
Abstract
Despite a greatly decreasing incidence of birth injuries over the past several decades with birth trauma currently accounting for less than 2% of neonatal deaths, birth trauma continues to be a significant cause of morbidity and mortality. Birth trauma is usually recognized by obstetricians and pediatricians, particularly when associated with a difficult delivery; therefore many birth injuries are diagnosed and documented in the neonatal period. Other delivery-related trauma may remain clinically silent without premortem identification. The challenge for the pathologist at autopsy is to correlate a history of birth trauma with injuries seen at autopsy, and to interpret injuries existing at death to accurately include or exclude birth trauma as a potential cause. Recognition of the spectrum of birth trauma is important when considering other accidental and nonaccidental mechanisms of injury, particularly in cases of unwitnessed perinatal death following delivery of a concealed pregnancy or in cases of alleged nonaccidental trauma. Discussed here is a general review of birth trauma that may be seen in a forensic setting to aid in interpretation of injuries that can be encountered.
INTRODUCTION
During pediatric autopsy performance, evaluation and interpretation of injuries is paramount to the determination of cause and manner of death. With ongoing controversy and a multitude of opinions surrounding pediatric head injury, the possibility of birth trauma is often invoked. The forensic pathologist must evaluate all injuries uncovered during autopsy of an infant with care given to interpret these injuries in the proper context: are they possibly related to birth trauma or is accidental or nonaccidental trauma more likely, given the age of the infant and location and extent of the injuries? As with any injury, the size and scope of birth trauma will affect the symptoms seen in the postnatal period as well as the rate of healing; many of the described birth-related injuries are symptomatic if extensive or significant, and if asymptomatic, are expected to resolve without complication.
This article provides a general review of birth trauma to aid in interpretation of injuries that may be encountered during infant autopsies. There are two recognized categories of birth injury: hypoxic-ischemic insults and mechanical trauma. Although these may coexist in an infant, the focus here will be on mechanical forces, with an emphasis on injuries likely to be seen in a forensic setting during the course of pediatric autopsy performance.
Birth injuries are a significant cause of neonatal morbidity and mortality, with frequently cited ranges from two to eight significant injuries per 1,000 live births (1, 2) and up to 25 injuries per 1,000 live births when all types of trauma, including less significant findings such as caput succedaneum, are included (3). Birth injuries accounted for 1.8% of neonatal deaths in 2002, with most years reporting a rate of less than 2% (4).
Mechanical forces including compression, traction, and torque are primarily responsible for fetal injuries sustained during childbirth; risk factors are multiple and include instrument-assisted deliveries (vacuum and forceps deliveries), vaginal breech delivery or other abnormal fetal presentation, cephalopelvic disproportion or macrosomia, prematurity, prolonged labor, and precipitous delivery (2, 5, 6). Often there exists an association with complicated or abnormal deliveries; however, injury may also occur during normal spontaneous deliveries. Additionally, although many birth injuries are symptomatic and therefore documented in medical records, injuries that can be more vexing to the forensic pathologist are those which may have been minimally symptomatic or asymptomatic in life, without diagnosis in the perinatal period.
In all infants, nonaccidental injury is the most frequent cause of injury and death, accounting for 80% of deaths under two years old attributed to traumatic brain injury (7). Therefore, special attention is given to subdural hematomas and retinal hemorrhages, as these findings position nonaccidental injury in the differential diagnosis, and in conjunction with diffuse axonal injury, comprise the traditional triad of nonaccidental trauma (NAT)/abusive head trauma.
