
Abstract
The pediatric skeletal examination (PSE) is an autopsy technique recommended for pediatric cases suspicious for nonaccidental injury. The technique requires the reflection of the musculature and periosteum of the ribs, clavicles, long bones, and scapulae, and inspection of the bone surfaces and chondro-osseous interfaces. The technique is time consuming, labor intensive and possibly disfiguring. Therefore, the value of the technique must be measured against the cost.
The present study was designed to evaluate the impact of the PSE on the sensitivity of the autopsy. A non-randomized retrospective review of 94 autopsy reports was done. The cause and manner of death for each case was classified as blunt force trauma and homicide. Half of the sample received a PSE during the autopsy and half did not.
The number of rib and long bone fractures noted in the reports was significantly greater in the group that received the PSE. The number of cranial, scapular and clavicular fractures was not significantly different between the two groups. The PSE does not increase the visibility of the neurocranium; therefore, a difference in the number of cranial fractures was not expected. Scapular and clavicular fractures were rare in the study population. The insignificant difference between the two groups may be a reflection of the rarity of the fracture as opposed to the sensitivity of the PSE. The results of the study indicate that the PSE increases the sensitivity of the pediatric autopsy with respect to long bone and rib fractures.
Introduction
Child abuse cases are often the most difficult and potentially contentious cases investigated by forensic pathologists. Accurate classification of cause and manner of death is dependent on a comprehensive understanding of the medical history, scene findings, police investigation, history of the terminal events, and a complete autopsy. One component of a complete autopsy is the recognition and documentation of skeletal injury. In children, skeletal injuries, especially those considered highly suspicious for nonaccidental injury, are often occult to standard radiography and autopsy techniques (1–5). In 2009, Love and Sanchez published a new autopsy technique later termed “pediatric skeletal examination” (PSE) (6,7) that enables the prosector to directly examine the ribs, scapulae and long bones, increasing the sensitivity of the autopsy to the recognition of skeletal injuries.
The PSE involves the reflection of the musculature and periosteum overlying the ribs, clavicles, scapulae, and long bones. Once the bone is exposed, the shaft is inspected for fractures and subperiosteal new bone formation (SPNBF), and the chondro-osseous interface is inspected for irregularity or separation. If trauma is observed or suspected, the bone is removed from the body and processed to allow for gross or histological inspection (
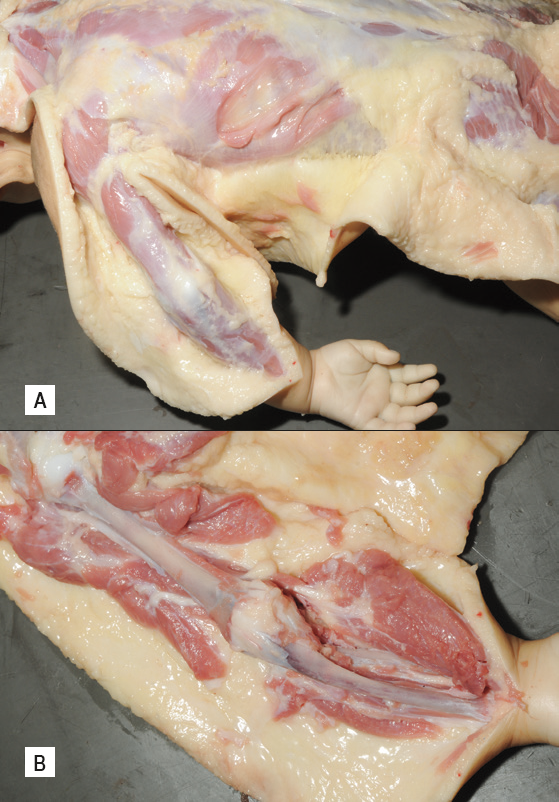
Shown are two steps of the pediatric skeletal examination (PSE).
