
Abstract
Sudden unexplained deaths in apparently healthy individuals (newborn through adult) pose a vexing challenge to medical examiners, law enforcement and society as a whole. Recent advances in “molecular autopsies” have begun to uncover the mystery surrounding sudden unexplained deaths by identifying mutations that can result in or predispose an apparently healthy individual to sudden death. Genetic risks of sudden unexplained deaths have been studied from several different perspectives, and categorized generally by systems, including: cardiac, nervous, immune, and metabolic. This article reviews the genetic risks in sudden unexplained deaths, presents the current state and challenges of molecular investigations, and sheds light on future directions in sudden unexplained death investigations.
Introduction
Sudden unexplained death is sudden death in apparently healthy individuals (newborn through adult), which remains unexplained after a thorough investigation including a complete autopsy, examination of the death scene and review of clinical history. This poses a vexing challenge to medical examiners, law enforcement and society as a whole. On the one hand, there is a general awareness that sudden unexplained deaths, especially in infancy, can be a natural, although devastating event. On the other hand, there is often an underlying suspicion on the part of the law enforcement and society about the validity of a determination of sudden natural death especially when the decedent was healthy and there were no obvious environmental or physical stressors, such as strenuous physical activity, preceding death. Such suspicions can have additional consequences in that they can make a second victim of innocent grieving family members who are trying to cope with a life changing loss.
Each year in the United States, more than 4,500 infants die suddenly with no immediately obvious cause. (1) The prevalence of sudden unexplained death (aged >1-22 years) has been estimated to be greater than 4,000 annually in the United States. (2) Clearly there is a need for the scientific research community to aid medical examiners in determining cause of death in sudden unexplained deaths, and one of the most promising areas of such research is molecular genetics. Recent advances in “molecular autopsies” have begun to pull back the shroud of mystery surrounding sudden unexplained deaths by identifying mutations that can result in or predispose an apparently healthy individual to sudden death.
While molecular testing is not yet commonly performed, it has become a routine part of the workup of sudden unexplained deaths at the New York City Office of Chief Medical Examiner (OCME). This article reviews the genetic risks to be considered in these cases and presents the current state and challenges of the molecular investigations, and sheds light on future directions.
Genetics of Sudden Unexplained Death
Over the decades, genetic risks of sudden unexpected deaths have been studied from several different perspectives, and categorized generally by systems, including: cardiac, nervous, immune, and metabolic. The majority of these studies focused on cardiac conduction and the central nervous system. Different methods have been used to study these systems, including molecular, biochemical, immunohistochemical, and imaging. Molecular studies have focused mostly on individual candidate genes; whole genome wide studies are rare.
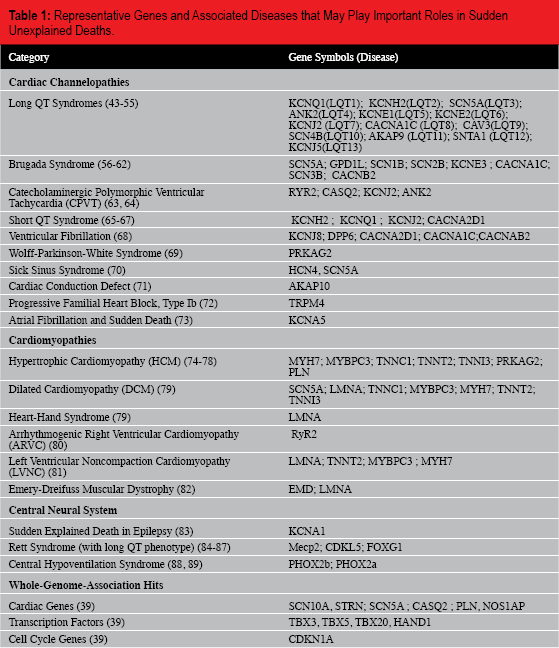
The following sections provide a review of the genetic risks that have been studied in sudden unexplained deaths. Representative genes and related diseases are summarized in Table 1.
