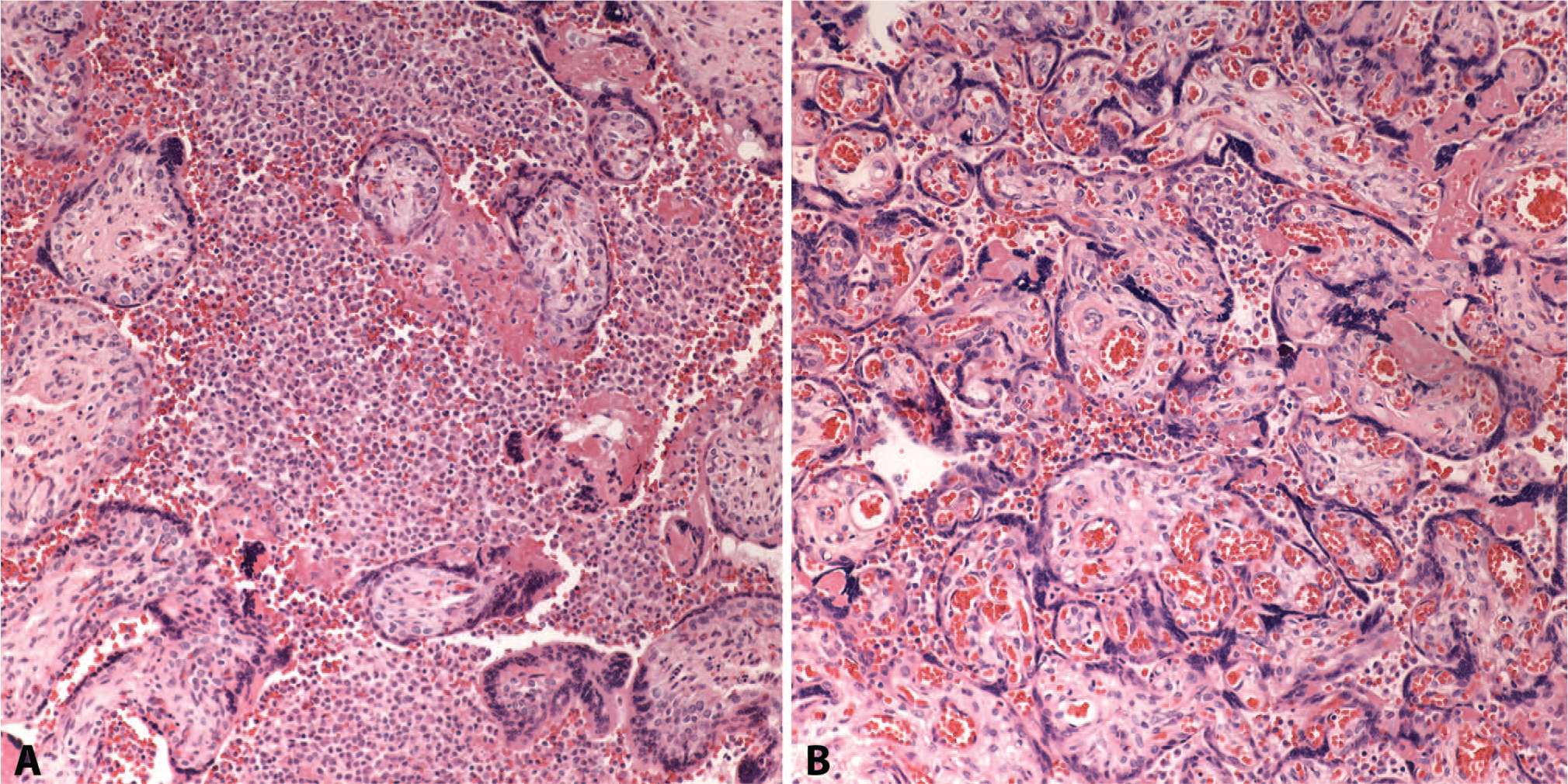
C4d-stained slides from both institutions were scored independently by five pathologists without knowledge of the clinical history or the reported placental histology diagnosis. Staining of the syncytiotrophoblast surface was given a score based on the following scheme: 0 = 0% to 5%; 1 = 5% to 25%; 2 = 25% to 75%; and 3 = ≥75%, with percentage referring to the proportion of positive villi. For analysis, consensus scores were achieved by grouping individual scores into four categories. For all consensus categories, individual scores reached agreement within a category range of one score difference. Final consensus scores were defined as “0” if all individual scores were 0; “1” if all scores were 0 or 1, “2” if all scores were 1 or 2; and “3” if all scores were 2 or 3. Cases were grouped into histological categories based on the original diagnosis: massive chronic intervillositis (MCI), few intervillous monocytes (FIM) (which was designated in the original pathology reports as intervillositis but with comments that the monocytes were less intense than those in MCI), and villitis with intervillous monocytes (VIM) (Fig. 1). Outcomes were divided into those that were complicated (perinatal death or intrauterine growth retardation) or uncomplicated. Cases were also reviewed for information on maternal gravidity and parity and for recurrence in the same mother.

