
Abstract
The prevalence of the opioid drugs is increasing worldwide. Greater access in turn increases the risk of infants and young children being exposed to potentially fatal concentrations of these drugs, either by accident or through the negligent or deliberate actions of a caregiver. This report reviews opioid-related fatalities in this population and discusses homicidal and accidental poisonings and the possible routes of exposure, including through breastfeeding. As with adults, autopsy findings in fatal pediatric opioid toxicity are nonspecific and such cases may mimic death from natural diseases such as metabolic disorders or channelopathies. A detailed review of the case history together with a complete autopsy and toxicology testing are essential for the correct certification of these deaths. Further challenges arise from the fact that toxic ranges for opioids are not well-defined in the pediatric population, and the forensic pathologist must rely on case reports and small case series’ to assist in the determination of “how much is too much”. Resources such as the National Association of Medical Examiners Pediatric Toxicology Registry (NAME PedTox) continue to be of great value, but depend on the voluntary submission of case data from members. Emerging phar-macogenetic data are revealing genetic variations associated with altered metabolism and tissue distribution of opioids; therefore, molecular autopsy techniques should be considered in these challenging cases, especially where the manner of death is unclear.
Introduction
Fatal poisoning of infants and young children, irrespective of manner of death, is an uncommon event in developed countries. According to the 28th Annual Report of the American Association of Poison Control Centers’ National Poison Data System, there were over 1.5 million exposures in children (defined as ≤20 years of age) reported to 60 poison control centers in the US in 2010, but only 91 resulted in death (1). Of the fatalities, 59 occurred in older children and adolescents (6-19 years). In 2005, the Public Health Agency of Canada reported a crude death rate of 0.3/100,000 persons for unintentional poisonings of children aged 0-19 years (2), while Flanagan et al. reported an age-adjusted mortality rate of 4.6/million children age ≤10 years for the year 2000 in their study on fatal pediatric poisoning in England and Wales (3).
The challenges posed to the forensic pathologist by the relative infrequency of fatal intoxication in infants and young children are compounded by the fact that poisoning may leave no specific anatomical finding at autopsy (4). Correct diagnosis depends on a thorough scene investigation, de-tailed history, complete autopsy and toxicology testing, and may also require other ancillary tests to rule out infectious, genetic or metabolic causes of death. In our jurisdiction, there are published sets of guidelines for forensic pathologists who perform autopsies on infants and children under five years of age, including criminally suspicious cases and homicides (5, 6). According to these guidelines, full toxicology testing is recommended in any case where no anatomic cause of death is identified at the conclusion of the autopsy, and is required where the history or scene information indicates a potential toxicologic contribution to the death, or when the autopsy findings or circumstances of death are criminally suspicious or indicative of inflicted injury. Toxicology testing in any “Death Under 5” case includes, at a minimum, screens that cover alcohols, benzodiazepines, opioids, common drugs of abuse and prescription medications that are potentially fatal in overdose (such as many antidepressants and antipsychotics), and over-the-counter (OTC) medications that are toxicologically significant (e.g., diphenhydramine, dextromethorphan, pseudo-ephedrine). In addition, targeted analysis is performed for cannabinoid metabolites, acetaminophen and salicylates. Additional targeted testing for other drugs not detected in the routine screens (e.g., gamma hydroxybutyrate, digoxin) may be performed at the discretion of the pathologist.
The opioid drugs, natural and synthetic compounds with morphine-like properties, are drugs primarily available through prescription that have high rates of use, misuse and abuse (7, 8). They are commonly prescribed in developed countries for a number of indications (e.g., analgesia, addiction treatment, cough suppression) and their consumption has been increasing dramatically worldwide, more than tripling between 1991 and 2010 (8). This class of drugs is of interest to those investigating pediatric deaths for a number of reasons: rates of opioid use in children for treatment of chronic pain are increasing in North America (9, 10); it has been shown that opioids are frequently implicated in poisoning deaths of young children (3, 11); their prevalence increases the risk of both intentional and accidental administration in children (9); it has been estimated that codeine, methadone, hydrocodone and morphine could be fatal in toddlers with as little as a single dose (11); pediatric fatalities from iatrogenic medication errors have been reported (12, 13); and many opioid drugs cross the placenta and are excreted in breast milk, resulting in potential exposure of the fetus and neonate (7, 14–16).
Evolution of Opioid Use
The United States and Canada represent two of the largest consumers of opioids in the world, and the use of prescribed opioids in Canada is growing. Fentanyl consumption increased by approximately 70% between 2006 and 2010, while that of oxycodone and methadone increased by approximately 50% and 75%, respectively, for the same period (8). The use of opioids for the treatment of pain in children has also been in-creasing. Opioids are currently recommended for the treatment of postoperative pain, and pain from cancer and sickle cell disease in neonates, infants and children (10, 17). Increasing use of opioid medications means there are more opportunities for infants and young children to be exposed to these drugs and develop serious toxicity, whether the exposure is accidental or intentional. Opioid medications that have been implicated in the deaths of infants and young children are listed in
Opioid Medications That Have Been Implicated in Fatal Poisonings of Infants and Young Children
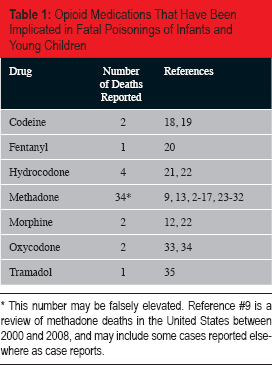
This number may be falsely elevated. Reference #9 is a review of methadone deaths in the United States between 2000 and 2008, and may include some cases reported elsewhere as case reports.
Opioid Related Homicide
Although poisoning is a common form of nonfatal injury, deliberate homicidal poisoning is unusual in North America. In their analysis of American Vital Statistics data for the years 1999-2005, Shepherd and Ferslew (23) found a total of 523 homicidal poisoning deaths with a rate of 0.26/million for the time period in question. The victims were most likely to be at the extremes of age, with infants (≤1 year) and the elderly (≥85 years) having the highest rates amongst all age groups. The rate for infants was found to be 2.05/ million while that for children ages one to four years was 0.49/million for the seven years of the study period. Although the specific methods of poisoning were not detailed, the most common category of intoxicant was “drugs, medicaments and biological substances” (23). In a report by Fujiwara et al. (24), analysis of data from the American National Violent Injury Statistics System revealed that of 72 homicides of children ≤2 years of age, four were a result of poisoning (5.6%). Again, the specific method of poisoning was not described.
A review of the literature confirms that homicidal poisoning of infants and children with opioid drugs is an uncommon, but well recognized phenomenon.
Summary of Measured Blood Concentrations From Cases of Fatal Opioid Poisonings in Young Children

Concentrations are listed as mg/L; where the original source reported the value as a different concentration (e.g. ng/mL), the conversion was calculated for ease of comparison.
Diazepam was also detected at a concentration of 0.044 mg/L
This was an antemortem blood sample drawn in hospital. Postmortem samples were not taken.
Transmitted via breast milk. Mother was taking codeine.
Present as a metabolite of codeine
Promethazine was also detected at a concentration of 217 mgc/L. Both drugs were present as a result of placental transfer.
Breast fed infant of a mother using methadone. The cause of death was given as unascertained.
Even if an opioid medication is administered to a child by a caregiver without malice, the death will typically result in criminal prosecution for homicide or manslaughter (26–28). The increasing prevalence of these drugs in North America, with their sedating effects on fussy children, may lead to an increase in cases of fatal, non-accidental intoxication.
Mention should be made of a special category of homicide: fatal Munchausen syndrome by proxy. In these cases, a caregiver will deliberately simulate or produce signs of illness or disability in a child for secondary gain (e.g., attention from health care workers). These cases typically do not result in the death of the child, although there are reports of mortality resulting from poisoning with clozapine (36), and insulin (3). No reports of cases of fatal Munchausen by proxy involving opioids were found in the literature, but the forensic pathologist should consider this possibility in cases where the history suggests factitious illness.
Accidental Opioid-Related Deaths
Infants and young children are particularly vulnerable to fatal opioid intoxication for both behavioral and physiologic reasons. Older infants and toddlers exhibit exploratory behavior that involves placing objects in the mouth, and fatalities may occur if these objects include pills or methadone containers. In addition, their small size leaves young children vulnerable to medication dosing errors, both at home and in the health care setting. Liquid formulations of opioid medications (such as cough syrups containing codeine or hydrocodone) may result in serious harm or death in the home as a result of imprecise measurement using household spoons or medicine droppers (18, 21). In hospitals, medication doses are calculated based in body weight or surface area, and the small medication volumes admin-istered increase the risk of errors that may result in doses that are manyfold greater than intended (22).
Accidental deaths of young children following exposure to methadone in the home have been reported (29–31). In the majority of these cases, an adult living in the home was enrolled in a methadone maintenance program and bottles were left within reach of a curious toddler. The accidental death of a one-year-old infant has been reported who swallowed a used transdermal fentanyl patch that had been discarded and was found lying on the ground (20), and a case from our jurisdiction involved the death of an 18-month-old boy who ingested an unknown quantity of timed-release morphine sulfate tablets that were left loose on a table in his home. Although the manner of death in this case was ruled an accident following review by a multidisciplinary death review committee, there are jurisdictions where such an incident may lead to criminal prosecution for criminal negligence or even homicide.
Adverse events in a health care setting have also resulted in fatal outcomes in children. A three-year-old boy with sickle cell disease died in hospital of a morphine overdose as a result of the incorrect programming of a morphine pump (12), while a six-year-old boy died of acute methadone toxicity when the opioid was accidentally substi-tuted for meperidine in a dental cocktail used for conscious sedation of patients (13).
Opioids in Pregnancy and Breastfeeding
It is known that opioids cross the placenta during pregnancy, and are excreted in breast milk (7, 14–16). It is also known that rates of opioid misuse are increasing amongst women of child-bearing age (16). Methadone is currently the recommended treatment for opioid dependency in pregnant woman (15, 38), and although studies have shown that there is no increased mortality risk for infants exposed to methadone in utero (16), questions remain about the safety of methadone (and other opioids) in breast feeding (14). Several studies have linked opioid exposure via breast milk to symptoms in infants, such as apnea, bradycardia and cyanosis (39–41), and a case reported in 1977 describes the death of a five-week-old male infant of a methadone-depen-dant mother who was found to have a significant concentration of methadone in his postmortem blood (29). A recent paper from the United Kingdom (35) reports two deaths of infants where the cause of death was thought to be related to methadone toxicity (see
Methadone and certain other opiates such as morphine and codeine are generally believed to be safe to administer to a breastfeeding mother (14, 42–44). However, research in the fields of pharmacokinetics and pharmacogenetics in recent years has led to advances that are of interest to those investigating opioid-related deaths in infants and young children. It is now known that there are several gene variations that can affect the metabolism of opioid drugs, and can lead to either slow metabolism (and a build-up of the active parent compound in the blood-stream) (14, 45, 46), or rapid metabolism (and a build-up of active metabolites such as morphine from codeine) (14, 47). For example, the gene CYP2B6 codes for one of the cytochrome oxidase enzymes that is responsible for the metabolism of methadone in the liver. Variations in this gene can cause slow metabolism of methadone and may result in the accumulation of fatal concentrations in users (45). Similarly, genetic variations in the ABCB1 gene coding for Pglycoprotein (P-Gp), which forms an important part of the blood-brain barrier, can affect the rate at which opioids accumulate within the central nervous system. Decreased function of P-Gp has been associated with lower dose requirements for patients in methadone treatment programs and increased toxicity in breastfeeding mothers and their infants (46, 47). It is therefore possible that opioid related deaths in infants and young children may be linked to inherent genetic variability, and molecular genetic testing may add yet another weapon to the forensic pathologist's armamentarium in these cases.
Autopsy Considerations
As is the case with adult deaths, children who die of opioid toxicity may show no anatomical findings at autopsy. Reported cases have described nonspecific findings such as congestion of organs, pulmonary edema, cerebral edema and early aspiration pneumonia (18, 20, 29). In cases of homicide by poisoning, children may show injuries indicative of ongoing child abuse or evidence of neglect (23). The history may indicate a prior history of acute life-threatening events, apneic episodes, lethargy, poor feeding, or repeated visits to doctors’ offices or hospitals (in the case of Munchausen syndrome by proxy) (3, 23, 25). Availability of opioids in the child's environment may or may not be indicated in the history (32, 33). Full toxicologic analysis is indicated in any pediatric case where a toxicologic cause of death is suspected, or where no anatomical cause of death is identified at the conclusion of the postmortem examination. Samples should include blood from the heart or great vessels for qualitative screening, and from a peripheral source such as the femoral vein for quantitative analysis. Urine, liver (or other solid tissue), stomach contents and hair can also be useful in these cases. When interpreting the toxicology result, the pathologist must remain mindful of the phenomenon of postmortem distribution, which can result in falsely high blood concentrations of opiates such as methadone, morphine, codeine and fentanyl (37, 48, 49).
The National Association of Medical Examiners (NAME) administers the Pediatric Toxicology (PedTox) Registry that may prove a helpful resource in these cases (50). Established in 1985, the registry collects reports of drugs and other substances detected in children under the age of 15. Members voluntarily submit information about cases including fatal intoxications, cases where positive toxicology was considered an incidental finding and cases of nonfatal intoxication. The information is then compiled into a database can be searched by those who have a NAME membership.
Conclusions
With increasing rates of opioid use in Canada and the United States, both illicit and legitimate, the opportunities for young children to be exposed to these drugs are also increasing. Fatal exposures may occur in the home or in the healthcare setting, and may result from accidents or the deliberate actions of a caregiver.
Full toxicologic analysis is an integral part of any death investigation of a child under five years of age. Because poisoning with prescription or non-prescription medications may not have any spe-cific findings at autopsy, such cases can mimic Sudden Infant Death Syndrome (SIDS), infant deaths occurring in unsafe sleep environments, metabolic disorders, Sudden Unexpected Death in Epilepy (SUDEP) or sudden cardiac deaths due to channelopathies. Although what constitutes “routine” postmortem toxicology may vary considerably between jurisdictions, minimal testing should include screens for the common drugs of abuse, prescription medications that are potentially fatal in overdose (narcotics, antidepres-sants, anticonvulsants, antipsychotics, etc.) as well as OTC medications that have been shown to cause significant toxicity in children. The forensic pathologist, coroner or medical examiner must interpret the toxicology findings in the context of the history, scene findings and autopsy findings, and consideration should be given to molecular genetic testing for gene variations that could predispose a child to fatal opiate toxicity.
Footnotes
The author, reviewers, editors and publication staff do not report any other relevant conflicts of interest.