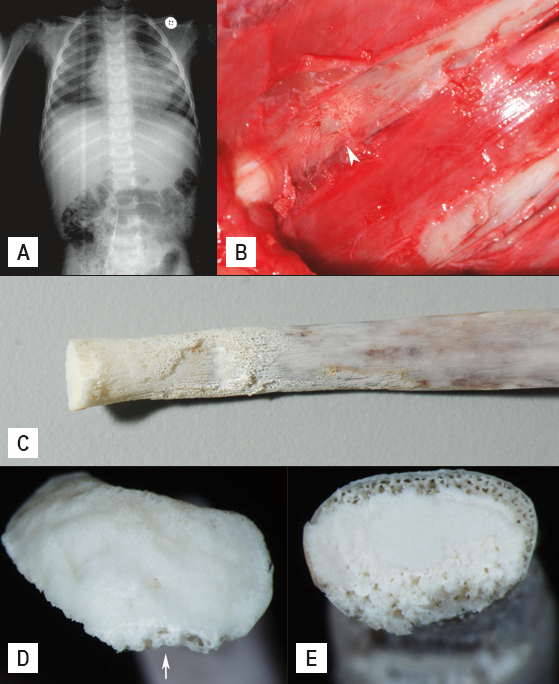
Shown are images of fractures of the right tenth rib.
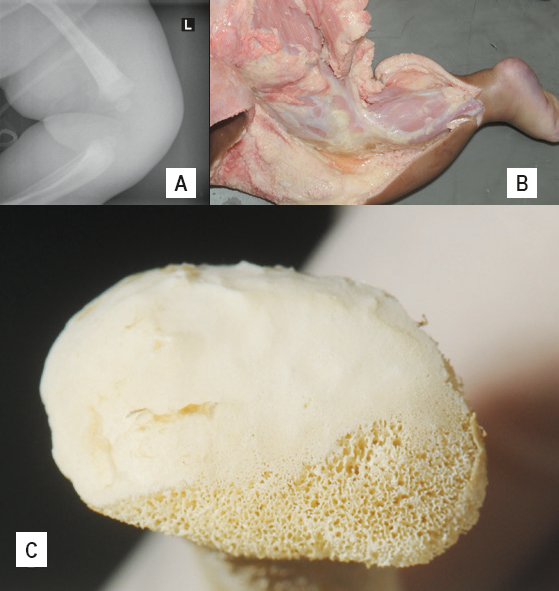
Shown are images of a classic metaphyseal lesion of left proximal tibia.
When a back dissection is performed, the PSE is done by continuing the cuts of the posterior surfaces to the long bones and scapulae. The ribs and clavicles are accessed through the standard Y-incision. This approach does not introduce any additional incisions to the body; however, removing the bones for additional examination is disfiguring. Furthermore, the procedure is time consuming and labor intensive. In light of the additional manpower requirement and alteration of the body, a cost/benefit analysis is needed. As a result, the present study was developed with the goal of measuring the impact of the PSE on the autopsy sensitivity.
Methods
A retrospective review of autopsy reports was performed. In 2007, Harris County Institute of Forensic Sciences (HCIFS) implemented the PSE as standard practice of pediatric autopsy when the pathologist had a suspicion of nonaccidental injury. All autopsy reports of pediatric decedents who received a PSE, whose cause and manner of death were classified as blunt force trauma and homicide, and who died between January 31, 2007 and July 28, 2010 were reviewed. This experimental group was matched to an equal number of decedents (control group) who did not receive a PSE and whose cause and manner of death were classified as blunt force trauma and homicide. The control group consisted of sequential autopsies progressing backward in time from September 6, 2006. The location and number of fractures documented in each autopsy report was recorded. The location of fracture was recorded as rib, cranial, long bone, clavicle, or scapula. Each fracture was counted individually; however, complex cranial fractures that included several communicating radiating fractures were counted as a single fracture. The data was statistically analyzed using Microsoft Excel.
Results
The autopsy records of 94 individuals were reviewed. Forty-seven individuals were included in the experimental and control groups, respectively. The date of death of the control group ranged from February 8, 2003 to September 6, 2006. The date of death of the experimental group ranged from January 31, 2007 to July 28, 2010. The age range of the experimental group was 1 month to 5 years (median age 12 months). The age range of the control group was 1 month to 4 years (median age 25 months) (
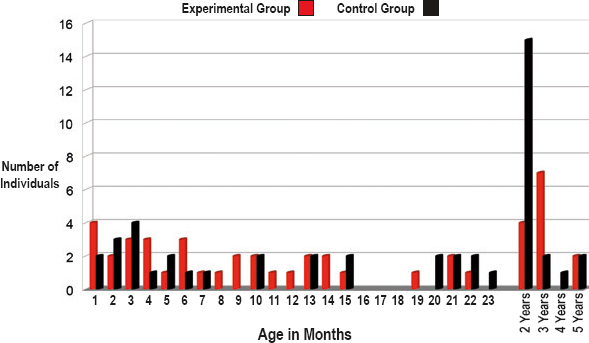
The distribution of the decedents’ age at death. Prior to two years of age, the age is stratified by months.