Scores of the staining were used to look for correlations with histology and outcome by using proportional odds logistic regression, with staining as the four-level endpoint. The model was adjusted for institution.
RESULTS
Table 1 presents data on each reviewed case. The C4d staining classification demonstrated a correlation between C4d staining and any chronic intervillositis without villitis compared to with villitis (odds ratio: 6.3; 95% confidence interval [CI]: 2.1–18.7; P = 0.001). Table 1 also documents the fact that five mothers had recurrent MCI (and these cases are reviewed below in detail). Six cases had only focal MCI (Fig. 2), that is, the histological picture in regions of the placenta showed massive numbers of intervillous monocytes that were absent in other areas. These cases were categorized as MCI. The mean gestation for MCI was 30.2 weeks, 34 weeks for FIM, and 35.5 weeks for villitis of unknown etiology (VUE). Table 2 compares four categories: A = those with intervillositis without complications; B = those with intervillositis with complications (stillbirth or growth restriction); C = those with villitis or intervillositis without complications; and D = those with villitis or intervillositis with complications. Patients were grouped by outcomes 0 to 1+ and 2 to 3+. There were no significant differences. Using the same grouping of staining outcome, Table 1 shows there are 12 MCI compared to 2 FIM for staining 1 to 0 and 12 FIM to 5 MCI.
Case data
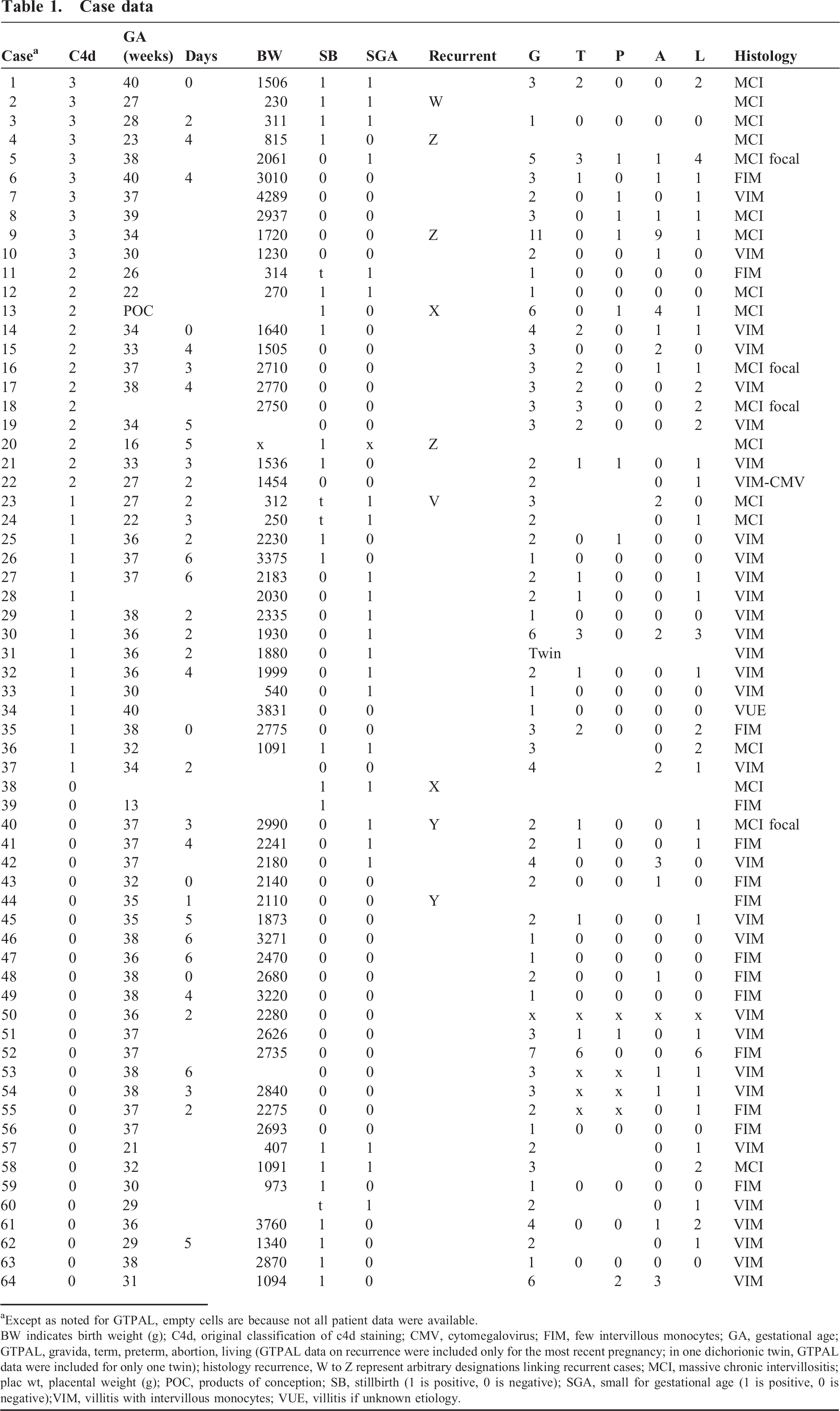
Except as noted for GTPAL, empty cells are because not all patient data were available.
BW indicates birth weight (g); C4d, original classification of c4d staining; CMV, cytomegalovirus; FIM, few intervillous monocytes; GA, gestational age; GTPAL, gravida, term, preterm, abortion, living (GTPAL data on recurrence were included only for the most recent pregnancy; in one dichorionic twin, GTPAL data were included for only one twin); histology recurrence, W to Z represent arbitrary designations linking recurrent cases; MCI, massive chronic intervillositis; plac wt, placental weight (g); POC, products of conception; SB, stillbirth (1 is positive, 0 is negative); SGA, small for gestational age (1 is positive, 0 is negative);VIM, villitis with intervillous monocytes; VUE, villitis if unknown etiology.
