
Abstract
Sudden cardiac death (SCD) is a rapid, unexpected death due to cardiac causes. The differential diagnosis includes diseases from all four structural divisions of the heart: the blood vessels, myocardium, valves, and conduction system. Although ischemic heart disease is a common cause of SCD, acute myocardial infarcts and/or coronary thromboses are not always detected and are not required to make the diagnosis of death due to atherosclerotic coronary disease. Some people die suddenly from heart disease with a grossly and microscopically normal heart. Molecular analysis of some of these autopsy-negative, sudden unexplained deaths (SUD) may detect putative cardiac channel mutations.
There are three SCD scenarios that are of particular interest to forensic pathologists: sudden cardiac deaths in young athletes, during criminal altercations (homicide by heart attack), and in other hostile environments. In young athletes, most sudden deaths involve cardiac disease and include cardiomyopathies, congenital coronary artery anomalies, myocarditis, and channelopathies. One must, however, consider other causes in these deaths (e.g., commotio cordis, hyperthermia, sickle cell trait). Homicide-by-heart-attack deaths are those in which the cause of death is an acute exacerbation of underlying cardiac disease, however, the manner is homicide because a criminal act triggered the lethal pathologic cascade. A sudden cardiac arrest may occur in hostile locations with resultant trauma (e.g., while driving a motor vehicle). When the event occurs in the bathtub or other body of water, the question of whether the person died naturally from heart disease or unnaturally from trauma (e.g., drowning) often arises. One should not be mislead by the initial physical surroundings of the death (i.e., in a motor vehicle collision, or swimming pool) and fail to distinguish a natural sudden death from an accidental one.
– William Boyd
Introduction
Sudden cardiac death (SCD) is an unexpected death due to cardiac causes that occurs in a short time period (usually within 1 hour of the onset of symptoms or without symptoms). It happens in an apparently healthy person who is performing everyday activities at the time of the incapacitation. In 2006 in the United States, cardiovascular disease was the proximate cause of approximately 1 of every 3 deaths (1). Almost half of all cardiac deaths can be classified as SCDs and many are the first expression of disease (2). The annual incidence of SCD in the United States has been estimated to range from 180,000 to >450,000 per year (3). This broad range is due to the lack of consensus on a definition, case ascertainment criteria, data sources, and methods of estimation (3). Clinical studies may underestimate the incidence since some decedents never make it to the hospital and reliance on death certificate data may over-estimate it (4, 5). Due to their sudden and unexpected nature, these deaths are commonly reported to the medical examiner/coroner (ME/C) (6). There are several forensic pathologic considerations for the investigation of these deaths. This review will further define SCD and discuss some of the forensic pathologic issues.
Sudden
Although death within one hour is often used in the definition of sudden cardiac death, there is no defined interval. Some studies include deaths that occur within 6 or 24 hours of the onset of symptoms (3, 7, 8). Others, use the term “instantaneous” (like switching off a light) to describe the suddenness of these deaths (8). For medico-legal investigative purposes, the rapidity of the event is an important finding since it may help to limit the magnitude of possible causes of death and can be useful for case triage with regard to decisions of jurisdiction and performance of an autopsy. In fact, a history of recent, prolonged, non-cardiac signs or symptoms, typically would necessitate further investigation (including an autopsy) since other non-cardiac diseases may be the culprit.
With the current state of rapid medical response, some out-of-hospital SCDs may receive sufficient resuscitation to delay death for hours or days. For example, a previously healthy 53 year-old man collapses due to ventricular fibrillation caused by undiagnosed hypertensive cardiovascular disease. Successful cardiac defibrillation is performed minutes after the collapse. He does not, however, regain consciousness due to prolonged cerebral ischemia from the initial event. Two days after his collapse, he is declared dead by neurologic criteria. Despite this extended interval, many would consider this a sudden cardiac death. It would technically, however, be classified as a sudden cardiac arrest (SCA) and not a sudden cardiac death (3).