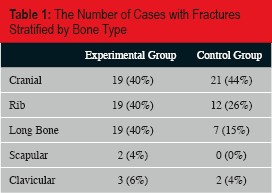
Fractures were identified in 34 (72%) of the experimental group and 30 (64%) of the control group (
The Number of Cases with Fractures Stratified by Bone Type
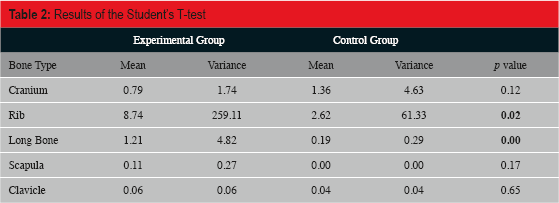
Results of the Student's T-test
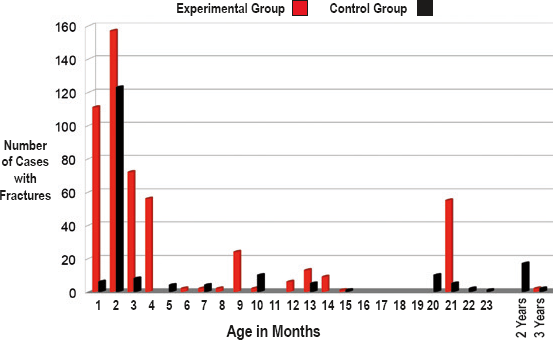
The number of cases with fractures in the experimental and control groups, stratified by age.
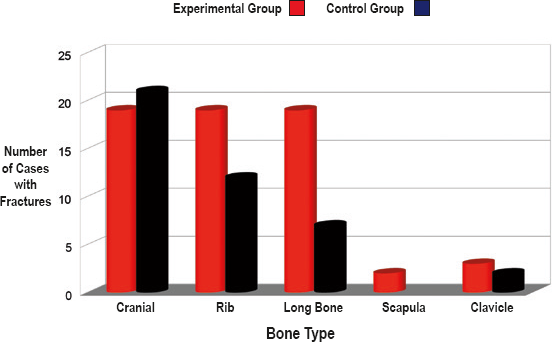
The number of cases with fractures per group, stratified by bone type.
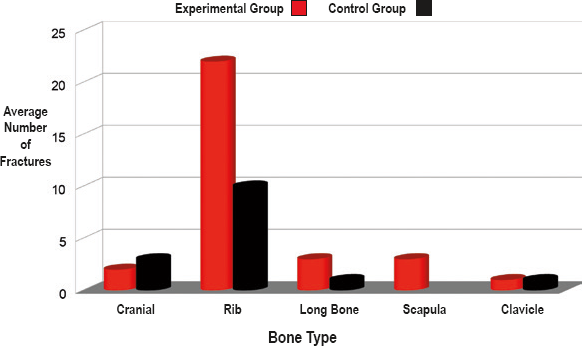
The average number of fractures per case positive for fractures, stratified by bone type.
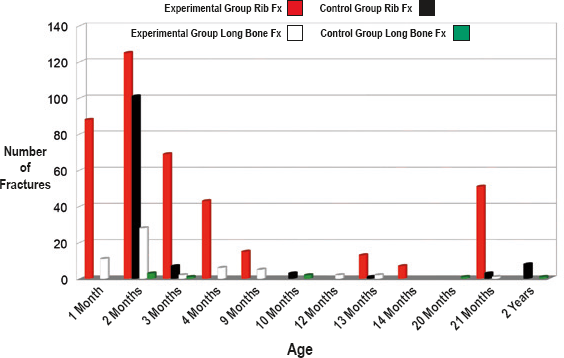
The distribution of rib and long bone fractures for the experimental and control groups, stratified by age.
