
Abstract
An autopsy was performed on a young child who died of blunt abdominal trauma. The parietal peritoneum exhibited focal dusky areas, which were sampled via 1) longitudinal sections of the abdominal wall and 2) preparing a cross-sectional sample of the peritoneal membrane roll. Microscopically, the membrane roll sections showed prominent neutrophilic inflammation; the longitudinal sections were comparatively more banal. We suggest that a peritoneal membrane roll might be of greater utility in the documentation of inflammation than typical longitudinal sections.
A young child was brought for autopsy after being found unresponsive by his caregivers, who stated the child had recently complained of abdominal pain. Autopsy revealed extensive blunt abdominal injuries that included: liver lacerations, bilateral diaphragmatic contusions, right renal avulsion and right adrenal hematoma. Over 500 milliliters of liquid blood was in the peritoneal cavity, and a perforation of the second portion of the duodenum was associated with a pancreatic head transection. The parietal peritoneum exhibited focal dusky areas, which were sampled via longitudinal sections of the abdominal wall. Additionally, different areas of the peritoneum, some away from the grossly discernible changes, were sampled by stripping the parietal peritoneum away from the fascia transversalis and the transversus abdominis muscles and preparing a cross-sectional sample of the peritoneal membrane roll (similar to traditional methods of sampling amniotic membranes).
Microscopically, the longitudinal sections of the abdominal wall

Longitudinal abdominal wall section (H&E, x100). Scarce inflammatory cells.
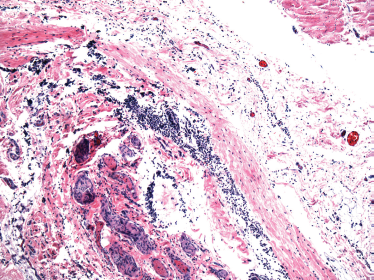
Peritoneal membrane roll (H&E, x100). Multiple, dense inflammatory foci.
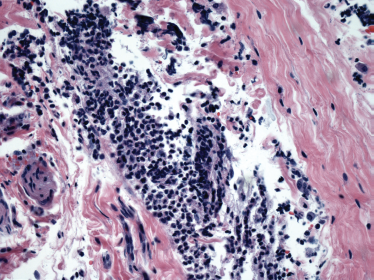
Peritoneal membrane roll (H&E, x400). Neutrophilic inflammatory infiltrates.
When looking for evidence of infection/inflammatory processes in other membranous structures (i.e., the amniotic membranes), the conventional practice is to sample the membrane by rolling it on itself and submitting transverse sections (1). This will increase the surface area to be sampled. Furthermore, there are studies that defined the correlation between the number of samples taken, and the increasing probability to identify abnormal features (2). This practice, however, has not been followed for other anatomic locations. The features seen in this case suggest that a single longitudinal section of the abdominal wall may not adequately represent the parietal peritoneum as a whole for the detection of peritonitis, which in some cases is useful to define cause-effect relations and potentially establish temporality of events leading to death that can be of paramount importance in cases of child abuse (e.g., confirmation of witness accounts).
Footnotes
The authors, reviewers, editors and publication staff do not report any relevant conflicts of interest.