Sudden cardiac arrest (SCA) and sudden cardiac death (SCD) have two distinct definitions and are not interchangeable (3). According to the American Heart Association and American College of Cardiology guidelines, sudden cardiac arrest is defined as “death from an unexpected circulatory arrest, usually due to a cardiac arrhythmia occurring within an hour of the onset of symptoms, in which medical intervention (e.g., defibrillation) reverses the event.” SCD is defined as “death from an unexpected circulatory arrest, usually due to a cardiac arrhythmia occurring within an hour of the onset of symptoms” (9). Due to the opportunity for further clinical evaluation of the SCA death, a ME/C may decline jurisdiction (or not perform an autopsy) on these deaths but may accept jurisdiction for the out-of-hospital sudden cardiac deaths.
Unexpected
Sudden deaths are not always unexpected. In many jurisdictions, these unexpected (rather than sudden) deaths are required to be reported to the medicolegal investigative system. Primary care physicians may be unwilling or unable to certify these deaths because of the absence of medical history and/or the lack of recent medical evaluation. Some jurisdictions have a 24-hour rule that requires all hospital deaths that occur within 24 hours of admission to be reported to the ME/C. This does not mean, however, that all will be accepted as ME/C cases. Not all sudden and unexpected deaths automatically require a medicolegal investigation or an autopsy. If there is a compelling medical history and clear circumstances, an autopsy may not be necessary (10).
A patient with metastatic pancreatic carcinoma may ultimately have a “sudden” death from a pulmonary thromboembolism due to a deep venous thrombosis that resulted from relative inactivity and the malignancy-induced hypercoagulability. Although this death is sudden, it may not be unexpected to the treating physician or the family. Another example would be a 65 year-old man with coronary atherosclerosis and a history of by-pass graft surgery ten years earlier, who collapses lifeless after mowing the lawn. This death was sudden but it was not completely unexpected from a medical point of view. The opinion as to whether a death is considered “unexpected,” may differ among the death investigator, the treating physician, and the next of kin. Although unexpectedness may or may not affect the investigation, it will certainly affect the next of kin. A death that is unexpected adds an additional element to the emotional burden of the family. As Adelson stated: “Even under the best of circumstances, death is almost always a traumatic experience to the survivors. The emotional impact of death is magnified enormously when it occurs unexpectedly. It is, as it has been phrased, “like being struck by lightning on a sunny day” (11). Medical personnel that interact with families at this most emotional time of their lives, need to be particularly sensitive to their questions and concerns. They often want and need to know why he/ she died and may request an autopsy to answer that question. These concerns should be considered by the ME/C even if these deaths may be reliably certified without an autopsy.
Some clinicians may be uncomfortable to certify an apparent natural death that is unexpected. Most would not have a problem with the patient with metastatic pancreatic cancer but what about the person who collapsed just after mowing the lawn? In that latter instance, the most likely cause of death involves the cardiovascular system. Arteriosclerotic cardiovascular disease includes both coronary and cerebrovascular immediate causes. For a natural cause of death, the death-certification standard required by vital statistics bureaus is a probability (i.e., more likely than not or the best medical opinion) (12–14). Some clinicians may not recognize this degree of certainty and mistakenly believe that a death can only be certified if they are 100% certain of the cause. Even for homicides, ME/C are not required to be 100% certain of the cause and manner of death. An autopsy may disclose information about the immediate cause of death (e.g., ruptured myocar-dial infarct, coronary artery thrombosis), but in the above instance, it is unlikely to change the underlying cause of death (10).
Cardiac
There are numerous causes of sudden unexpected natural death. These include cardiac and non-cardiac (e.g., ruptured cerebral artery aneurysm) etiologies (7, 8, 15). Some studies include pulmonary thromboembolism and aortic disease (e.g., aortic dissection) in the group of SCDs. We will restrict our discussion to the primary cardiac causes of sudden death since they result in the majority of deaths. In addition, the proximate causes of the majority of aortic aneurysms and dissections are atherosclerosis and hypertension, respectively. Forensic dogma holds that 60% of medicolegal autopsies will be natural deaths of which 60% will be due to cardiac causes. Among the cardiac causes, 90% will be due to atherosclerosis. The autopsy findings of a sudden cardiac death, in fact, typically detect some form of ischemic heart disease (7, 15). The other common pathologies of SCD include hypertensive cardiovascular disease, congenital coronary artery abnormalities, valvular disease, myocarditis, and dilated or hypertrophic cardiomyopathies (7, 8, 15).
