
Abstract
This manuscript will discuss Best Practices for Death Investigation when conducting Infant Death Scene Investigations. The autopsy starts at the scene, a thorough investigation cannot be done without completing a scene recreation. During the infant death scene investigation, the Death Investigator will gather information concerning all potential causes of the sudden unexpected infant death. The Pathologist will use this information to interpret autopsy findings, and determine cause and manner of death. One goal of the death scene recreation is to be able to accurately depict the sleep environment and sleep position in which the infant was last placed down to sleep, how the infant was last known to be alive and the position the infant was found unresponsive. Another goal of the scene recreation is to be able to provide the family with an explanation of what happened to their infant. Best Practice for the Death Investigator is to follow the Centers for Disease Control and Prevention's (CDC) Sudden Unexplained Infant Death Investigation (SUIDI) Training guidelines. This includes the use of the Sudden Unexpected Infant Death reporting form. The SUIDI reporting form is an essential tool designed to standardize and improve the data collected at infant death scenes. Inaccurate classification of cause and manner of death hampers prevention efforts and researchers are unable to adequately monitor national trends, identify risk factors, or evaluate prevention programs. Valid and consistent data is needed to support research and prevention efforts if we want to reduce infant deaths.
Introduction
The State of Missouri has been nationally recognized for instituting the most comprehensive child fatality review system in the nation. Effective in 1991, Missouri legislation required each of the 114 Missouri counties and one city (St. Louis) establish a child fatality review panel (CFRP) to systematically review the death of each neonate, infant, child or teenager through 17 years of age at death (1). The CFRP program was designed to objectively study child deaths in a standardized, prescribed fashion (2). If a death meets specific criteria, the Medical Examiner/Coroner is required to refer the death to the county's CFRP. At a minimum, each CFRP includes a representative of the following county agencies:
Prosecuting Attorney
Medical Examiner/Coroner
Law Enforcement
Family/Juvenile Court
Children's Division
Emergency Medical Services
Public Health
The CFRP is not an investigative body. Each county panel exists to collect standardized data. Goals include identifying generalizable risks to life of people 17 years old and younger, and proposing prevention strategies for families and the community. The information reviewed during the CFRP meetings is confidential and meetings are closed to the general public (3, 4). However, statistical information developed by CFRPs is available to the general public via the Missouri Child Fatality Review Program Annual Report pursuant to section 210.195 of the Missouri State Statutes (2).
The Challenge of a Scene Recreation
A comprehensive scene investigation is one essential leg of a complete and thorough infant death investigation. Forensic pathologists uncommonly attend death scenes; this is the primary domain of the professional death investigator (DI). The DI is a medical examiner “extender”, contributing observational and interpretive expertise to each death investigation. Infant death investigations present particular challenges to DIs in that communication skills of a DI will influence the degree of investigative success or failure.
The death investigator (DI) must establish a rapport during his/her initial contact with the family and/or caretaker. A professional demeanor, an empathetic, non-confrontational approach, and interviewing skills are essential. The DI must pose questions in a non-accusatory tone and with neutral phrasing while maintaining sensitivity to the family and/or caretaker's grief. Acknowledge the loss and give sincere condolences. Keep in mind that individuals express emotions in various ways; anticipate a wide range of behavior and expressions of grief. The initial tone of the investigative conversation, set during first contact with the family and/or caretaker, may influence outcome of the investigation in terms of the value of information collected (6).
There were 159 sudden, unexpected infant deaths in Missouri in 2009. A scene investigation was performed in 143 cases (90%), of which 99 (69%) were performed by a medical examiner/coroner or a designated investigator (7). Following integration of scene investigation, autopsy examination, toxicology testing and records review (at a minimum), there were ten homicides (6%), 20 cases considered to represent the Sudden Infant Death Syndrome (SIDS) (13%), and 71 cases (45%) of infants who died in an unsafe sleep environment (Figure 1) (7).