Representative Genes and Associated Diseases that May Play Important Roles in Sudden Unexplained Deaths.
Cardiac System
The first molecular evidence demonstrating the effect of a gene defect in a near sudden death event was published in 2000 by Peter Schwartz and colleagues (3). In this study, a sequence variant, S941N, in a cardiac sodium channel gene, SCN5A, was identified in a near-SIDS patient. Furthermore, a prolonged QT interval on the patient's electrocardiogram was observed, and in vitro ion channel functional analysis of the mutant channel supported a causal effect of the gene defect on ion channel activity. This study came a year after the first population based study, which concluded that prolonged QT intervals on electrocardiograms are strongly associated with sudden infant death (4).
Heart rhythm is directly related to the function of the cardiac ion channels for Na+, K+, and Ca2+. Through selective permeability and the gaiting properties of the cardiac ion channels, ions flow across the membranes of myocardial cells, often in a voltage-dependent manner, which in turn generate myocardial action potentials. When measured on the body surface, the different phases of the action potential (0-4) correlate to the standard wave observed on the electrocardiogram (P, QRS, and T). Spatially and temporally tightly regulated action potential initiation and propagation are the molecular basis for regular myocardial cells contractions, and hence, heart rhythms. Abnormal ion channel function changes the duration and/or shape of the action potential and alters the surface electrocardiogram. Such changes may result in lethal arrhythmias, in particular Torsade de Pointes-type polymorphic ventricular tachycardia that can progress to sudden death. Comprehensive review on this topic has been illustrated by other authors (5).
Genes encoding most of the cardiac ion channels (Na+, K+, and Ca2+) have been mapped, cloned, and sequenced. Defects in these channel genes are known to cause a group of heritable cardiac arrhythmia syndromes, collectively known as channelopathies, including long QT syndrome, Brugada syndrome, short QT syndrome, catecholaminergic polymorphic ventricular tachycardia (CPVT), familiar ventricular fibrillation, and others. Each of the syndromes is typically associated with a characteristic change in EKG (5, 6). Although syncope is a primary symptom in some heritable channelopathies, only about half of patients exhibit symptoms. Channelopathies are often undetected prior to sudden death in apparent healthy individuals with structurally normal hearts, and consequently are not recognized as the cause of death without molecular testing.
It should be noted that, in addition to dysfunctional ion channels per se, proteins involved in folding, assembly, or trafficking of the ion channels, have also been shown to elicit cardiac arrhythmias and sudden death in a structurally normal heart (7). Table 1 summarizes major cardiac channelopathy syndromes and known disease causing genes.
Several large, independent population-based studies (8–11), including testing results from the NYC OCME, have demonstrated that defects in channelopathy genes are responsible for 10 -15% of sudden unexplained deaths.
Cardiomyopathies, on the other hand, are often not thought to be the cause of sudden unexplained deaths. When dealing with cardiomyopathies, structural cardiovascular changes are usually evident at autopsy to explain the cause of sudden death; however, occasional case reports have implicated changes in genes known to cause myocardial structural changes found in sudden unexplained death with structurally normal or subnormal hearts (12, 13). It is thought that the myocardial structural gene mutations may affect the cardiac conduction system and result in cardiac arrhythmias before structural changes become apparent. Candidate genes responsible for many cardiomyopathies including familial hypertrophic cardiomyopathy, dilated cardiomyopathy, arrhythmogenic right ventricular cardiomyopa-thy (ARVC), left ventricular noncompaction cardiomyopathy (LVNC), etc, have been cloned, but the prevalence of this group of diseases in sudden unexplained death remains to be determined.
Central nervous system
The focus of central nervous system involvement in sudden unexpected deaths in infants has historically been the brainstem. The serotonin pathway in the brainstem has been studied by several groups, including Hannah Kinney's. The serotonergic (5-hydroxytryptamine [5-HT]) neurons in the medulla oblongata project extensively to autonomic and respiratory nuclei in the brainstem and spinal cord and help regulate homeostatic function.