A study from Spain examined the causes of sudden cardiac death in 216 adults aged 35-49 years that underwent forensic autopsy (16). Ischemic heart disease was diagnosed in 140 (65%) decedents of which 74 had a coronary thrombosis or acute myocardial infarct. The remaining had coronary artery atherosclerotic stenosis and/or myocardial fibrosis. The second largest group consisted of myocardial diseases (e.g., structural cardiomyopathies, myocarditis). Sudden arrhythmic deaths with structurally normal hearts were diagnosed in 10 decedents (5%). These results highlight two important pathologic issues when investigating these deaths.
The first is that sudden cardiac death due to coronary artery atherosclerosis is not always associated with coronary artery thrombosis or an acute myocardial infarct. There often is no acute lesion at autopsy. The detection of an acute myocardial infarct or coronary artery thrombosis is not required to make a diagnosis of SCD due to atherosclerosis. Myocardial infarct is not a synonym for SCD. Some of these deaths occur so suddenly that overt pathologic changes do not have time to develop. Morphologic changes of myocardial infarcts are first detectable by light microscopy from 4-12 hours after the onset of marked ischemia. Coronary artery atherosclerosis may cause lethal cardiac arrhythmias by different pathways. Some of these pathways leave no acute evidence of its occurrence. These purely electrical deaths are commonly seen by pathologists. The likely pathogenesis is myocyte ischemia (due to an imbalance of myocardial oxygen supply and demand usually in the setting of fixed stenoses) that causes a ventricular arrhythmia (17). In addition, the detection of a lethal, acute cardiac process does not alleviate the need to perform toxicology analysis of these deaths. Acute and/or chronic cocaine and methamphetamine abuse may contribute to or cause some of these apparently natural sudden cardiac deaths. Inclusion of such an acute intoxication on the death certificate usually will result in an accidental manner of death, not natural (18, 19).
The second important finding from this study is that people die suddenly from heart disease with a grossly and microscopically normal heart (17, 20). Recent studies have used molecular techniques to examine these hearts that are “too good to die.” A study by Tester and Ackerman, reported 49 sudden, unexpected deaths in the young (143 years old) that had undergone comprehensive medicolegal autopsies and were subsequently referred for cardiac-channel molecular testing. Molecular analysis of these autopsy-negative, sudden unexplained deaths (SUD) detected putative cardiac channel mutations in 35% of the decedents (21).
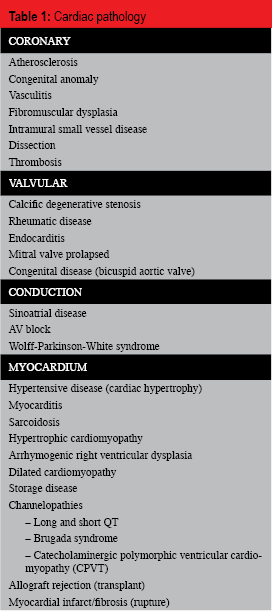
Structurally, the heart can be divided into 4 components: the blood vessels, myocardium, valves, and conduction system. Common findings/diseases can be categorized by these four divisions (Table 1). When the differential diagnosis of a sudden cardiac death is developed, whether it is in the emergency room or the autopsy room, all four parts of the heart should be considered (22).
Cardiac pathology
The examinations performed by a clinician and an autopsy prosector each have their advantages and disadvantages. If there is a survival interval, clinicians can evaluate contractility and valvular function (echocardiography), electrical alterations (EKG), myocyte damage (serologic markers), and vascular stenoses (catheterization). Pathologists are able to examine the heart grossly, microscopically, and molecularly, but can only infer function.