INTRACRANIAL INJURIES
Symptomatic intracranial hemorrhage in term infants occurs in approximately 5.1 to 5.9 per 10,000 live births (8, 9). The lowest rate of intracranial hemorrhage is in infants born via cesarean delivery prior to the start of labor, and is highest in instrument-assisted deliveries. In a review of 583,340 deliveries, intracranial hemorrhage occurred in one of 1,900 spontaneous deliveries and one in 2,750 cesarean deliveries without labor; with rates of one in 860 vacuum-assisted deliveries, one in 664 forceps-assisted deliveries, and one of 256 deliveries requiring both forceps and vacuum assistance (8). Eighty-seven percent of infants with significant intracranial hemorrhage will be symptomatic within 48 hours of birth (10); apnea and seizures are the most common presenting symptoms. Additional signs of hemorrhages that may be evident in review of the medical records include indications of increased intracranial pressure (including bulging of the fontanels), lethargy, and increasing head circumference. Subtle findings may also be described, including excessive irritability, crying, and feeding problems. In one hospital-based review of intracranial injury in children under two years old (11), 19% of children were asymptomatic at presentation, all of which were infants under six months of age (14 of 19 patients) or six to 12 months of age (five of 19). None of the asymptomatic patients required surgical intervention or medical management of increased intracranial pressure, and none showed delayed neurologic deterioration at follow-up evaluation.
Subdural Hemorrhage
Subdural hematomas (SDH) are the most frequent intracranial hemorrhage related to birth trauma, in some reports comprising 73% of intracranial birth injuries (10), and ranging from 2.9 per 10,000 live births in spontaneous vaginal deliveries to ten per 10,000 live births with instrument-assisted delivery (8). The most common locations for birth-related subdural hemorrhages are posterior cerebral and infratentorial
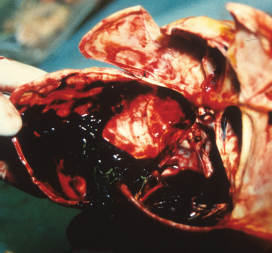
Large posterior cerebral and infratentorial subdural hemorrhage in a two-day-old infant following vacuum assisted delivery.
It was previously believed that most infants with subdural hemorrhages are symptomatic within 24 hours of birth, but symptoms may be delayed for four to five days after delivery; several radiologic studies have also shown high rates of subdural hematomas that are never symptomatic. Small subdural hemorrhages overlying the posterior cerebral convexities or below the tentorium have been documented in studies of asymptomatic newborns following uncomplicated vaginal delivery, with ranges up to 26 to 46% (12–14). As these are the most commonly cited studies documenting high rates of asymptomatic subdural hematomas, they are reviewed briefly here. Large subdural hematomas are almost uniformly diagnosed and documented at birth and therefore easier for the pathologist to interpret when findings at autopsy correlate with birth records. It is the asymptomatic and undiagnosed subdural hematomas that cause consternation for the pathologist as the possibility of rebleeding of a birth-related subdural hematoma is often postulated in arguing against the possibility of nonaccidental trauma.
A study by Rooks (12) screened 101 normal term newborns with magnetic resonance imaging (MRI), reporting subdural hematomas in 46% of infants. Newborns were imaged before 72 hours of age; all 46 infants with subdural hematomas had posterior supratentorial hemorrhages, most of which were three millimeters or less in thickness; 65% were in the posterior interhemispheric fissure and 20 (43%) also had posterior fossa subdural hematomas. In this study, a majority of the infants with subdural hematomas were spontaneous vaginal deliveries, with ten instrument-assisted deliveries and four infants born via cesarean delivery (one elective cesarean for macrosomia and three following failed trial of labor). Follow-up imaging was completed in only 18 of the 46 infants; 15 patients had resolution of subdural hemorrhage by one month of age, and all 18 showed resolution at three months of age, suggesting that subdural hematomas in infants older than three months of age are unlikely to be birth-related.
One prospective study reported an 8% prevalence of subdural hemorrhage in asymptomatic newborns using MRI, finding nine of 111 infants with subdural hematomas; all nine newborns were born vaginally at term (three with normal delivery, six with instrumentation) and were scanned within 48 hours of delivery. Six of these infants had infratentorial subdural hemorrhage, two had infratentorial and posterior supratentorial subdural hemorrhage, and one showed posterior parietal subdural hemorrhage. The subdural hematomas ranged from one to ten millimeters in thickness, with resolution of all subdural hematomas at follow-up imaging by four weeks of age (13).