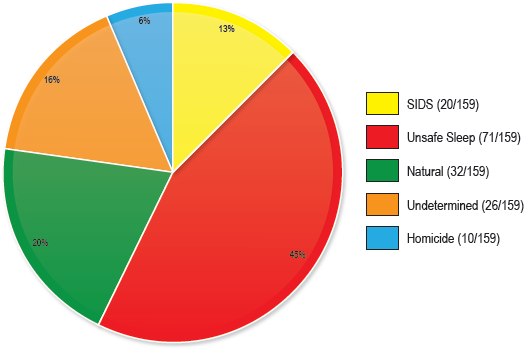
Total sudden, unexpected infant deaths less than 1 year of age in the State of Missouri in 2009.
DIs should note well that the data indicate that many sudden unexpected infant deaths are the result of one or more unsafe sleep practices; homicides are very uncommon. Therefore, while conducting the investigation, criminality should not be a default assumption. It is the DIs role to interview the family member(s) and/or witnesses, and to document the circumstances of the death; DIs do not interrogate these individuals.
Infant death scene investigations are emotionally challenging for DIs. It is highly recommended that DIs who respond to such scenes have a usable and professional support system in place and easily available.
The autopsy starts at the scene; therefore, the forensic pathologist is dependent on the DI to conduct a comprehensive death scene investigation, including a scene recreation (8). The DI must have knowledge of normal infant development to assess the credibility of the witness account of an infant's usual movements and action (9).
In sudden unexpected infant deaths lacking preliminary scene or other investigative suspicion of homicide, parents should have an opportunity to hold their infant at the scene or at the emergency room. Photographic documentation of the infant should occur prior to supervised parental holding, if logistically possible. Direct parental holding of a deceased infant should be a supervised activity (DI or a delegated individual such as a social worker or law enforcement officer). The individual supervising parental holding of their infant must understand and enforce the priorities of a death investigation to ensure that the parents do not alter the infant in any way. If keepsakes are collected for the parents, the DI should document such events in written report (10).
Suidi Reporting Form
Best practice is for DIs to adhere to the Centers for Disease Control and Prevention's (CDC) Sudden Unexplained Infant Death Investigation (SUIDI) guidelines, which includes a reporting form customized to this case type (11). The SUIDI reporting form is an essential tool designed to standardize and improve data collection at infant death scenes, and should be used in every case. The reporting form is lengthy (eight pages) and detailed, and divided into the following sections:
Investigation Data
Witness Interview
Infant Medical History
Infant Dietary History
Pregnancy History
Incident Scene Investigation
Investigation Summary
Investigation Diagrams
The last page of the SUIDI reporting form is a summary for the pathologist: a check-list of the “Top 25” critical data points most useful to the pathologist prior to autopsy (11).
It is important to follow standard interview procedures and interview witnesses separately. The DI will complete the SUIDI reporting form with the key witnesses
The data gathered using the SUIDI reporting form are essential for determining cause and manner of death and for larger epidemiologic studies. If your agency uses a scene reporting form that differs from the CDC document, a comparison to the SUIDI reporting form is recommended. Consistent use of the CDC SUIDI reporting form will yield standardized data collection over time, a death investigation strategy that optimizes interpretation of individual cases and invests in the public health value of aggregate death investigation information.
Goals and Fundamentals of a Scene Recreation
A structured, patient, sensitive infant death scene investigation provides the DI and the pathologist with data points to evaluate potential causes of the sudden unexpected infant death, which include disease, suffocation, poisoning, and blunt trauma. The DI collects and presents the scene and historical information in a predictable and standardized fashion; the pathologist uses this information, to varying degrees, to interpret autopsy and toxicology results. Final synthesis yields determination of cause and manner of death.
An infant death scene recreation is an essential component of an infant death scene investigation. Within limits of human memory and truthfulness, the DI must document and convey details of the sleep environment and the sleep position in which the infant was placed down to sleep, the position and environment in which the infant was last known to be alive, and the position and environment in which the infant was found unresponsive (8).
The scene recreation should be the final prescribed activity of an infant death scene investigation. The recreation may be a highly emotional and wrenching task for the parent(s) and/or caretaker(s). The DI should plan the interview sequence so that he/she has collected all relevant data before the recreation. The DI should conclude the interview and scene investigation shortly after completing the recreation.
The placer, the LKA and the finder are key individuals in a scene recreation - their cooperation is essential. The DI must keep in mind that the scene recreation of a recently deceased infant may be an exceptionally difficult task for these witnesses. Patience, empathy, and professionalism should guide the DIs work. Slowed speech and a softened voice are useful techniques for the DI (10). The placer, the LKA and the finder must receive a clear explanation of the value of the scene recreation to resolution of the death investigation. The DI should emphasize that to properly determine the cause and manner of death, persons with firsthand knowledge of the scene must willingly participate.
Many people are not sufficiently verbally adept to describe - precisely - describe how an infant was put down (Image 1) and how that infant was found (Image 2). Using a doll as proxy for the infant, the scene recreation is a visual and documentable illustration of the infant's position in the sleep environment (8). It is a vital tool in the DIs efforts to collect comprehensive data for later interpretation. The scene recreation should be as accurate as possible, illustrating the sleep environment in which the infant was placed down to sleep and the position in which the infant was found. The witnesses and the DI should be especially attentive to demonstrating and documenting the space around the doll's (the infant's) nose and mouth.

Placed position.

Found position.
Introduce the doll as an aid for the witness demonstration. Handle the doll with respect, but do not attempt to treat the doll as a living infant. Demonstrate the articulation of the doll's body, head, arms and legs, and explain that this allows for most accurate positioning of the doll as the witnesses recreate the placed, LKA and found positions (8).
When verifying the sleep position, use terminology the witnesses will easily understand. For example, use “back,” “belly,” or “side” rather “supine,” “prone” or “lateral”. Encourage the witnesses to ask questions. Reiterate that their cooperation assists in the establishment of both cause and manner of death.
The following distinct image sets are necessary to fully document the scene recreation:
overview
placed position
last known alive position
found position
sleep environment
The overview consists of photographically documenting the scene in general, and then specifically, the sleep environment. After doll placement by each witness, the DI photographically documents the positions from multiple perspectives. Subsequently, the DI photographically documents the bedding in a layer-by-layer fashion, and further documents all objects in the sleep environment. Any potentially hazardous products identified during the scene recreation should be referred to the United States Consumer Product Safety Commission (12).
Family Debriefing
The DI should provide the family with an overview of office procedures for investigating a sudden unexpected infant death and a timetable for release of conclusions in the form of an official report. Ensure that the family has Medical Examiner/Coroner Office contact information. Encourage the family members to ask questions and to not hesitate to call the Medical Examiner/Coroner Office with additional questions. The DI should provide the family with bereavement resources such as First Candle (13).
Summary
A goal of the CDC SUIDI training program is to standardize and enhance data collection during the investigation of every sudden unexpected infant death. A nationwide training curriculum was not available prior to the CDC SUIDI training program. Currently, while adhering to the SUIDI guidelines, the DI collects predetermined information to improve investigation of individual cases and study of aggregate data. This occurs in the setting of individual death investigations - interactions between DIs and family members and/or witnesses that are times of high emotion due to an incomprehensible sudden loss. The DI must be prepared to encounter a wide range of emotions and cooperation. The DI must remain professional and non-accusatory at all times, and demonstrate sensitivity and patience. Fundamentally, the DI should acknowledge the loss, give sincere condolences, and thank the family and other witnesses for their willing cooperation throughout the investigation.
Inaccurate and inconsistent determination of cause and manner of death in sudden unexpected infants deaths, based at least in part on variably complete investigative data, hampers research and development of education programs. Public health officials cannot adequately monitor national trends, identify risk factors, or evaluate prevention efforts. Valid and consistent data may be obtained through the CDC SUIDI program. These data are essential for meaningful research and public health education programs to reduce infant mortality. Public awareness and education are keys to reducing infant deaths. A fundamental public health message, already in use, is remarkably simple: infants sleep safest