Coronary Circulation
It is a common misconception that a coronary artery thrombosis or acute myocardial infarct occurs in all deaths due to coronary artery disease. As the study from Spain demonstrates, approximately half (47%) of sudden cardiac deaths due to ischemic heart disease have no thrombosis or acute infarct (16). This also is supported by a study of survivors of pre-hospital ventricular fibrillation in which 80/306 (26%) patients were successfully resuscitated and underwent clinical evaluation and diagnosis (23). Among them, 39% had an acute myocardial infarct, 34% had ischemic changes without infarct, and 19% had no EKG changes (23). Of the 80 survivors, 52% never developed clinical myocardial infarcts as documented by serial EKGS. Autopsies were performed on 220 of these SCDs: 58% had acute coronary lesions (ruptured plaques or acute thrombosis), 27% had acute myocardial infarcts, and 37% had no acute vascular or myocardial lesion. Flow limiting chronic coronary artery stenosis (>75%) was detected in 207 (94%) of decedents. Pathologists need to investigate the entire circumstances of the death and not just rely upon the autopsy findings. The pathologist who requires a thrombus or myocardial infarct to certify death as due to coronary artery disease will misdiagnose a considerable percentage.
In addition to atherosclerosis, there are other coronary artery pathologies including arteritides and coronary artery dissections seen in postpartum women (7, 24–28).
Myocardium
Acute or remote myocardial infarcts, myocytes with hypertrophy or disarray, and myocarditis are common autopsy findings in sudden deaths. Myocyte hypertrophy may be a sign of hypertensive cardiovascular disease or hypertrophic cardiomyopathy. Hypertrophic cardiomyopathy (HCM) is an autosomal dominant inherited disease of cardiac myocytes that results in left ventricular hypertrophy. A number of associated mutations have been identified which primarily involve genes encoding for sarcomeric proteins (7, 29–34). The most common pattern of hypertrophy is highly characteristic and results in a disproportionately thickened interventricu-lar septum compared to the left ventricular free walls (7, 29, 35). Microscopic examination of the septum shows myocyte “disarray”, referring to a bizarre, intersecting arrangement of myocytes with interstitial fibrosis (7, 29, 35).
Myocarditis is diagnosed histologically by the light microscopic detection of infiltrating lymphocytes and myocytolysis and has a variety of causes (36–41). Major cardiac symptoms of myocarditis typically occur over time and include heart failure and structural changes (dilation). Sudden fatal arrhythmias, however, also can occur with myocarditis as the myocardium may become unstable due to the inflammation, edema, myocyte necrosis, and fibrosis. Sudden death may occur in either the active or healed phases of the disease. These sudden arrhythmic deaths often come to the attention of the ME/C. Histologically, in suspected myocarditis deaths, it is important to sample the heart adequately as the inflammation may be patchy in the early phases.
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a common cause of SCD in Italy (29, 42). It is an autosomal dominant inherited disease of the myocardium resulting in a thin-walled, dilated right ventricle with a high propensity for cardiac arrhythmias (29, 43–47). It is caused by mutations in genes encoding desmosomal proteins (7, 29). The disease is characterized by myocyte atrophy associated with fibro-fatty replacement most commonly affecting the right ventricular free wall (7, 29). The disease process may be segmental resulting in false-negative endomyocardial biopsies.
Molecular studies have not only discovered mutations for structural cardiomyopathies (myosin, troponin) but also in myocyte electrolyte channels (sodium, chloride, calcium) which have further elucidated syndromes that had been previously only recognized by clinical and electro-cardiographic features (e.g., Brugada syndrome, long QT syndrome) (21, 48–53). These “chan-nelopathies” are a group of genetic diseases affecting the electrical system of the heart caused by mutations in genes encoding ion channel proteins and are a recognized cause of SCD in the general population (49, 52). Cardiac “channelopathies” should be considered when no structural cardiac abnormality or extra-cardiac cause of death has been identified.
Valves
Sudden death due to valvular disease is commonly due to aortic stenosis or chordal rupture of the mitral valve. Since the etiology of the valvular disease is the proximate cause of death, one must determine if the aortic stenosis is due to a bicuspid congenital anomaly, senile degenerative/dystrophic calcification, etc. For the flail mitral valve, the proximate cause of death may be mitral valve prolapse (MVP) or a myocardial infarct involving a papillary muscle due to coronary artery atherosclerosis.