Comparison of staining by clinical/histological group
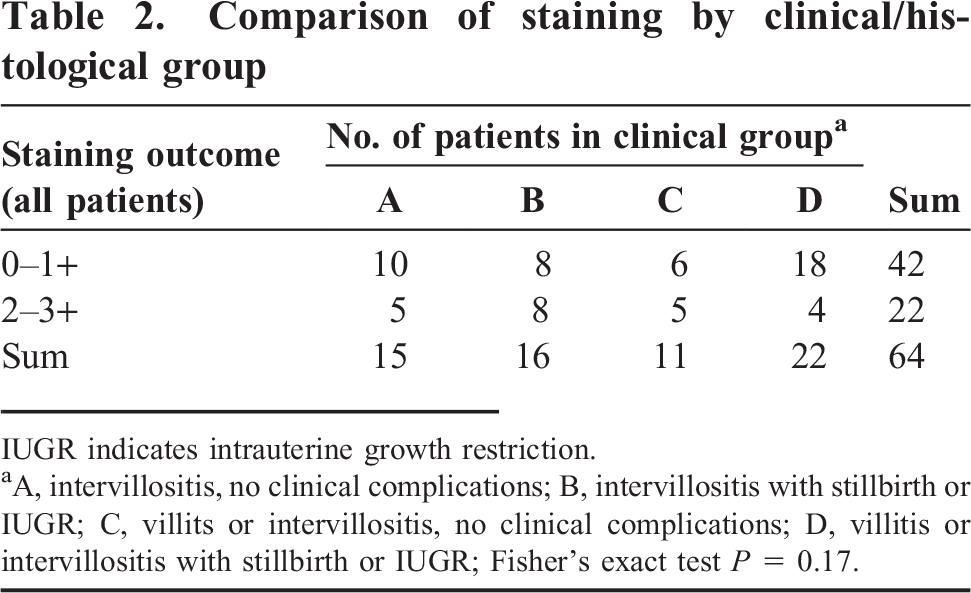
IUGR indicates intrauterine growth restriction.
A, intervillositis, no clinical complications; B, intervillositis with stillbirth or IUGR; C, villits or intervillositis, no clinical complications; D, villitis or intervillositis with stillbirth or IUGR; Fisher's exact test P — 0.17.
Presentation of patients with recurrence
Mother Z
This was the case of a gravida (G) 11 mother who had 1 successful pregnancy followed by 9 losses, which included placentas 4 and 20. Placenta 9 in our series was from her last pregnancy (successful although preterm at 34 weeks of gestation). This placenta had visually less intense C4d staining and fewer intervillous monocytes than her two previous pregnancies (Fig. 3). This pregnancy had been treated with prednisone.
Mother Y
This mother had an index placenta with FIM, but her second delivery had more intense focal accumulation of monocytes. Neither of the placentas had C4d staining, and both of the pregnancies were uncomplicated.
Mother X
This G6 mother with 4 losses had 1 preterm delivery of a living infant. The index fetal loss case from an outside institution was reviewed at our institution and diagnosed as placental MCI; however, because we did not have tissue blocks to stain, we could not include this case in the present study. We were able to find two earlier curettages of first trimester fetal losses that demonstrated MCI and positive C4d staining.
Mother W
This patient had two first trimester fetal losses in our files, with the diagnosis of MCI. The tissue blocks could found only for one of those cases; the placenta did demonstrate MCI and C4d staining.
Mother V
This G3 mother had two prior pregnancy losses before undergoing a therapeutic termination of her third pregnancy secondary to severe intrauterine growth restriction and oligohydramnios. Examination of the placenta for the third fetus showed diffuse chronic histiocytic intervillositis with weak C4d staining. The placenta for the index fetal loss case was requested from an outside institution for review and was subsequently diagnosed with placental MCI. However, because we did have access to tissue blocks for this case, we could not include the index case in the present study.
DISCUSSION
After consensus was reached among the pathologists for classification of the C4d staining, the study analysis found a significant association between extensive C4d immunolocalization and placentas showing only intervillous monocytes compared to those with villitis. Separate from the statistical significance is the simple observation that those placentas with chronic intervillositis, and particularly those with denser intervillous monocytes, showed immunolocalization of C4d along the microvillous border of the syncytiotrophoblast. The implication of this finding is that complement was being fixed along that border. The severe growth retardation and fetal death often associated with massive chronic intervillositis is likely explained by injury to this critical absorptive microvillous border. Complement fixation might also induce cytokines that would up-regulate monocyte adhesion in the intervillous space. Localization of C4d was relatively diffuse in many cases, consistent with a diffuse antibody in maternal blood fixing to the syncytiotrophoblast. Recurrence of such staining and of intervillous monocytes in subsequent pregnancies suggests that a paternal alloantigen on the microvillous surface could be inducing an allogeneic humoral rejection analogous to Rh blood group. Other studies have also suggested a non-human leukocyte antigen-based alloantigen on Trophoblast to play a role in recurrent fetal loss [10].
