
Abstract
This paper presents a recommended dissection technique for adult hearts. This method allows for complete examination and sampling of the myocardium, cardiac valves and coronary arteries, while preserving the heart and conduction system for potential further study.
Introduction
The dissection of the heart is often the most important element of the autopsy and is the most difficult of the organs to dissect. Appropriate cardiac dissection technique relies on the pathologists’ ability to identify the presence of underlying cardiac abnormalities and previous surgical interventions, and is necessary for preservation of the heart for possible future re-evaluation and studies. The heart is the organ most commonly responsible for sudden unexpected death; therefore, thorough examination with appropriate myocardial sampling and preservation of materials is essential in evaluating such cases.
The following is the preferred dissection technique of an adult heart in a routine autopsy as examined by the cardiac pathologists at the Jesse E. Edwards Registry of Cardiovascular Disease, which is based on previously published techniques (1). The technique is summarized for quick reference in Table 1.
Flowchart of adult dissection technique
Dissection Technique
The first part of the cardiac examination is to determine whether the heart size is normal or enlarged. The heart weight is recorded and then compared to reference range tables previously published, shown in Tables 2 and 3 (2). Heart size is more accurately evaluated when using the body weight reference ranges within the normal Body Mass Index (BMI). If the BMI indicates obesity, body height reference ranges should be used for determining normal heart size, as cardiomegaly often is a pathologic condition associated with obesity.
Predicted Normal Heart Weight (g) as a Function of Body Weight in 392 Women and 373 Men *
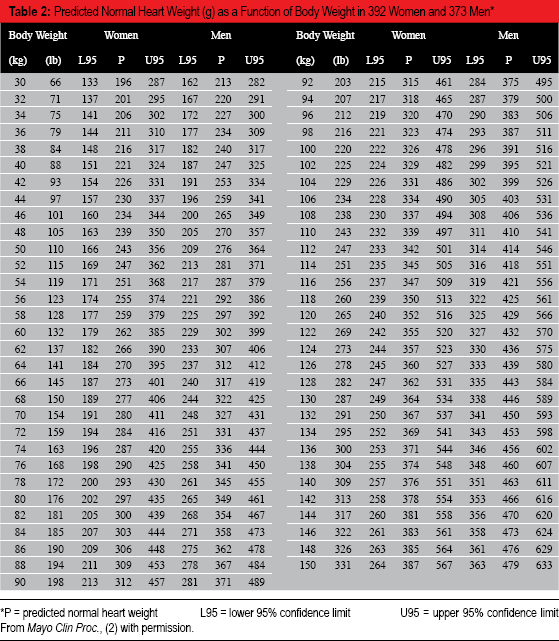
P = predicted normal heart weight
L95 = lower 95% confidence limit
U95 = upper 95% confidence limit From Mayo Clin Proc., (2) with permission.
Predicted Normal Heart Weight (g) as a Function of Body Height in 392 Women and 373 Men *
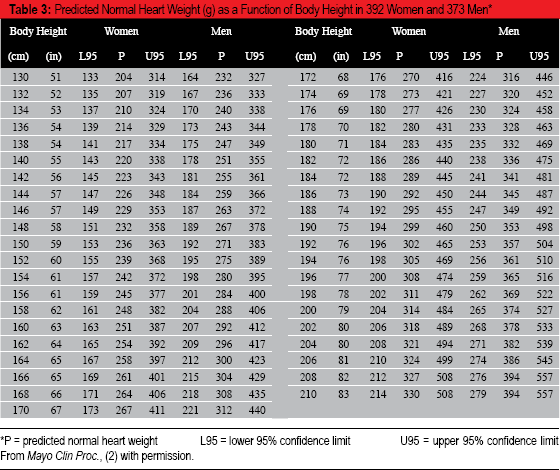
P = predicted normal heart weight
L95 = lower 95% confidence limit
U95 = upper 95% confidence limit From Mayo Clin Proc., (2) with permission.
Once the heart size is determined, the external surfaces of the heart should be examined. This includes documentation of the overall external features of the heart and any previous surgical procedures. If the heart is enlarged, is this due to left-sided enlargement, right-sided enlargement or four chamber enlargement? Additional external features to document include the presence of epicardial nodules, plaques, adhesions or areas of hemorrhage.
Once the external features have been documented, the dissection can continue. The coronary artery dissection is the first step in the dissection of the heart. The coronary arteries should be serially cross sectioned at 3 mm intervals through the entire length of the artery including all major branches. Documentation of dominance should be recorded. Eighty percent of cases will be right dominant, defined as the right coronary artery providing the posterior descending coronary artery which supplies blood to the posterior wall of the left ventricle. Ten percent will be left dominant in which the posterior descending coronary artery arises from the left circumflex coronary artery and ten percent will be co-dominant with a posterior descending coronary artery arising from both the right coronary artery and left circumflex coronary artery. In addition to documentation of coronary arterial dominance, all coronary artery abnormalities should be documented including abnormal origin of coronary arteries, abnormal courses of coronary arteries, aneurysms, luminal stenosis by atherosclerotic disease or other process and/or the presence of coronary arterial thrombosis. In cases with atherosclerotic coronary artery disease, the degree of luminal narrowing and extent of the disease (diffuse or focal) should be noted.
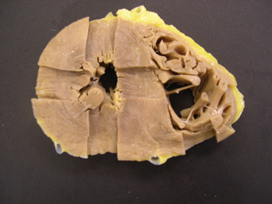
Once the coronary arterial system has been completely dissected, the heart should be placed on the dissecting table with the anterior wall facing up. Three cross sectional slices should be made to the ventricles from the ventricular apex to the mid ventricular level, which is approximately at the level of the papillary muscles (Image 1). The ventricular cross sectional slices allow for more complete visualization of the right and left ventricular myocardium and ventricular septum and provides access for full thickness myocardial sections for histologic review.

Three cross-sectional slices of the ventricles.
Once the ventricular cross sectional slices are complete, the remaining heart should be opened along the direction of flow of blood. Using scissors, the right atrium should be opened from the inferior vena cava to the tip of the right atrial appendage, keeping the superior vena cava intact for potential examination of the sinoatrial node (Image 2). Structures to examine and document within the right atrium include the atrial septal anatomy, patency of the foramen ovale, coronary sinus ostium, right atrial appendage with presence or absence of thrombi, and the connections of the inferior vena cava and superior vena cava with the right atrium.

Right atrial incision, extended to the tip of the right atrial appendage.
Opening of the right ventricle should be through the posterior wall. The knife is placed through the tricuspid valve annulus toward the apex. The knife should be oriented parallel to the ventricular septum approximately 2-3 cm into the ventricular cavity, away from the ventricular septum (Image 3). After making this incision, the tricuspid valve should be examined and any abnormalities documented. Structures to examine and note include size of the tricuspid valve annulus, any changes to the tricuspid valve leaflets, presence of vegetations and the structure of the chordae tendineae. Structures to examine and document within the right ventricle include the right ventricular size, thickness of the compact myocardium and any gross changes to the myocardium. The wall thickness measurement should be done at the mid ventricular level in the posterior wall. The myocardium should be a straight transmural cut and not a tangential section. Only the compact myocardium should be measured.

Right ventricular incision through posterior wall, parallel to septum.
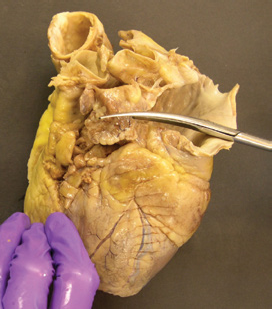
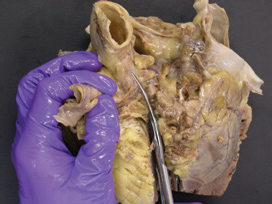
The right ventricular outflow tract cut should be made on the anterior aspect of the heart. The knife is placed anterior to the anterior papillary muscle of the right ventricle and through the pulmonary valve (Image 4A & 4B). This incision will allow for examination of the right ventricular outflow tract, pulmonary valve and pulmonary artery.
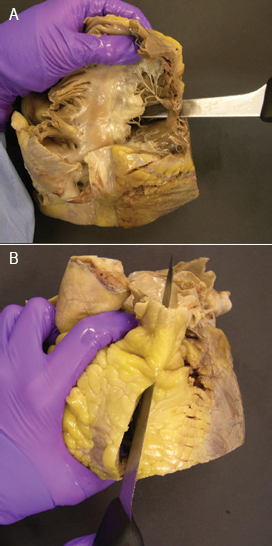
(A) Knife position for right ventricular outflow tract incision. (B) Right ventricular outflow tract incision
Structures to examine within the right ventricular outflow tract include the size of the right ventricular outflow tract, the degree of fat within the anterior wall of the right ventricle and the anatomy of the ventricular septum. The ventricular septum should be intact and this incision allows for complete visualization of the perimembranous region of the ventricular septum, which is the most common site of a ventricular septal defect. This incision also allows for the examination of the pulmonary valve and pulmonary artery. Structures to note include the number of cusps of the pulmonary valve, changes to the valve cusps, in-timal changes to the pulmonary artery, the presence of a persistent patent ductus arteriosus and the presence of thromboemboli.
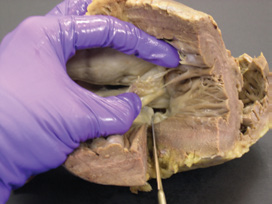
Using scissors, the left atrium can now be opened connecting the right and left pulmonary veins (Image 5). The cut should then be continued through the left atrial appendage, which should be opened (Image 6). Structures to examine in the left atrium include the presence or absence of thrombi in the left atrial appendage, the atrial septal anatomy, and notation of correct pulmonary venous connections.

Left atrium incision
Extension of left atrium incision to the tip of the left atrial appendage
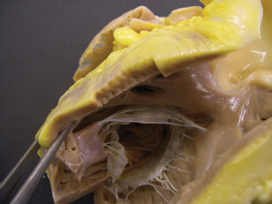
To open the left ventricle, place the knife through the mitral valve oriented with the knife blade toward the lateral wall and between the two papillary muscles (Image 7). Examination of the mitral valve includes evaluation of the annular size, the presence of annular calcification, changes to the mitral valve leaflets, chordae tendineae and papillary muscles. Special note should be paid to whether the chordae tendineae are of normal thickness, elongated or fused and how they insert into the papillary muscles. Chordae tendineae from both leaflets should insert into both papillary muscles. Examine the left ventricular endocardium underlying the chordae tendineae for endocardial friction lesions, which suggests mitral valve insufficiency. Examination of the papillary muscles includes number of papillary muscles, hypertrophic changes and gross myocardial changes. Examination of the left ventricle should document the thickness of compact myocardium of the lateral wall at the mid ventricular level and gross appearance of the left ventricular myocardium.

Left ventricular incision through the lateral wall, between the two papillary muscles
The most difficult aspect of the cardiac dissection is the left ventricular outflow tract incision. The left ventricular outflow tract should always be opened in a routine case. A rare exception is severe aortic valve stenosis. Opening of the left ventricular outflow tract allows for examination of the aortic valve and origins of the coronary arteries. In children and young adults, it is important to document the origins of the coronary arteries prior to opening the aortic valve. This may be accomplished by placing a probe through the ostia in the ascending aorta or via a retrograde approach with a probe placed in the coronary artery and extending retrograde through the ostia into the aorta. This is done to rule out acute angles of origin and anomalous origin of the coronary arteries.
To make the left ventricular outflow incision, visualize the aortic valve (Image 8), and orient the heart so that the anteroseptal wall of the left ventricle is flat on the dissecting table (Image 9). Place the knife immediately behind the anterolateral papillary muscle and cut through the anterior wall. This cut should only extend halfway up the left ventricular outflow tract. The remainder of the incision is made by positioning the heart with the aortic aspect downward on the dissecting table. Using a scalpel, extend the incision to the aortic valve (Image 10). When the aortic valve is visualized, reflect the pulmonary artery anteriorly and the left atrial appendage posteriorly and using scissors, open the aortic valve through the commissure between the right and left cusps (Image 11). This approach allows for examination of the aortic valve and coronary artery ostia, which should now be on either side of the incision (Image 12).

Visualizing the left ventricular outflow tract and aortic valve

Initial left ventricular outflow tract incision
Extension of left ventricular outflow tract incision with scalpel, to the aortic valve
Completing the left ventricular outflow tract incision using scissors, by reflecting the pulmonary artery and cutting through the commissure of the right and left aortic valve cusps

Open left ventricular outflow tract
Examine and document changes to the left ventricular outflow tract including the shape of the ventricular septum and whether the septum is intact. Note any changes to the membranous septum. Examine and document the aortic valve including the number of cusps, any changes to the cusps and the presence of any vegetations or nodules. Structures to examine within the aorta include the presence, absence and extent of atherosclerotic disease and the number and patency of aortic arch branches.
The coronary artery ostia can easily be visualized. The coronary artery ostia should arise centrally from their respective sinuses of Valsalva and below the sinotubular ridge. Two to three ostia for the right coronary artery are common and are a normal anatomic variant. Eccentric origins of the coronary arteries also are a common anatomic variant and are usually located toward the commissure shared with the noncoronary cusp. Abnormalities of clinical significance include single coronary artery ostium, origin of the coronary arteries from the wrong sinus and high origin of the coronary artery ostium above the sinotubular ridge. Ideally, these abnormalities would have been identified prior to opening the left ventricular outflow tract.
Myocardial sections for histologic evaluation are part of the cardiac examination and should include complete transmural sections (endocardium to epicardium) of the four walls of the left ventricle including the ventricular septum (Image 13). Always include a section from the right ventricular outflow tract to evaluate for the presence of arrhythmogenic right ventricular cardiomyopathy (Image 14). Additional right ventricular sections should be taken in sudden unexplained death cases. Other sections should be taken as needed including sections of the coronary arteries if abnormal. A representative section from the mitral valve taken at the inflow incision of the left ventricle is a useful section as it includes the left atrium, coronary sinus, left circumflex coronary artery, mitral valve with annulus and the base of the lateral wall of the left ventricle.
Recommended histologic sections from left ventricle
Recommended histologic section of anterior right ventricle, taken from the outflow tract
Additional Considerations
The approach described here can be applied to any specimen, and provides for a complete examination of the myocardium and valves. Special dissection techniques are not required for any specific disease state or abnormality. Dissecting the heart along the flow of blood does not allow for a complete transmural view of the myocardium from all walls of the right and left ventricles and makes appropriate sections much more difficult. Serial bread loafing of the ventricles to the annulus of the valves is unnecessary and often disrupts the AV nodal region, interfering with possible conduction system examination. A possible deviation from the presented technique is in cases of severe aortic valve stenosis, where opening the valve can destroy the tissue. In those cases, the outflow tract incision need not be extended through the valve. Special incisions such as the four-chamber view may be performed in cases of hypertrophic cardiomyopathy (HCM) for photographic purposes, but is not required for the proper diagnosis of HCM,
Formalin fixation is not required to perform a detailed and appropriate dissection. The heart should be fixed if the four-chamber cut is to be done. Fixation may be helpful in potential legal cases or post-surgical cases, but is a matter of personal preference. Anatomic relationships are often best preserved if the heart is fixed prior to any dissection, to prevent distortion artifacts.
We include a histologic section of the mitral valve in every case as part of our routine set of sections. The mitral valve section includes left atrium, posterior mitral leaflet, posterolateral left ventricular base, circumflex artery and coronary sinus, allowing for several structures to be examined in just a single section. Histologic sections of other valves are taken as needed, in cases of known valvulopathy or if abnormalities are observed.
Specimens with prior surgical procedures present a special challenge, particularly coronary artery bypass (CABG) cases. Evidence of prior surgery should be documented as part of the initial external examination, including the number and location of bypassed arteries and the standard suture lines from bypasss in the right atrial appendage and ascending aorta. The graft vessels should be examined first, prior to any sectioning of the native arteries or ventricular sectioning. Patency of the aortic anastomosis, graft vessel, coronary artery anastomosis and distal native artery should be documented using probes and serial sections. Histologic sections of the graft vessel, coronary artery anastomosis and distal coronary artery for each graft should be taken to confirm patency. We no longer perform post-mortem angiography in our laboratory as we did not find it to be superior to serially sectioning the coronary arteries and viewing them in three dimensions.
This same approach can still be used for the examination of a post-valve recovery donor heart, where the aortic and pulmonic valves have been excised. In such cases, the outflow tract incisions are generally not necessary.
Conclusion
This examination and sampling of the myocardium allows for a complete examination of the myocardium, cardiac valves and coronary arteries while preserving the heart for possible re-examination. The dissection technique also preserves the regions of the sinoatrial and atrioventricular nodes for cardiac conduction system studies, if warranted. This technique can be applied to any adult heart, regardless of premortem diagnoses, with possible additional steps in post-surgical and CABG cases. Modifications of this technique may be required in cases of congenital heart disease, and should be modified in a case by case basis.