Over time, aortic stenosis results in systolic overload and left ventricular hypertrophy. Common signs and symptoms include exertional angina, syncope, and dyspnea. Since the likelihood of sudden death is increased once a person is symptomatic, it is recommended that virtually all symptomatic patients undergo surgery (54–58). The risk of sudden death in asymptomatic adults is low but does occur (57–59). The mechanism of sudden death is related to myocardial ischemia and a subsequent arrhythmia (60). Increased ventricular pressure and myocardial hypertrophy may increase myocardial oxygen consumption (hypertrophy, increased left ventricular systolic pressure, increased left ventricular ejection time) and decrease coronary artery flow reserve (decreased aortic pressure, increased left ventricular diastolic pressure, and decreased diastolic time). This may result in ischemia particularly in the subendocardium. At autopsy, subendocardial ischemia (as evidenced by myocytolysis) is evidence of the arrhythmogenic substrate.
Mitral valve prolapse (MVP) due to myxomatous degeneration is the most common cardiac abnormality in the general population and is usually asymptomatic but has been associated with arrhythmias and sudden death (7, 29, 61–64). Examination of the heart at autopsy shows redundant, myxomatous mitral valve leaflets. Deaths attributed to MVP typically involve an otherwise healthy person who has a sudden death and the only pathologic finding is mitral valve prolapse (62). Since MVP is such a common disorder, it is possible that some of these “MVP” deaths may actually have been caused by an unrecognized channelopathy.
Conduction system
Aside from the myocardium, the SA and AV node and bundle of His are the major components of the conduction system of the heart. Ischemia (nodal artery dysplasia) or myocardial lesions (e.g., sarcoidosis) may interfere with the signal transmission (26, 65–69). By-pass tracts also may cause re-entrant arrhythmias. In select instances, microscopic examination of the conduction system may be of benefit (68, 70, 71).
Mechanisms
Another approach to investigate SCD is to consider the mechanism of death. Arrhythmias are the most common final pathway for many cardiac diseases. The onset of the arrhythmia results in ineffectual cardiac output and subsequent global ischemia and irreversible cell death. The majority of sudden cardiac deaths have arrhythmic mechanisms involving myocardial ischemia. Other pathologic processes (such as a channelopathy or cardiomyopathy) also may result in an arrhythmia. Aside from arrhythmias, there also are mechanical mechanisms of cardiac death. Clinically, this may be seen as pulseless electrical activity (PEA) or electromechanical dissociation (EMD). In these instances, the electrical activity of the heart is intact, however, the heart is unable to provide cardiac output. It is “on” but not pumping blood. Cardiac tamponade, sudden valve failure (e.g., flail mitral leaflet), myocardial rupture, or an air or thromboembolism may impair cardiac output without initial rhythm affects resulting in PEA.
Clinicians frequently equate mechanisms of death with causes of death. Since there is an ultimate cardiac arrhythmia in virtually all deaths, some clinicians focus on the terminal cardiac event instead of the underlying cause. Thus, clinicians may use the term “myocardial infarct” to denote any sudden death. There is a risk of an over-certification of deaths as due to heart disease because of this focus on the terminal event (72).
Specific Forensic Issues
There are certain sudden cardiac deaths that are of particular forensic interest. These include sudden cardiac deaths in young athletes, during criminal altercations (homicide by heart attack), and those that occur in other hostile environments (e.g., swimming pools, driver's seat of a motor vehicle) where there is a potential for trauma.
Sudden death in young athletes: (42, 73–78)
Sudden death in young, previously-healthy athletes, although relatively uncommon, is invariably unexpected and often results in much public interest (29, 35, 79–80). The majority are of cardiac etiology and include cardiomyopathies, congenital coronary artery anomalies, myocarditis, and channelopathies. Given the heritable nature of some of these conditions, determining the cause of death is crucial to provide the family with an explanation for the sudden loss and to determine the need for genetic counseling and/or screening of at-risk family members.
Despite increasing interest in this topic, there are few long-term, large-scale studies estimating the prevalence of sudden death in athletes in the United States. Maron and colleagues assembled a national registry of 1,866 sudden athlete deaths in the United States over 27 years including both high school and college athletes in a wide variety of organized sports (79). Their findings suggest that the incidence of sudden death in athletes may have been previously underestimated and, although still relatively low, occurs at a rate of fewer than 100 per year.