Discussion
The PSE is an invasive and labor intensive evaluation. Although it does not introduce additional incisions on the skin when a back dissection is performed, removing the bones with skeletal injury for gross or histological analysis does significantly alter the body. Therefore, the value of the exam must be carefully weighed against its cost in terms of both manpower and psychosocial concerns.
The study was designed to compare two groups of cases that only varied by inclusion of the PSE during the autopsy. The study was initiated in conjunction with the adoption of the PSE as standard autopsy protocol at the HCIFS. The experimental and control groups were congregated around January 1, 2007, which was the approximate date of the PSE adoption as standard protocol. Presumptively, the deaths investigated prior to and after 2007 were similar in level and extent of blunt force. Several findings support this presumption. First, the number of cases with cranial fractures in the two groups was not significantly different. In fact, more decedents in the control group had cranial fractures (21 cases) than the experimental group (19 cases). Standard autopsy protocol fully exposes the neurocranium; therefore, no change in the frequency of cranial fractures was expected with the PSE. Second, the mean age of the two groups was not significantly different, indicating that the children were similar in size and developmental status. Finally, once the PSE was adopted as standard autopsy protocol, it was ordered in all pediatric cases suspicious for nonaccidental injury. The sources of suspicion often were inconsistencies in the initial investigation or scene presentation as well as recognition of non-therapeutic external and internal injuries during the autopsy, not the outcome of the PSE. In light of this practice, the cases that received a PSE should not have had more traumatic injuries than the cases that did not receive a PSE.
Although the mean age of the two groups was not significantly different, a potential age bias must be considered. When considering only the cases with fractures, the control group was significantly older than the experimental group. Meanwhile, more fractures were found in the younger decedents. Therefore, there is an age bias among the cases with fractures towards the experimental group. When considering only the cases with rib and long bone fractures, there is no significant difference in the mean age between the two groups; yet, there were significantly more fractures in the experimental group. Thus, there was no age bias among this subpopulation.
The significant increase in the number of long bone and rib fractures identified with the PSE supports the hypothesis that performing the PSE increases the sensitivity of the autopsy in cases suspicious for nonaccidental injury. The PSE fully exposes the ribs, long bones, clavicles and scapulae in a way that a standard autopsy does not. Furthermore, each of the decedents in the study received a radiographic skeletal survey and the images were examined by a forensic pathologist prior to the start of the autopsy. Therefore, even with a radiographic survey performed by a pathologist, the PSE increases the sensitivity of the pediatric autopsy. Surprisingly, no significant difference was found between the number of clavicular and scapular fractures between the two groups. This finding may be more a reflection of the rarity of these injuries as opposed to the sensitivity of the exam; only two cases with scapular fractures and five cases with clavicular fractures were identified in the complete study population.
Macerating soft tissue for gross examination of bones is the preferred method of fracture analysis at HCIFS and has several advantages. First, gross examination enables evaluation of the fracture biomechanics; compress and tension failure locations can be identified (9). Understanding how the bone failed allows for reconstruction of impact direction. Second, unexpected fractures are often identified after all the soft tissue is removed; this is most notable with subtle fractures of the sternal rib end and rib head (10). Gross examination of these areas, previously not examined by most pathologists, likely impacted the number of fractures recognized during the study in addition to performing the PSE. Third, gross examination ensures partial surface fractures are identified (
The impact of the PSE on the classification of the cause and manner of death was not evaluated during this study. A skeletal injury is rarely a cause of death, and the influence of a skeletal injury on the cause and manner of death classification is difficult to measure. Additionally, several of the fractures identified during the PSE were remote; further limiting the causal relationship between skeletal injury and death. Despite these limitations, the authors recommend including PSE as part of the pediatric autopsy when the case is suspicious for nonaccidental injury. Identification of all skeletal injury, acute as well as remote, is an important component of the complete autopsy.
Conclusion
In 2009, Love and Sanchez published a new autopsy technique that they recommended for pediatric cases suspicious for nonaccidental injury. The technique, named pediatric skeletal examination, is both invasive and labor intensive. This study shows that significantly more skeletal injuries are identified when a PSE is performed.
Footnotes
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest.