
Abstract
The clinical or forensic pathologic evaluation of an infant with an apparently inflicted head injury can be challenging, particularly when objective findings are limited to the classic triad ascribed to “Shaken Baby Syndrome” – subdural and retinal hemorrhages and anoxic brain injury. These three findings together, in the absence of an apparent impact site (scalp or skull injury) have a controversial differential diagnosis. However, the discovery of an impact site of virtually any size is sufficient for some forensic pathologists to make the diagnosis of homicidal (impact) blunt head trauma in babies with limited additional evidence of abuse, or with the classic triad, but without careful consideration of its differential diagnosis. Although relatively uncommon in modern intensive care units, occipital scalp ulcers can and do occur, and may mimic the appearance of a blunt impact site. Two separate cases of infant death are presented to illustrate the nature and appearance of occipital pressure ulcers. Abnormalities of the occipital scalp were not detected in either infant upon hospital admission, but scalp lesions were clearly observed at autopsy. Macroscopically, these lesions closely resembled blunt impact sites. They were determined to be pressure ulcers based predominantly on the histologic findings of epidermal thinning and dermal homogenization, combined with the absence of both hemorrhage and stainable free iron. Further supportive factors were the absence of skull fractures, intracranial hemorrhages, and cerebrocortical contusions.
Introduction
Pressure ulcers are frequently observed within neonatal and pediatric intensive care units (ICUs). Studies have indicated that up to 27% of pediatric ICU patients develop pressure ulcers (1), with the most common locations being the occipital scalp, the ear, and the nose (2), with localized ischemia being recognized as the causative factor for the development of tissue necrosis (3). Occipital scalp pressure has even been documented as a cause of alopecia following prolonged operative procedures (4). Unlike adults, children (and especially infants) have limited hair growth, and less subcutaneous tissue in the occipital region, increasing their susceptibility to the effects of scalp pressure (5). The vast majority of pediatric ICUs have protocols in place to minimize or prevent pressure ulcers; these protocols are meant to address not only the amount of pressure exerted upon pressure points, such as the bony prominence of the occipital scalp, but also the length of time that pressure is applied (5). Infants hospitalized for a variety of conditions, especially those with severe neurologic illness or trauma, with or without paralysis (therapeutic or otherwise), and those with low systolic blood pressure are particularly vulnerable to occipital pressure ulcers, even with regular turning of the head and/or torso (6–8). Ischemic occipital ulcers (IOUs) may be caused not only by pressure of the head against a pillow, bed or other surface, but also against cervical stabilization collars and other medical devices (6, 9), particularly when cervical collars are in place over a period of several days (10).
Clinicians and forensic pathologists tasked with the assessment of the apparently abused child must be aware that IOUs do occur, albeit uncommonly, and may closely mimic the appearance of impact sites observed in cases of alleged inflicted blunt impact head trauma. The risks associated with misinterpretation of an IOU as an impact site are highest when the clinician / pathologist is faced with the evaluation of an infant with limited evidence of injury, particularly in the circumstance of the classic triad of “shaken baby syndrome” (SBS) – subdural hemorrhage, anoxic brain injury and retinal hemorrhages. Forensic pathologists may forego validation of the triad based on the presence of an impact site. Here we present two cases in which IOUs developed in a pediatric ICU, and closely mimicked occipital impact sites. While neither case had other objectively suspicious features of inflicted trauma, the discovery of apparent impact sites was cause for concern. Careful evaluation including histologic studies facilitated reaching a correct diagnosis.
Case 1
A 3-month-old black male was at home under the care of his biological father when he was observed to have labored breathing while prone in a bassinet. He was lying on top of a thick, furry blanket that had been folded four times. Upon discovery, he allegedly had arched legs, puckered fists and white milk-like mucus on his mouth. He was transferred to hospital and admitted with anoxic brain injury and its complications. Diagnostic imaging revealed brain swelling without intracranial hemorrhage. “Retinal hemorrhages” were detected via direct fundoscopy. He was admitted to hospital intubated, and over the course of three days was determined to be brain dead. His family consented to harvesting of his thoracoabdominal viscera for transplantation purposes, which occurred four days later. While in hospital, he was reportedly turned as per hospital nursing protocol, once per hour. Careful review of the scene, thorough autopsy and review of the medical records did not refute the circumstances of death. Interviews with the hospital staff revealed that scalp “injuries” were not observed at the initial admission, and scalp ulcer development during hospitalization was adamantly denied. A cervical stabilization collar was in place for several days of the hospitalization.
At autopsy three red-brown ‘abraded’ lesions were located in the midline occipital scalp and were up to 6 x 3.5 centimeter (Image 1). The subjacent subcuticular soft tissues were markedly congested (Image 2). Classic end-stage anoxic features were present, without intracranial hemorrhages. Evaluation of the en bloc cervical spine resection specimen did not reveal trauma. Dissection of the enucleated eyes revealed only punctate posterior pole hemorrhages. Histology of the scalp lesion (Images 3 and 4) demonstrated marked ischemia with thinning and necrosis of the epidermis, early thinning and homogenization of the dermal collagen, subtle vascular congestion and an absence of extravasated erythrocytes and stainable iron. The death was certified as an accidental suffocation.

(Case 1): Occipital scalp ulcers following shaving of the scalp hair. The lowermost two lesions were felt most likely to be associated with ICU monitoring lines that passed under the infant's neck and occipital scalp while hospitalized prior to organ and tissue procurement.

(Case 1): Occipital skull following reflection of the scalp. The subcutaneous soft tissue immediately underlying the cutaneous ulcer have marked vascular congestion. Patchy galeal ecchymoses near lambda are associated with profound sutural diastasis.
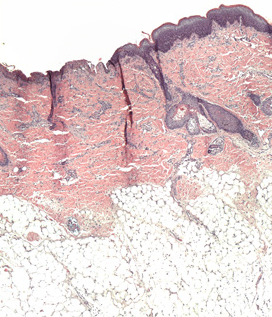
(Case 1): Composite image composed of multiple photomicrographs taken at 10X from a single H&E slide prepared from the occipital scalp. Notice the clear delineation between normal (right) and ischemic (left) skin. The abnormal scalp is characterized by epidermal thinning and dermal homogenization. Erythocyte extravasation and free iron are not within any section of examined skin. Inflammation is not a significant component of the normal or abnormal skin. The subcuticular adipose tissue is essentially normal.
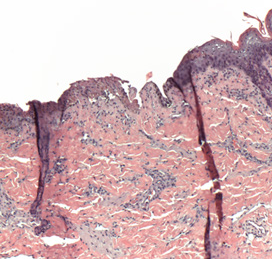
(Case 1): A closeup taken from the composite photomicrograph presented in Image 3. Demarcation between normal and ischemic scalp is distinct; the ischemic tissues are to the left
Case 2
A 7-week-old Asian male was at home under the care of his biological mother who laid him down to sleep, supine on an adult mattress on top of numerous folded blankets. When the mother checked on him approximately 1 to 1-1/2 hours later she discovered him prone and face down, cyanotic, not breathing and flaccid, directly against the soft sleeping surface of the mattress. He was transferred to hospital where he was admitted to the ICU for three days before he was declared brain dead, and taken off of life support. While he was in hospital, he was reportedly turned as per hospital nursing protocol, once per hour.
An autopsy demonstrated numerous complications of treatment for anoxic brain injury. A close aggregate of two red abrasion-like marks (0.8 centimeter diameter, and 2 x 1 centimeters) was in the midline occipital scalp (Image 5). The scalp soft tissues immediately underlying these markings were markedly pale and without ecchymoses (Image 6). The ring of pallor was encircled by prominent vascular congestion within the adjacent deep scalp tissues. Skull fractures, intracranial hemorrhages and cerebrocortical contusions were absent. The superior sagittal sinus was extensively thrombosed, and classic features of venous infarction were in both hemispheres. Histology of the scalp demonstrated early superficial ischemia without extravasation of erythrocytes. Careful review of the scene including doll re-enactment, thorough autopsy and review of the medical records did not refute the circumstances of death. Interviews with the hospital staff revealed that scalp “injuries” were not observed at the initial admission, nor were scalp ulcers detected during the course of hospitalization. The death was certified as an accidental suffocation.

(Case 2): Occipital scalp ulcers following shaving of the scalp hair.

(Case 2): Occipital skull following reflection of the scalp. The subcutaneous soft tissue immediately underlying the cutaneous ulcers have marked pallor; the soft tissues surround the area of pallor are markedly congested.
Discussion and Conclusion
This report describes two infants admitted to hospital with severe anoxic brain injury and associated complications, both of whom subsequently developed ulcers of the occipital scalp. Both infants were declared brain-dead after several days in the ICU. During their stay, both infants were said to have had standard scalp care as per hospital protocol. Neither infant was observed to have scalp abnormalities at the time of hospital admission. At autopsy, occipital ulcers on both infants were determined to be ischemic in origin, and not blunt impact sites.
These two cases clearly illustrate that pediatric IOUs mimicking impact sites may be observed following ICU admission. In the case of non-lethal “injuries”, it is mandatory that the clinician carefully inspect the occipital scalp upon admission to the hospital – evidence of an impact site, if any, will often be present upon initial presentation. When associated with significant scalp ecchymoses, a hematoma may even be observed in the admission computed tomography (CT) scan. In the case of infant death, the forensic pathologist must not only observe and document the presence of apparent impact sites and IOUs, but also utilize routine histology to determine the etiology of the scalp findings. With routine H&E histology, IOUs may be distinguished from impact sites by several factors including epidermal thinning, dermal homogenization, the absence of erythrocyte extravasion, and the lack of stainable free iron. Of course, the presence of a skull fracture underlying an IOU or impact site minimizes the concern of over-diagnosis.
Proper analysis of apparent scalp impact sites will provide information necessary to properly formulate cause and manner of death statements. Clinicians faced with the difficult responsibility of assessing the posterior scalp of a living child (without the benefit of histology) must be aware of the differential diagnosis for these lesions, and the severity of consequences facing an over- (or under-) diagnosis.
Footnotes
Acknowledgements
Drs. Reade Quinton, Joni McClain and Jeffrey Barnard of the Southwestern Institute of Forensic Sciences at Dallas are appreciated for their thoughtful discussions around the topic of occipital pressure ulcers in infants.