Using biochemical (high performance liquid chromatography and western blotting) and tissue autoradiography to study 41 SIDS cases and seven controls of infants with a known cause of death, the study concluded that SIDS was associated with lower 5-HT and its key biosynthetic enzyme (tryptophan hydroxylase (TPH2)), consistent with a disorder of medullary 5-HT deficiency (14).
To confirm this finding a large study cohort and controls are required. Limited molecular studies on 5HTT gene common polymorphisms have not been helpful (15–18).
Immune system
A relationship between sudden infant deaths and genes of immune system dysfunction has been explored. Molecular studies primarily have focused on the common polymorphisms in the interleukin genes (IL-6 (19), IL-10 (20, 21), and IL-1RN (22- 24)) and complement pathway (C4) (25, 26). The results from different groups are not consistent, and a solid association has not yet been established. The immune defense system is highly complex; therefore, it is understandable that a limited gene polymorphism study is futile. A systematic molecular approach examining coding and regulatory regions of multiple genes involved in the immune system is needed to determine the contribution of immune system dysfunction to sudden unexplained deaths.
Metabolic system
Metabolic and energy production pathway defects, primarily involving carbohydrates and fatty acids, have been implicated in sudden unexplained deaths (27–30). Fortunately, these groups of devastating and often treatable diseases, such as medium-chain Acryl-CoA dehydrogenase (MCAD) deficiency (31), have been on the expanded national newborn screening panel since early 2002 (27–30), largely due to the developments in tandem mass spectrometry. The expanded newborn screening program mandates testing for all US-born children and is designed for early diagnosis and intervention. Nevertheless, in large cities like New York City, medical examiners are constantly challenged with the possibility that a sudden death may in fact be due to a devastating metabolic disease which was not previously screened in the home country of the decedent. Obtaining newborn screen record of a decedent, or routinely ordering post-mortem metabolic screening for sudden unexplained death cases, is recommended.
The roles of other metabolic diseases not on the current newborn screening panel, such as mitochondrial disorders, have also been studied in sudden unexplained deaths. In general, mitochondrial diseases usually have obvious clinical findings that are not present in these cases, unless the cardiac conduction system is primarily affected (32). Polymorphic variations in the D-Loop (33, 34) and coding region (35, 36) of the mitochondrial genome (37) have been examined in sudden unexplained deaths. The significance of the findings remains to be validated.
Whole genome involvement
The standard molecular approach to the genetic risks of sudden unexplained deaths involves limited target gene analysis, usually by a direct sequencing method. This testing method allows identification of likely disease-causing variants; however, it is costly and time-consuming. With the advancement of array-based and next-generation sequencing technologies, research into the genetic causes of sudden unexplained deaths is expected to accelerate. Copy number changes of certain regions of the genome have been recently reported in three sudden infant death cases, using array-based technology (38), and genome wide studies of all coding regions seems a likely next step as sequencing prices continue to fall.
Whole genome wide association studies (GWAS) have identified several genes which may play important roles in sudden unexplained deaths. GWAS are not candidate-gene driven, and are unbiased in their evaluation of associations between a phenotype and genes. In a recent study, a genome-wide association meta-analysis involving more than 47,000 individuals found that 22 loci are associated with QRS duration (39). These loci map to or near genes in pathways with established roles in ventricular conduction such as: sodium channels, transcription factors and calcium-handling proteins, but also point to previously unidentified biologic processes, such as kinase inhibitors and genes related to tumorigenesis. Further evaluation of the role of all 22 loci in sudden unexplained deaths is warranted. (Table 1.)
Current State of Molecular Investigations of Sudden Unexplained Deaths at the New York City Office of Chief Medical Examiner
Recognizing the importance of molecular investigation in sudden unexplained deaths, the OCME of New York City established a molecular genetics laboratory within the agency in 2003. The laboratory is headed by an American Board of Medical Genetics certified molecular geneticist, staffed with several criminalists and experienced PhD-level research scientists, accredited by College of American Pathologists (CAP), and located in a state-of-the-art facility.