A retrospective study reviewed MRIs of 88 neonates performed between one and five weeks of age, revealing 16 clinically silent subdural hematomas, seven of which also had coexisting sub-arachnoid or intraparenchymal hemorrhages; all of these subdural hemorrhages occurred in full-term infants delivered vaginally and were predominantly found in the posterior fossa or over the occipital lobe, with two cases showing temporal fossa subdural hematomas. This study was limited by its retrospective nature and limitation of MRI evaluation between one and five weeks of age, with no clinical or radiological follow up relating to the resolution of intracranial hemorrhage (14).
The subdural bleeding usually seen in birth trauma may be of dural plexus origin rather than of bridging cortical vein derivation (15, 16); in birth-related hemorrhage, the process of labor produces excessive molding of the calvarium with stretching and tearing of the superficial venous channels or venous sinuses, particularly the vascular dural folds of the posterior fossa (15). The neomembranes of organizing subdural hematomas contain neovascular channels that bleed during organization; this bleeding tends to occur within the granulation tissue without involvement of the adjacent subdural space (17). Dating of injuries, particularly those with chronic findings, can be difficult based on many factors, including time since injury, the occurrence of single versus multiple episodes of bleeding/rebleeding, and the nonspecificity of pathologic appearance after passing from the subacute to chronic phase.
Evolution of birth-related subdural hematomas that may be documented at autopsy later in the postnatal period includes persistent chronic subdural hematoma (Image 2), subdural hygroma, and hydrocephalus, which may evolve over weeks to months (18). However, as has been shown in radiologic studies, the vast majority of neonates with asymptomatic SDH recover without complications.

Flat, chronic subdural hematoma near the tentorium in a two-month-old infant.
Epidural Hemorrhage
The most uncommon form of birth-related intracranial hemorrhage, epidural hemorrhage, accounts for only 2% of intracranial birth injuries (19). Epidural hemorrhages are often associated with skull fracture or cephalohematoma (20), with sub-periosteal blood being forced into the epidural space through an underlying fracture or adjacent diastatic suture, or with shearing of the dura from the skull with excessive skull molding or instrument-assistance during delivery (21). In newborns, the middle meningeal artery is uncommonly the etiology of epidural hemorrhage as it is less susceptible to injury because the middle meningeal artery groove is not yet developed in the newborn skull (5). Until the hematoma is large, infants may not be symptomatic; infants usually present shortly after birth with seizures or hypotonia, but symptoms may be delayed, with one report of initial presentation at 15 days of age (22). Drainage of an associated cephalohematoma may result in resolution of the epidural blood as well (22, 23), however surgical drainage may be necessary (24).
Subarachnoid Hemorrhage
Subarachnoid hemorrhages range from 1.3 per 10,000 live births (spontaneous vaginal deliveries) to two or three per 10,000 live births with instrument assistance; risk factors include prematurity and hypoxia (8). Subarachnoid hemorrhages are predominantly basilar, and are often associated with intraventricular hemorrhage.
Subarachnoid hemorrhages may be asymptomatic, or may present with seizures, irritability, or depressed level of consciousness.