There are some limitations to further interpretation of the data. The distinction of few intervillous monocytes from massive chronic intervillositis was arbitrary based on the initial pathology diagnosis, and no specific criteria were established to make this distinction. Thus, there is no analysis of this difference, but there is a clear tendency seen on Table 1 for the cases with fewer monocytes to have less C4d staining and fewer complications. Other studies have graded intervillositis intensity but there is no consensus technique [12–14]. (Cell counts of intervillous monocytes have shown no overlap of normal controls with MCI [15].) The C4d staining was variable as was the density of intravillous monocytes in the cases of VIM. Lymphohistiocytic villitis is considered a maternal T-cell-mediated rejection within villi, but coexisting humoral antibody-mediated injury cannot be excluded. Another limitation of our study was that villous staining for C4d was scored in all villi including those with evidence of injury, either villitis or perivillous fibrinoid, which may be a less specific localization than that on normal appearing villi because such injury could expose antigens not otherwise accessible to intervillous blood.
An unanticipated finding was the existence of focal MCI with corresponding focal C4d staining. This is difficult to account for as an allogeneic rejection, unless there was mosaicism. A focal surface viral response might account for focal complement injury. These cases do show that there was a direct correlation of areas of C4d staining with the monocytes, consistent with the hypothesis that complement injury is triggering local cytokine up-regulation of monocyte cell adhesion.
Proof of an allogeneic paternal trophoblastic antigen would require identification of a complement fixing antibody to the antigen in maternal blood. Nonetheless, based on the C4d evidence, a study of antihumoral rejection treatment of mothers with fetal growth restriction and a prior infant with massive chronic intervillositis is reasonable. Our one case treated with prednisone, occurring with a viable infant, showed decreased C4d staining and decreased intervillous monocytes compared to those in her prior pregnancy losses. Published cases have had mixed results, with treatment of recurrent loss associated with MCI [6]. However, the small numbers, the heterogeneity of pathological definition, and the possibility that some cases are due to a paternal antigen that is heterozygous would be confounding factors. Another possible confounding factor would be maternal heparin therapy, because that may prevent activation of complement [16]. A prospective multi-institutional study would be needed to evaluate therapy and the potential role of maternal complement levels or C4d staining of the placenta in previous pregnancies to predict success.
Mechanisms other than alloimmune rejection could also cause the accumulation of intervillous monocytes and or C4d villous localization. There is evidence that patients with autoimmune disease such as systemic lupus erythematosus may have C4d staining of the placenta [17,18]. A case of neonatal alloimmune thrombocytopenia demonstrated MCI [19]. Possibly an additional antitrophoblast antibody was present in those cases. Malaria is commonly associated with MCI but not with intrauterine growth restriction or stillbirth, and may have a different mechanism than non-malarial MCI [20].
In summary, the C4d staining of syncytiotrophoblast seen in our study supports but does not prove the concept that MCI is the result of allogeneic humoral rejection of the placenta. Small numbers of monocytes in the intervillous space may not be due to the same mechanism and usually lack C4d villous staining and pregnancy complications. The chronic intervillositis associated with VUE may have C4d staining that may or may not be related to humoral rejection. Not all complicated outcomes are necessarily related to the pathological lesions described. Future research will be needed to determine whether complement fixation as measured by lower serum levels is a useful measure of autoimmune villous injury in growth-restricted infants and whether therapy aimed at reducing complement fixation will improve outcome for infants with MCI or Villitis.
CONCLUSIONS
C4d staining is evidence of complement fixation at the microvillous surface of the placenta. This mechanism could interfere with trophoblastic function and result in activation of monocyte adhesion. C4d staining and high risk of recurrence in intervillositis is consistent with allogeneic humoral rejection to a microvillous trophoblastic antigen.