After extensive method and technology validation on post-mortem samples, a molecular analysis panel for inherited cardiac arrhythmia genes was put on-line in 2008 for routine investigation of sudden unexplained deaths in New York City. The test panel consists of all or selected exons in six major cardiac ion channel genes (KCNQ1, KCNH2, SCN5A, KCNE1, KCNE2 and RyR2) in which disease-causing sequence variants have been previously reported in sudden unexplained death. Genomic DNA is isolated from post-mortem tissue samples preserved in RNAlater® or dry blood samples on paper. DNA is amplified by the polymerase chain reaction and the amplification products are used as templates for bidirectional (or repeat uni-directional) sequencing using BigDye® terminator chemistry followed by automated capillary electrophoretic separation. Exons and intronexon boundaries are analyzed. The clinical relevance of sequence variants is evaluated in accordance with the American College of Medical Genetics Recommendations for Standards for Interpretation and Reporting of Sequence Variations: Revision 2007 (40).
This testing panel has been useful not only in determining cause of death, but also for the clinical management of the high-risk families. As a routine practice, medical examiners at OCME advise family about a positive molecular testing finding and encourage the family to pursue their clinical and genetic evaluations. Below are two examples from the NYC OCME.
Case 1
An apparently previously healthy 26-year old Hispanic woman suddenly collapsed at home. Ventricular fibrillation was noted by the emergency response team. Subsequent autopsy failed to uncover structural cardiovascular disease. Post-mortem toxicology revealed elevated ethanol, cocaine and cocaine derivatives in blood. The death was signed out as an overdose due to the combined effects of cocaine and ethanol. A few months later, a cardiologist contacted OCME about this case. The decedent had been referred to him for cardiac evaluation after a prolonged QT interval was noted on a screening ECG obtained during a pre-operative assessment for umbilical hernia repair, but she was lost to follow-up after an initial physical examination and stress test. Molecular testing at the NYC OCME revealed that the decedent carried a previously reported deleterious mutation S277L in a cardiac potassium channel gene, KCNQ1, which encodes the alpha subunits of the cardiac potassium channel complex that carries the slow inward potassium current (IKs) and is responsible for myocardial repolarization. Of particular interest in the decedent is the possible role cocaine may have played in contributing to sudden cardiac death. The “repolarization reserve” model postulates that, overlapping potassium currents contribute to normal cardiac repolarization (41). Normally two potassium currents, slow (IKs) and fast (IKr), are active during the repolarization phases of the cardiac action potential. Loss of function of one current does not necessarily result in a clinical phenotype until the second current is also compromised. However, as cocaine is a known blocker of the fast potassium ion channel KCNH2 (42), diminished IKs current may have contributed to her death. The cause of death remained the acute drug intoxication, but we added the channelopathy mutation as contributory. Importantly, the decedent's two children were subsequently tested by their cardiologist, and both are carriers of this deleterious mutation. Close clinical monitoring and drug education are in place for the two children.
Case 2
A previously healthy seven-year-old Black boy went into a sudden cardiac arrest at school. At autopsy his heart appeared soft and dilated, and results from all other examinations appeared noncontributory. Molecular testing revealed that the decedent carried a previously reported Long QT syndrome mutation, Y1795C, in the SCN5A gene, which encodes the α-subunit of the cardiac sodium ion channel and is responsible for cardiac action potential initiation and propagation. This result was relayed to a cardiologist who at the time was evaluating the decedent's sister for an extremely prolonged QT interval on surface ECG. Based on this new diagnostic information, the cardiologist was able to direct costly molecular genetic testing to a single candidate gene in the sister.
Challenges in Molecular Investigations of Sudden Unexplained Death
Post-mortem molecular investigation of sudden unexplained death has unique challenges, ranging from sample collection and test indication, to test result interpretation. These problems are often very different from those faced in a clinical laboratory.