RETINAL HEMORRHAGES
Retinal hemorrhages are often discussed in distinguishing birth trauma from nonaccidental injury. The frequency of birth-related retinal hemorrhages ranges from 2.6 to 50% of all births, is highest in vacuum delivery, and lowest with cesarean delivery (25–27). Other associations with more severe retinal hemorrhages include fetal distress, low birth weight, and second stage of labor less than 30 minutes (28). Retinal hemorrhages related to birth are benign and self-limited in the normal neonate (27, 29); the American Academy of Ophthalmology states that intraretinal hemorrhages related to birth trauma should not persist beyond one month of age, unless hemorrhages are more extensive to include preretinal, subretinal or vitreous hemorrhages (30). Hemorrhages are described as occurring throughout the retina (
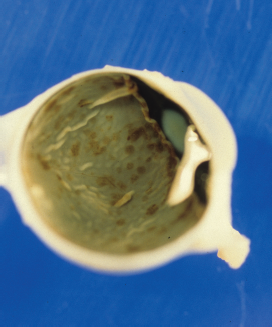
Retinal hemorrhages in a neonate following instrument-assisted delivery.
A study of 149 newborns (26) described retinal hemorrhages in 34% (50/149) of infants, with 52% (26 infants) having bilateral involvement. Hemorrhages were intraretinal in 49 of the infants, with one instance of subretinal hemorrhage in one of 298 eyes examined; hemorrhages were described as flame or dot-blot shaped but some eyes also showed confluent hemorrhages. Most hemorrhages occurred in the posterior pole, but were also documented more anteriorly in the globe. Hemorrhages were severe (grade III, designated by greater than ten hemorrhages per eye) in 54% of eyes, with grade I (one or two hemorrhages) and grade II (three to ten hemorrhages) hemorrhages in 22% and 24% of eyes, respectively; the severity of hemorrhage in one eye did not correlate with the presence or severity in the other eye. Retinal hemorrhages had disappeared by two weeks in 86% of patients for which follow-up was available (33 patients); in the remaining five infants, all initially had grade III hemorrhage with disappearance of all but the subretinal hemorrhage by four weeks after birth. This subretinal hemorrhage also had resolved at six week postnatal follow up.
A 2006 study (32) identified retinal hemorrhages in 18 of 53 neonates (34%); with the highest rates seen in vacuum delivery (77.8 %), followed by normal vaginal and forceps deliveries (30% each); retinal hemorrhages in cesarean deliveries showed a rate of 8.3%. All hemorrhages were in-traretinal, with resolution of the hemorrhages in 16 of the infants by 16 days; two infants showed residual hemorrhages when evaluated at 31 and 58 days (both vacuum-assisted deliveries).
SOFT TISSUE INJURIES
Soft tissue hemorrhages of the head, when present, are commonly documented in the birth record; at autopsy, residual evidence of their presence will depend greatly on the size of the hemorrhage and age of the infant at death.
Subgaleal Hematoma
Subgaleal hemorrhage is bleeding between the galea aponeurosis of the scalp and the periosteum; this potential space encompasses the entire scalp and therefore the resultant hematoma may cross suture lines (

Large posterior subgaleal hemorrhage in a two-day-old infant following vacuum assisted delivery.
Cephalohematoma
A cephalohematoma is a collection of blood between the periosteum and bone, arising due to shearing forces applied to the scalp during birth and occurring in 0.5 to 2.5% of all births (37, 38). Cephalohematoma is often associated with forceps or breech deliveries and is associated with skull fractures in ten to 25% of cases (39). Presenting as swelling of the scalp, often parietal or occipital, this hemorrhage does not cross suture lines (

Cephalohematoma (yellow arrows) and subgaleal hemorrhages (blue arrows) in an infant who was delivered dead via emergent cesarean section after fetal distress was observed during failed attempt at vaginal delivery.
Subcutaneous Fat Necrosis
Subcutaneous fat necrosis is not usually detected at birth; pressure in the affected areas during delivery is the most common etiology. The gross appearance is that of subcutaneous plaques which are irregular, hard and non-pitting with overlying red-purple cutaneous discoloration; calcification may also occur (40).
SKULL FRACTURES
Fractures of the skull primarily occur due to compression from forceps application or from pressure against the maternal pelvic bones. The reported incidence is approximately 3% (41); fractures are often asymptomatic.