In keeping with the definition of sudden cardiac death, SCD in athletes occurs most commonly during or immediately after physical exertion in training or competition (29, 79). Sudden cardiac death should be distinguished from other causes of sudden death during sports activities that include heat stroke, sickle cell disease/trait, bronchial asthma, and illicit drug use (29, 57, 79, 81, 84). In the Maron registry, 56% of sudden deaths were of cardiac etiology and trauma accounted for 25% of deaths including 3% due to commotio cordis (see below) and another 2% due to hyperthermia. Non-traumatic, non-cardiac causes of death (e.g., asthma) and unresolved causes each accounted for 8% (79).
Specific causes of sudden death in athletes differ by age. In a comprehensive review of sudden death in athletes, Pigozzi and Rizzo divided athletes into “young” (≥ 35 years) and “older” athletes (> 35 years) (29). In the “young” group, the vast majority of sudden cardiac deaths were attributed to structural cardiac abnormalities, most commonly an inherited cardiomyopathy or congenital coronary artery anomaly. In the “older” athletes, atherosclerotic cardiovascular disease was most common followed by valvular and hypertensive cardiovascular diseases (29, 85).
Causes of sudden cardiac death in athletes also differ by geographic region. In the United States, the most common causes of sudden cardiac death in athletes are hypertrophic cardiomyopathy (36%) and congenital coronary artery anomalies (17%) (79). In Italy, the most common cause is arrhythmogenic right ventricular cardiomyopathy followed by coronary artery disease (29, 35, 80).
Hypertrophic cardiomyopathy (HCM) is the most common cause of SCD in young athletes in the United States, particularly in Black males (29, 35, 79–80). Mild cases of hypertrophic cardiomyopathy must be distinguished from the physiologic hypertrophy induced by rigorous exercise (the “athlete's heart”) (80). In the athlete's heart, the left ventricular hypertrophy is symmetrical and associated with an increased end-diastolic cavity dimension, while the hypertrophy in HCM is asymmetrical and not associated with dilation of the left ventricular cavity (29, 80, 86). Family history may help to establish the diagnosis as most athletes who die from HCM have at least one affected first-degree relative (29, 35).
Congenital coronary artery anomalies (CCAAs) are the most common cause of SCD in female athletes (29). Anomalous origins of the left main coronary artery from the right coronary sinus and of the right coronary artery from the left coronary sinus are the most common anomalies found at autopsy (29, 35). CCAAs are believed to exert their lethal effects through exercise-induced myocardial ischemia; for example, an anomalous left main coronary artery arising from the right coronary sinus may become compressed between the aortic and pulmonary trunks (80).
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a rare cause of SCD in athletes in the United States but is the most common abnormality found in young athletes who die suddenly in areas of northern Italy (29, 80). The regional difference has been attributed to a higher prevalence of mutations in the Italian population, although it has been suggested that a lower incidence of SCD from other causes (due to mandatory pre-participation screening of athletes) may be responsible for the relatively high rate of deaths due to ARVC (29). A study that compared death rates in Italy (Veneto) and United States (Minnesota) found that sudden cardiovascular deaths in young competitive athletes have not differed significantly in recent years despite the use of preparticipation screening 12-lead electrocardiograms (EKGs) in Italy (87).
Cardiac “channelopathies” should be considered when no structural cardiac abnormality or extra-cardiac cause of death has been identified. Sports-related SCD is most frequently associated with long QT syndrome and catecholaminergic polymorphic ventricular tachycardia (CPVC) which results in an exercise-induced ventricular tachycardia (29).
Commotio cordis or “cardiac concussion” has been reported to be the most common cause of sudden death in young athletes without underlying heart disease (29, 80). It refers to a sudden cardiac arrest following blunt impact to the chest that results in ventricular fibrillation (88). Link et al, using a swine model, found that when the chest impact occurred between 30-15 msec before the peak of the T-wave on the EKG, this caused ventricular fibrillation in 9 of 10 instances (89). Accordingly, these deaths are most frequently seen in sports involving high-speed projectiles, such as baseball, lacrosse, or hockey (29, 90). Although it technically falls into the category of trauma-related sports deaths, it is included here because it may occur without structural signs of trauma at autopsy. Commotio cordis occurs most commonly in athletes under the age of 17 which is likely related to the size and high compliance of the chest wall in this age group (29). Since the manner for these commotio cordis deaths is accident, an autopsy as well as a thorough investigation is needed to make the diagnosis. The investigation requires interviews with primary sources (i.e., those that saw the event) in order to determine if there was chest impact seconds before the collapse.