First, tissue samples collected at autopsy are traditionally preserved in formalin which often cannot be used for genetic testing. Non-formalin preservation solutions, such as RNAlater®, are more suitable and can be stored at −80°C long term. Alternatively, a dry blood card sample can be used as the DNA source. This usually requires a DNA titration study during the test validation to accommodate the low concentration DNA recovered. Because post-mortem samples need to be stored indefinitely, storage capacity, especially freezer space, becomes an issue. Other means of long-term storage of post-mortem tissue samples (DNA) are currently being explored.
Second, lack of specific test indication can be challenging. In a clinical setting, ordering a molecular test for an inheritable arrhythmia syndrome usually is triggered by clinical evidence, such as syncope, characteristic ECG findings that suggest a specific syndrome (such as a prolonged QT interval), or a specific clinical response to certain medications. In contrast, post-mortem testing of sudden unexplained death often does not have pre-existing clinical evidence to support the diagnosis. As a result, the current testing panel consisting of a limited number of genes for inherited arrhythmia syndromes will yield a low rate of positive results. Furthermore, molecular testing and interpretation of any genetic disease is complicated by genetic heterogeneity, low penetrance and variable expressivity, as well as genetic and environmental modifiers. To reduce complexity to a certain extent, well-trained medical examiners and scene investigation teams are essential to ensure that all sudden unexplained deaths are thoroughly investigated before molecular testing is ordered.
Third, interpretation of the clinical relevance of the genetic testing results may be challenging. In situations in which a previously identified disease causing mutation or a mutation which is likely to be disease causing (based on molecular characteristics) is identified, we are very comfortable attributing the cause of death to the mutation and assigning a natural manner of death. These are individuals with a negative autopsy, a negative toxicology screen, a negative medical history, and circumstances consistent with an arrhythmic death. Keep in mind that a cause of death is simply our best opinion considering all the facts of the case. No matter how the death certificate is signed, it is of the utmost importance that the medical examiner conveys the results of the molecular autopsy to the family with
recommendation for additional clinical follow-up. Interpretation of the clinical relevance of a previously unreported variant in a gene known to be associated with disease can be extremely difficult. Often there are no clinical or laboratory functional studies or additional family information of another affected relative to support the importance of the variant. Collaboration with a research laboratory on functional characterization of the defective gene products (such as in vitro electrophysiology study of a mutant ion channel function), or correlation of testing results in a living family member with clinical signs or symptoms can be very helpful to further delineate the importance of a molecular defect.
Lastly, the molecular autopsy is largely technology dependent. Current capillary electrophoresis sequencing technology is limited by low throughput, long sequencing times and relatively high costs. Over 50 genes are thought to contribute to sudden unexplained death (Table 1), and the list is growing rapidly. Next-generation or third-generation sequencing technology has dramatically increased throughput and maintained accuracy while significantly reducing costs. This new technology will eventually help medical examiners determine the precise cause of these sudden deaths. Until this “molecular autopsy” becomes widely available at a reasonable cost, it is reasonable to advise the family members of an apparent arrhythmic sudden death with a negative autopsy to follow up with their physicians and consider being tested for disorders that may predispose to sudden death.
Future Direction in Sudden Unexplained Death Investigation
Our understanding of sudden unexplained death continues to grow as the result of a multidisciplinary team approach, involving medical examiners, scene investigators, epidemiologists, molecular geneticists, and clinicians in various disciplines working together to identify possible environmental stressors and genetics risks. Such collaborative work will continue to be the theme of sudden unexplained death investigation. The “molecular autopsy” requires special medical examiner and scene investigator training and experience, modern technology, and a state-of-the-art facility. A national molecular testing and research center for sudden unexplained deaths should be considered. Such a center would allow resources to be allocated effectively and efficiently to the study of all sudden unexplained deaths in the United States.