Linear skull fractures usually affect the parietal bones and are often associated with cephalohematomas, but may also be associated with dural injury, resulting in epidural hemorrhage or subsequent development of a leptomeningeal cyst along the fracture line. Calcification and healing should be apparent by 11 days of life (42); linear fractures should heal within four to six weeks, however reports of identifiable healing lesions have been reported several months after birth (43).
Depressed skull fractures resemble an indented ping-pong ball radiographically; they likewise may be associated with dural tears and intracranial hemorrhage particularly with instrument-assisted deliveries. Although surgery is not always required in these infants, follow up monitoring or external reduction is usually well-documented in these patients and postmortem findings should be easily correlated to postnatal medical records (5).
Basilar skull fractures are exceedingly rare; fractures of the occipital bone are seldom seen with occipital osteodiastasis (separation of the synchondrosis of the squamous and lateral/condylar portions of the occipital bone). Primary risk factors for occipital osteodiastasis are breech and forceps deliveries and cephalopelvic disproportion. Separation of the synchondrosis leads to displacement of the occipital bone into the posterior fossa, resulting in occipital sinus disruption, posterior fossa hemorrhage, cerebellar contusion or laceration, or cerebellar-pulmonary embolism (44). Historically this was of greater significance and invariably fatal, with one reported incidence of 19.3 per 100 newborn infant autopsies (45), however it is much less common with current obstetric techniques, as low as 1.19 cases per 100 neonatal deaths (46). Less severe forms have also been described, with callus formation of the syn-chondrosis seen radiographically within one to two months of age in survivors (47).
NERVE INJURIES
Brachial Plexus Injury
Risk factors for brachial plexus injury include shoulder dystocia, instrumented deliveries, macrosomia, and abnormal fetal presentation (48); the injury occurs with extreme nerve stretching with lateral flexion and traction of the head. The incidence has been reported as 1.5 to 2.6 per 1,000 (1, 49). Clinical diagnosis is made by physical examination; however, associated injuries that may be identified include fractures of the clavicle or humerus, and hematomas of the sternocleidomastoid muscle (5). Long-term findings may include bony deformities, muscle atrophy, and joint contractures.
Phrenic Nerve Injury
Up to 75% of cases of phrenic nerve injury are associated with brachial plexus injury (5) and are seen under similar circumstances with excessive traction on the head and neck during delivery. Symptoms of respiratory distress usually manifest within the first day of life, but may not present until one month of age (41, 50).
Spinal Cord Injury
As in other nerve injuries, spinal cord injury is caused by excessive traction or rotation during childbirth. Damage to the spinal cord is rare, with an incidence of 0.14 in 10,000 live births. Risk factors include forceps delivery, breech presentation, hyperextension of the fetal head, precipitate delivery, and prematurity (51); upper cervical cord injuries are associated with forceps rotation during delivery and are more common than lower cervical or thoracolumbar injuries, which are associated with breech delivery (52). Because of the relative laxity of ligaments and incomplete mineralization of the vertebrae, the spinal cord can be vulnerable to injury from stretching or from vertebral dislocations (53, 54); there is rarely associated bony injury, although cervical and thoracic fractures have been infrequently reported. Spinal cord injury is often associated with hypoxic-ischemic encephalopathy, and therefore the diagnosis may be delayed (55); the prognosis is uniformly poor with a majority of patients experiencing significant disability or death, therefore this is unlikely to present as an undiagnosed injury at forensic autopsy. Pathologic changes include epidural and parenchymal hemorrhages, edema, laceration or transection of the cord, or atrophy of the cord with delayed death; the dura may occasionally be torn and associated vertebral fractures or dislocations may be seen uncommonly at autopsy (55).
LONG BONE FRACTURES
The clavicle is the most frequently fractured bone during birth, occurring in 0.3 to 2.9% of newborns, although up to 40% of these fractures are not identified until after discharge from the hospital (56). Most occur during normal deliveries, although risk factors include shoulder dystocia, high birth weight, prolonged second stage of labor, and instrumented deliveries. Associated findings may include a palpable or visible bony abnormality; healing usually occurs in seven to ten days (57).
Long bone fractures are uncommon, ranging from 0.05 to 0.13 per 1,000 live births (58); risk factors include breech presentation, low birth weight and cesarean delivery (59). Occasionally the diagnosis is not made on initial postnatal exam; however symptoms include pain, swelling, crepitus, and decreased movement of the affected limb. If the fracture involves separation of the epiphysis, it may not be evident radiographically due to non-ossification of the epiphyses. Callus formation will be seen in approximately seven to 12 days, with remodeling with recovery typically expected in two to six weeks (60).
Rib fractures can also occur during birth although they are sporadically documented in the literature often as isolated case reports; one study of bone injuries in 34,946 live born neonates revealed no rib fractures (61), and a survey of 39 infants less than 12 months of age with diagnosed rib fractures found only one case attributable to delivery trauma (62). Rib fractures are correlated with high birth weight and difficult deliveries, including instrument-assisted deliveries, and when present, are often associated with shoulder dystocia, clavicular fracture, or brachial plexus injury. In a summary of 13 reported cases in the literature, fractures primarily involve the mid-posterior ribs (singly or in succession on a single side), rather than the more medial paraverterbral location often described with NAT, with involvement of the ipsilateral clavicle when clavicle fracture is also present (63). Affected infants may present with respiratory distress or crepitus; none of the reported cases had associated thoracic solid organ injury.
INTRA-ABDOMINAL INJURIES
Intra-abdominal injuries are rare and manifest as lacerations or subcapsular hematomas of the liver or spleen, or adrenal hemorrhages, with liver injuries being the most common (64). Mechanisms include direct trauma to the abdomen, compression of the chest against the surface of the liver or spleen, or torso compression with tearing of the peritoneal support ligaments of the liver or spleen (65, 66). Presentation is variable, depending on the amount and rapidity of blood loss; signs and symptoms may be delayed with insidious loss of blood into the subcapsular space of the liver or spleen, with acute decline following rupture. Discovery of abdominal hemorrhage at autopsy within the postnatal period requires careful evaluation of the age of the injury, presence of inflammation and hematoma organization, and review of the postnatal records for insidious signs and symptoms including anemia, poor feeding, tachypnea and tachycardia, or the presence of an abdominal or flank mass.
DISCUSSION
Many studies of birth injury are clinical or radiographic, as is necessary to evaluate healing and resolution of injuries in a living child. Pathologic studies are much more difficult if not impossible to perform, particularly in a prospective manner, as most children with birth related injuries do not die, and the discovery of injury at autopsy is rarely able to be traced to previously documented birth injury.
Birth injuries are frequently encountered by clinicians in obstetrics and pediatrics, and are less frequently observed by the forensic pathologist. Review of the medical records, to include birth history, is critical in any pediatric autopsy, however because signs and symptoms of some injuries might be masked by other clinical problems or may be clinically silent immediately after birth, there may be no documented record of birth trauma in the child's history. It is important to recognize the spectrum of injuries that are commonly described as birth trauma, particularly in a forensic setting where other accidental and nonaccidental mechanisms of injury must be considered.
The presence of fatal injuries in infants, particularly head injuries, indicate trauma in a majority of cases; the challenge is interpreting the injuries in the context of each individual case, with attention paid to the constellation of findings and the acuity or chronicity of injuries, and with chronic findings, attributing those findings to innocuous birth trauma or a more significant postnatal traumatic event such as nonaccidental trauma. In evaluating injuries discovered at autopsy and deciding if birth trauma may play a role, consider that if birth injury is major, then it is most commonly symptomatic and documented, while most asymptomatic injuries are clinically insignificant and typically resolve over a short timeframe.
Footnotes
The author, reviewers, editors, and publication staff do not report any relevant conflicts of interest.