Homicide by heart attack: (91–92)
Homicide-by-heart-attack deaths are those in which the cause of death is an acute exacerbation of underlying cardiac disease, however, the manner is homicide because a criminal act triggered the lethal pathologic cascade. The criminal activity results in a physiologic stress response that causes the acute fatal event in the predisposed person. A sudden cardiac arrest may follow a verbal dispute or physical alteration that includes non-life-threatening injury. In these complex cases, the pathologist must first determine if there is any physical injury and then whether the injury caused or contributed to death. If it did, then these deaths usually are certified as homicides (93). In other instances when there is either no injury or no life-threatening injury, a homicidal manner, however, still may be appropriate (91). This is most commonly seen in a person with advanced heart disease in which the stress of a hostile altercation results in a sudden cardiac arrest. The most commonly encountered underlying cardiac disease is hypertensive and/or arteriosclerotic cardiovascular disease, however, other types may predispose to a cardiac arrhythmia. Coronary arteries with aberrant origins, congenital valve disease, and other congenital cardiac anomalies may be implicated with an assault in the cause of death.
Even without underlying cardiovascular disease, stress can result in considerable physiologic disturbances of the heart (93–94). In these instances, an emotionally precipitated (catecholamine driven) cardiac arrhythmia occurs and one may see acute myocyte injury (91, 93). In a study of victims who died as a direct result of physical assault without sustaining internal injuries, 11 of the 15 decedents had myofibrillar degeneration of the heart (“cardiac stress cardiomyopathy”) (93). A similar phenomenon has been described in the living with so-called acute, stress-induced (takotsubo) cardiomyopathy (94–96).
The history of an assault and/or exposure to an emotionally stressful situation preceding a cardiac event usually is obtained through a careful investigation. The autopsy is necessary to confirm or refute acute life-threatening injury, underlying cardiac disease, and acute myocyte injury. Cardiac disease or acute myocardial injury in five decedents who had a recent history of assault or emotional stress associated with criminal activity was reported in an autopsy series (92). The autopsy findings included atherosclerotic cardiovascular disease, recent and remote myocardial infarcts, and acute cocaine intoxication which can increase the risk of a cardiac arrhythmia (92).
In some instances, the determination of the manner of death may be complicated if there is no life-threatening physical injury nor any evidence of physical contact between the victim and the assailant (91). For these deaths, any unauthorized and offensive physical contact or a threatening action (e.g., pointing a gun at a person) would typically still result in a manner of homicide (97). For example, one report describes a 67-year old woman walking in a parking lot of a grocery store where she was stopped and threatened by a teenager demanding her purse. She refused and the boy struggled with her for the purse, threatening to kill her if she did not comply (92). She was able to break free, run into the store, and tell others what happened before she collapsed. At autopsy, there was no evidence of acute injury but there was hypertensive and atherosclerotic cardiovascular disease with cardiac hypertrophy, marked coronary artery atherosclerosis, and a remote myocardial infarct (92). The cause of death was certified as: cardiac arrhythmia due to hypertensive and atherosclerotic cardiovascular disease during an emotionally stressful event (victim of a robbery attempt). The manner of death was homicide (92).
Davis described five criteria to evaluate these cardiac-related homicides (91). These include: a criminal act; the decedent should recognize the threat to personal safety; highly emotional circumstances; collapse and death must occur during the emotional response period; and the demonstration of an organic disease (91). The revision of these criteria by Turner et al. focuses on physical contact and re-works the criteria (92). They state that the “action of the perpetrator toward the victim should be of such severity and have sufficient elements of intent to frighten, injure, or kill, either in fact or in statute, so as to lead to a charge of homicide in the event that death resulted from physical injury” (92). The National Association of Medical Examiner's “A Guide for Manner of Death Classification,” states that fatalities resulting from “fear/fright induced by verbal assault, threats of physical harm, or through acts of aggression intended to instill fear or fright may be classified as homicide if there is a close temporal relationship between the incident and death” (13). Such circumstances are considered above and beyond the stresses of “everyday living” especially when they occur during the commission of a crime and the cause and manner of these sudden deaths following such an encounter should take into consideration these events.
Sudden cardiovascular death in hostile environments
A sudden cardiac arrest may occur in unusual locations during a variety of activities. When the event occurs in the bathtub or other body of water, the question of whether the person died naturally from heart disease or unnaturally from trauma (e.g., drowning) often arises. The same question may be considered for the driver found dead in an automobile after a collision. The autopsy findings (cardiovascular disease in the absence of lethal trauma) in conjunction with the circumstances may be useful in the proper certification.
Deaths in the bathtub or larger bodies of water may cause diagnostic dilemmas with regard to the cause and manner of death (98). Did the person have their sudden cardiac event while in the water or did they drown? Since there are no pathognomonic findings to make a diagnosis of drowning, one must rely on the circumstances of death. If there is an acute cardiac finding, the diagnosis may be more clear. There are some ME/ Cs, however, who still may certify such a death as drowning despite detection of a coronary artery thrombosis or acute myocardial infarct (99). Due to the high likelihood of death following a cardiac arrest due to an acute coronary thrombosis, it is reasonable to certify these deaths as due to heart disease (natural) despite the subsequent submersion (99). The likelihood that a person would survive this out-of-hospital cardiac arrest is extremely unlikely, whether or not the person subsequently submerged in water. There is no need to invoke the drowning to explain the death in these circumstances. Even without an acute thrombosis, however, advanced chronic heart disease is sufficient to certify the death as a natural sudden cardiac death with the proper investigative circumstances (e.g., a former Olympic swimmer observed suddenly unresponsive in a health club swimming pool).
Sudden natural death “at the wheel” is a well know and described scenario of motor vehicle deaths (100–105). Although sudden death may occur so quickly that it has been compared to “turning off a light,” there may be a prodrome of a few seconds in which the person is aware of symptoms. Palpitations, light-headedness, headache, or nausea may occur. This likely explains why low speed collisions (or none at all) are typically seen when these sudden deaths involve the operator of the motor vehicle. The driver may sense something is wrong and try to stop or steer the car to the side of the road (104). A study of sudden natural death among automobile drivers in Baltimore found that heart disease was the most frequent cause of death in these drivers (104). Of 81 deaths, 80 were due to cardiovascular disease effecting either the heart, aorta, or brain. Among these 80 decedents, 25 had acute coronary thromboses or myocardial infarcts while 40 had only chronic arteriosclerotic or hypertensive cardiovascular disease. There was little damage to property and no serious injuries to pedestrians, passengers, or other drivers. More than half of the drivers were apparently able to stop the vehicle before a collision (104).
The absence of lethal mechanical injuries in conjunction with advanced heart disease is not pathognomonic for a sudden cardiac death at the wheel. The absence of obvious lethal injury in a motor vehicle fatality warrants further investigation: a posterior neck dissection to exclude occult trauma, carbon monoxide analysis, and scene investigation to exclude positional or traumatic as-phyxial mechanisms.
Conclusion
Sudden cardiac deaths continue to be among the most common deaths investigated by ME/C systems and it is vital that these deaths are properly recognized and certified. Acute myocardial infarcts and/or coronary thromboses are not required to make the diagnosis of atherosclerotic cardiovascular disease. Despite the detection of advanced heart disease, one should not fail to consider and investigate a contributing intoxication with appropriate toxicologic analysis. Although cardiac disease is frequently the cause of sudden death in athletes, one must consider other etiologies (e.g., commotio cordis, asthma, hyperthermia, sickle cell trait). Homicide-by-heart-attack does occur and one must use strict criteria when making this determination in order to maintain consistency and fairness. One should not be mislead by the initial physical surroundings of the death (i.e., in a motor vehicle collision, or swimming pool) and certify a natural sudden death as an accidental death simply due to the initial impression.