
Abstract
Elder mistreatment (EM) and elder self-neglect (SN) are risk factors for mortality. Medical examiners (ME) seldom investigate EM and SN as potential influences of death in older adults. Recognizing forensic markers associated with EM and/or SN may lead to further investigation into EM and SN as potential contributors and thus, may impact the cause and manner of death.
Methods
One-hundred and ninety-two Adult Protective Services (APS)-substantiated EM and SN cases 65 years of age and older, residing in Houston, Texas in Harris County with ME records were matched on age, race, gender and socio-economic status to individuals with ME records and no APS history. A conditional logistic regression was conducted to identify variables that reliably predict ME cases with an APS history.
Results
APS cases had significantly higher odds of having a history of pressure sores (OR: 2.4; 95% CI = 1.2 – 4.9), but had significantly lower odds of presenting with abnormally high body mass indexes (OR: 0.5; 95% CI = 0.3 – 0.9).
Conclusion
These data suggest that forensic case information such as a decedent history of pressure sores may indicate a past history of elder mistreatment or self-neglect. In contrast, having an abnormally high body mass index may indicate a lack of APS history. More studies are needed to better define these predictors and to identify other predictors that may assist forensic pathologists in identifying deaths in older adults that may have been impacted by EM and/or SN.
Introduction
Older adults often have fewer support systems and reduced physical, psychological and economic reserves. These reserves play an important role in adequately responding to environmental and social conditions that may negatively impact their health and well-being (1). Such instances include elder mistreatment (EM) and self-neglect (SN), both of which have been linked to significantly higher mortality rates among older adults (2, 3). Despite being independent risk factors for higher mortality, EM and SN are very seldom identified by forensic pathologists as contributing to the deaths in older decedents (4).
It has been estimated that one to two million older adults experience EM and SN annually (3). EM consists of financial exploitation, caregiverneglect, physical abuse, sexual abuse and psychological abuse and is defined by the National Center on Elder Abuse as “any intentional act against an older adult that results in harm or loss of personal property” (5). SN is very similar to caregiver-neglect, but occurs in the absence of a perpetrator and is defined as the inability or unwillingness of an individual to provide oneself with the necessary resources to live safely and independently (6). The two prominent mortality studies have reported three to six-fold increases in mortality rates among older adults who experience EM and SN compared to demographically matched controls with no history of abuse or neglect (2, 3).
Despite the high numbers of persons impacted by EM and SN, and the increased mortality, evidence suggests that many forensic pathologists are not fully aware of EM or SN circumstances that may surround the individual's death (4). This may be reflective of a general trend towards not performing autopsies on the elderly (7, 8), limited social and historical information surrounding a death with strict reliance on medical history and/or the difficulty identifying subtle forensic markers of elder abuse (1, 9, 10). National experts agree on the need to identify useful forensic markers which could assist forensic pathologists in differentiating EM and/or SN from the common maladies seen in old age. The evidence in studies aimed at identifying markers of EM and SN in older adults remains inconclusive (1). As the aging population grows nationally and the prevalence of EM and SN increases, forensic pathologists will undoubtedly investigate more and more cases in which EM and/or SN were at least proximally involved.
This study provides an exploratory case/comparison analysis of older adult deaths with and without histories of EM and/or SN. The purpose is to determine if specific forensic markers and circumstances at death, encountered during postmortem examinations, can be used to indicate an increased likelihood that the older decedent had a prior substantiated history of EM and/or SN. Identifying such markers could prompt forensic pathologists to inquire into the potential role that EM and/or SN had in the cause of death and therefore affect the cause and manner of death determination. To do so, this study combines data from the Texas Department of Family and Protective Services, Division of Adult Protective Services (APS) and postmortem examination records from the medical examiner's office of a large and diverse metropolitan area in Texas. It is the first study to identify forensic markers to predict a history of elder mistreatment or self-neglect using data from medical examiners. The findings and their implications for law, forensic pathology, policy and future research are discussed.
Methods
Sample
This study includes 384 adults 65 years of age and older who underwent postmortem examination by the Harris County Institute of Forensic Sciences (HCIFS) in Houston, Texas. All postmortem examinations occurred between the dates of January 1, 2004 and December 31, 2008. One-hundred and ninety-two participants, (50%) of the sample, also had a Texas APS region VI substantiated history of EM and/or SN within the study period. A group of 192 older adults without an APS region VI substantiated history of abuse and/or neglect during the study period was selected from the HCIFS database for comparison on parameters of interest. One to one matching of case and comparison was performed using age, race, gender and socioeconomic status.
Data Sources
Texas APS
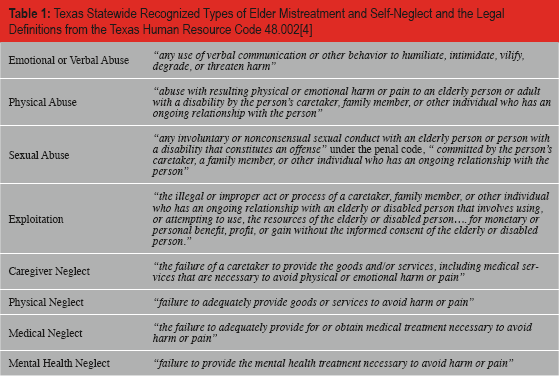
APS agencies nationwide are charged with responding to reports of domestic EM and SN. Incidents are reported from community agencies, healthcare providers, family, friends, neighbors and victims themselves. Once a report is filed, an investigation must be initiated within 24 to 72 hours. APS workers conduct in-home investigations and deem a case valid, invalid, or unable to be determined based on the findings of the Client Assessment and Risk Evaluation (CARE) tool and other available information collected during the investigation. The Texas Human Resource Code 48.002[4] defines the different types of elder mistreatment and self-neglect recognized by Texas APS agencies (5).
Texas Statewide Recognized Types of Elder Mistreatment and Self-Neglect and the Legal Definitions from the Texas Human Resource Code 48.002[4]
In Texas, APS is divided into 11 regions to respond to these reports. APS region VI is the second largest region in the state and serves Harris County and surrounding counties. The APS data used in this study included individuals 65 years of age and older with region VI substantiated EM and SN in Harris County between dates of January 1, 2004 and December 31, 2008. Between these dates, the county substantiated 10,280 cases of EM and SN in adults 65 years of age and older.
Harris County Institute of Forensic Sciences (HCIFS)
HCIFS is the county agency charged with medicolegal death investigation in Harris County, Texas, and operates according to Chapter 49.25 of the Texas Code of Criminal Justice. The department seeks to determine the cause and manner of unattended or unusual deaths in Harris County and 15 surrounding counties, and provides forensic analytical support to over 60 agencies. The office provides unbiased medical testimony in murder cases, informs law enforcement agencies in accident, suicide and homicide investigations, conducts pretrial conferences for assistant district attorneys, presents seminars for grand jurors, alerts city and county health departments of potential communicable or contagious diseases, and creates death certificates. Between January 1, 2004 and December 31, 2008 the HCIFS completed physical exams and/or autopsies on 4403 deaths in Harris County for adults 65 years of age and older.
Linking APS and HCIFS Databases
The APS and HCIFS datasets were linked using Link King v9.1.2 to provide systematic and accurate cross-matching results. Link-King uses deterministic and probabilistic algorithms to locate potential matches between two independent datasets (11–15). The primary variables used to match individuals across the datasets were race, gender, date of birth, and first and last name. Zip code was used as an additional matching variable to improve accuracy with no penalty for non-matches. In order to maximize the data matching process, matches with low and medium matching likelihoods were manually reviewed for potential inclusion.
Data Abstraction
The variables chosen for abstraction were identified prior to the study by elder abuse experts and forensic pathologists. The variables were chosen based on both empirical data and anecdotal experiences.
Study Variables Abstracted from the HCIFS Records*
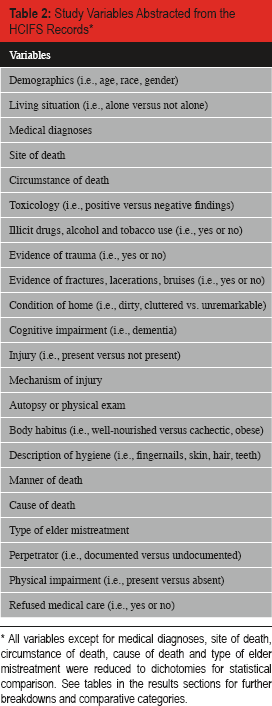
All variables except for medical diagnoses, site of death, circumstance of death, cause of death and type of elder mistreatment were reduced to dichotomies for statistical comparison. See tables in the results sections for further breakdowns and comparative categories.
Analytic Strategy
This analysis was designed to identify forensic markers associated with prior EM and/or SN among medical examiner cases 65 years of age and older. One to one matching of case and controls was performed based on age, race, gender and socioeconomic status. Cases were defined as medical examiner cases with a history of EM and/or SN within the sampling frame (January 1, 2004 through December 31, 2008) and comparisons were defined as those with no documented history during this time.
Descriptive statistics were used to characterize the data using means, standard deviations, and percentages. Paired t-tests and McNemar's chisquare, which control for the matching design, were used to assess for bivariate statistical differences between groups (16). Multivariable modeling to predict case-control status was performed using conditional logistic regression (17) in STATA 12 (Stata Corp, College Station). Two separate criteria were used to determine covariate inclusion in the model: 1) less than 10% missing data and 2) bivariate associations meeting the conventional statistical significance (p < 0.05). All variables meeting these criteria were entered simultaneously into a single predictive model. All dichotomous variables were dummy coded with values of 0 (not present) and 1 (present). Body Mass Index (BMI) was calculated by dividing weight in pounds by height in inches squared and multiplying that number by a constant equal to 703. This continuous value was reduced into scientifically plausible categories. Specifically, BMI was reduced into low abnormal (BMI <19), normal (BMI = 19–24), and high abnormal (BMI >25). Normal BMI was the reference group. The dependent variable (Case vs. Control) was coded as 0 indicating controls and 1 indicating cases. Odds ratios (OR), 95% confidence intervals (CI) and associated Wald statistics were evaluated to determine variable significance in the model. The Mantel-Haenzel method was used to derive adjusted odds ratios for the different model covariates. Conventional p-values of <0.05 were used for Z-scores and odds ratios that did not include 1 were considered significant.
Sample Size
Given the matched-design study the outcome of case versus control was equally likely in the presence of no covariates. Studies suggest dividing the dependent outcome, with the lowest presence, by the number of covariates in the model to determine the sufficiency of the covariate to outcome ratio. A 10 to 1 ratio is considered adequate (17). In the present study both outcome conditions had n=192. The ratio of covariates to outcomes was 38 and thus, is considered to provide adequate power for the model. Model assumptions pertaining to covariate linearity do not apply to models with discrete covariates and outcomes therefore no model assumptions tests were conducted.
Results
Sample Characteristics of N=384 Adults 65 Years of Age and Older With Postmortem Medical Examiner Records With and Without a Confirmed History of Adult Protective Services (APS) and Harris County Institute of Forensic Sciences (HCIFS) Validated Elder Mistreatment and/or Self-Neglect*
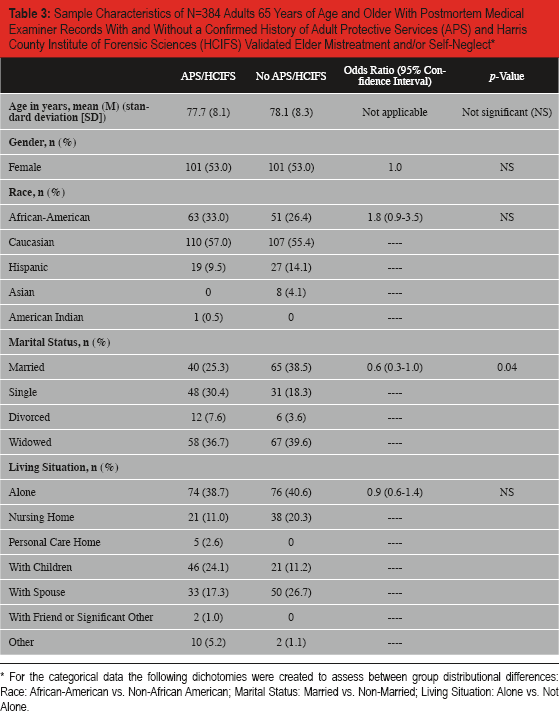
For the categorical data the following dichotomies were created to assess between group distributional differences: Race: African-American vs. Non-African American; Marital Status: Married vs. Non-Married; Living Situation: Alone vs. Not Alone.
The data showed that 65% of the APS cases had a single substantiated allegation. Of those, 92% were for physical neglect (n=101), mental health neglect (n=4), and medical neglect (n=12). Only 35% of the sample had multiple allegations with the combination of physical and medical neglect showing up 63% of the time.
Results of the bivariate associations for the remaining variables can be found in
Differences in Body Composition and Medical Examiner Investigations Between N=384 Adults 65 Years of Age and Older With and Without a History of Adult Protective Services (APS) and Harris County Institute of Forensic Sciences (HCIFS) Substantiated Elder Mistreatment and/or Self-Neglect
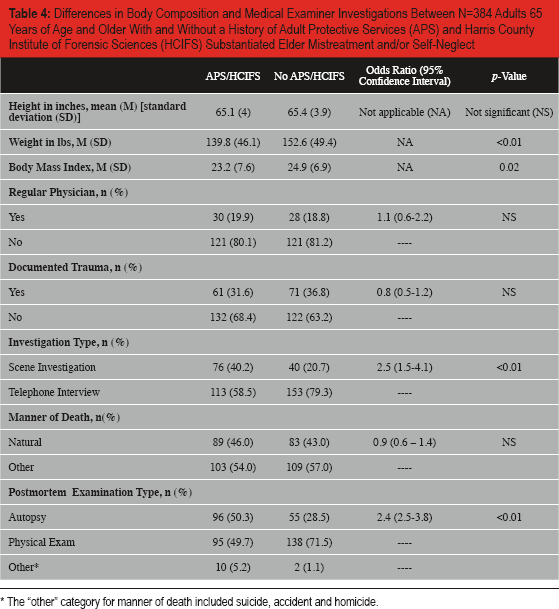
The “other” category for manner of death included suicide, accident and homicide.
Differences in Decubitus Ulcers and Hygiene Documented in Medical Examiner Records Between N=384 Adults 65 Years of Age and Older With and Without a History of Adult Protective Services (APS) and Harris County Institute of Forensic Sciences (HCIFS) Substantiated Elder Mistreatment and/or Self-Neglect
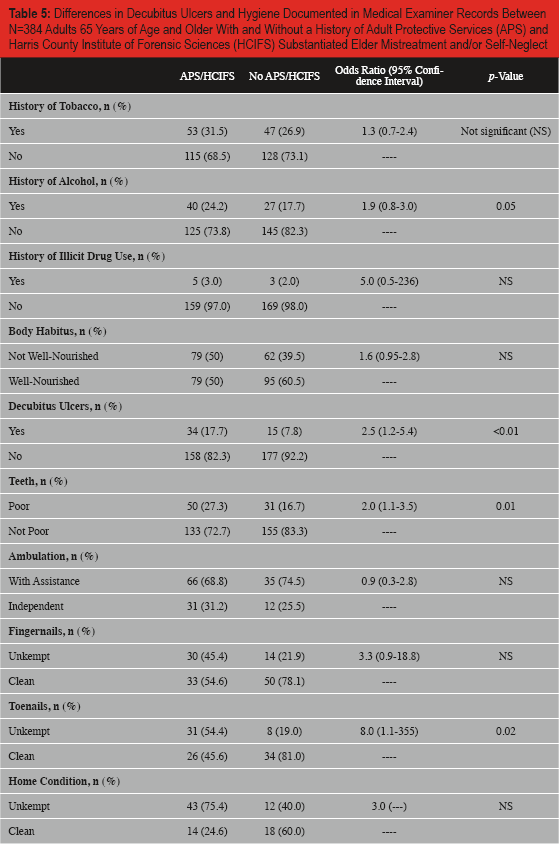
Conditional logistic regression was used to predict the probability of APS history based on covariates meeting the inclusion criteria. The variables included in the final model were BMI categories, dentition, and a history/presence of pressure sores. Past history of alcohol use, toenail hygiene, marital status, and external appearance also exhibited bivariate significance, but had missing data percentages ranging from 15% to 70%. Including these variables reduced the sample size considerably which negatively affected the precision of the estimates and the convergence of the model. Likewise, scene investigation and postmortem examination type met bivariate statistical significance, but were not included in the model because they reflect policy-based decisions and thus, are not generalizable. The full predictive model including 95% confidence intervals is provided in
Conditional Logistic Regression Model Predicting a History of Adult Protective Services Elder Mistreatment and/or Self-Neglect Among N=384 Medical Examiner Cases
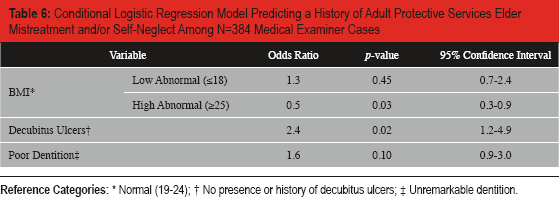
Normal (19–24);
No presence or history of decubitus ulcers;
Unremarkable dentition.
Discussion
Despite data reporting a marked increase in mortality associated with elder mistreatment and self-neglect (2, 3), forensic pathologists often are not aware of such neglect prior to classifying the cause and manner of death (4). In cases of EM, this limits the ability of law enforcement to prosecute offenders. Increased recognition of EM or SN by the forensic pathologist may inform the cause and manner of death and lead to the design of better prevention and intervention programs.
The purpose of this exploratory study was to identify specific markers and circumstances, which when encountered during postmortem examinations, may lead forensic pathologists to suspect a relatively recent history of EM and/or SN associated with the decedent. The identification of these markers could allude to EM and/or SN as potential contributors to the decedent's death. Because EM and SN are broad categories, they are not expected to stand-alone as diagnoses on death certificates, but substantiating their role in an older decedent's death may influence the cause and manner of death determination. For instance, within the EM category it would primarily be physical abuse or caregiver neglect that may influence a case to be anything other than natural in manner.
This study found two physical markers that provide reliable predictions of APS-substantiated EM and SN at least five years prior to the decedents death. The final variables retained in the conditional logistic regression were BMI and history/presence of decubitus ulcers. The results indicate that APS cases are less likely to have abnormally high BMIs, but are more likely to have a history/presence of decubitus ulcers. Although these data are preliminary, the identification of these indicators is a good practice and provides the medicolegal death investigation with potential information needed to make more informed determination of cause and manner of death. Accordingly, these exploratory findings could have potentially important implications for forensic pathology, law and public health.
Aside from obvious signs of trauma and neglect, it remains difficult for forensic pathologists to differentiate deaths resulting from common age-related diseases and the sometimes subtle effects of EM and/or SN. EM and SN experts suggest that even non-physical trauma such as psychological abuse, experienced by older adults with diminished reserves, can result in a cascade of negative events including death. Identification of such impact on the life of the elderly becomes very difficult to discern by the forensic pathologist. This may be the reason why Kim et al. found that forensic pathologists, in a large metropolitan area with high rates of EM and SN reports, very rarely attributed EM and/or SN as contributing to the cause and manner of death among older decedents (4). The current study provides preliminary support for physical findings that may serve as indicators for forensic pathologists to inquire about the potential for EM and/or SN to be involved. Low body mass index scores and past or present pressures sores both may indicate neglect. As the forensic pathology community becomes more aware of the markers of EM and SN, there may be a shift in how those cases with well documented EM and SN are classified.
The current study findings are consistent with cases often brought to the investigation of elder abuse fatality review teams. For instance, the following case study provides a brief glimpse into an EM case that impacted the death of an older adult. Briefly, a 79-year-old African-American female was transported from her home to a local hospital where she passed away two days later. She had a formal care-provider. Her external appearance was described as cachectic. Her body mass index was calculated to be 16. She was edentulous, with ecchymosis in multiple bodily areas. She has numerous decubitus ulcers on her back, sacral region, buttocks and lower extremities. There were no noted injuries and her cause of death was identified as complications from hypertensive cardiovascular disease and her contributing cause of death was chronic obstructive pulmonary disease. In this case, caregiver neglect was substantiated and prosecution followed.
More research on the physical markers identified in the current study is needed to ensure their utility as predictors of past EM and/or SN. For instance, the association between body weight and body mass index in the current study remains unclear regarding their practicality as markers for predicting past APS history. Although APS cases, on average, had lower body weights and BMIs, their weights and BMIs were within the normal range. Moreover, the data only showed that APS cases were significantly less likely to present with abnormally high BMIs. Therefore, this finding predicts the absence of APS history. Although this is useful in helping rule out EM and SN it does not help predict positive cases of EM and SN. Nevertheless, the finding that for APS cases to present with body weights that were on average 12 lbs lower than non-cases, we believe represents a trend towards cases of EM and SN and thus, forensic pathologists should be prompted to consider APS history in older decedent cases where body weight and BMI deviate from the age related norm. That said, further research is needed to determine the best BMI value or ranges that provide forensic pathologists with more sensitive and specific predictions of APS history in older decedents.
If further research provides support for the markers identified in this study, these markers may be valuably incorporated into the routine postmortem assessments of older adults, by forensic pathologists, as screening items to determine whether further investigation of EM and/or SN is appropriate. In the cases of EM, the investigation findings and the use of these markers may lead to the classification of homicide or undetermined in cases that would otherwise be classified as natural; allowing law enforcement the opportunity for proper investigation. In the case of SN, information can be made available to the public health sector for the purpose of informing prevention programs and policy.
The current findings should be considered in light of several limitations. First, this was a secondary data analysis using data not systematically collected for scientific purposes. Therefore, some of the potentially important variables were unable to be included in the predictive model due to missing data which greatly reduced sample size. It is unclear whether including these variables would have attenuated some of the obtained associations. Second, although the sample sizes for each group were not considered small, there were several variables with very little variance for the dichotomous responses. This reduced the precision of the model parameter estimates. Future research to determine forensic markers may be better served by investigating more homogeneous populations of APS cases. Third, the data were limited to Harris County and thus may not be widely representative and generalizable. Fourth, we used a time frame of five years and thus, the period between APS substantiation and the time of death may have mitigated some of the associations. Like all new studies, these findings warrant replication.
This was the first study to identify forensic markers capable of predicting a history of EM and/ or SN among older decedents receiving medical examiner reviews. With the abundance of older adults who die each day it would be too burdensome for the medical examiner to inquire about APS involvement on every case before deciding whether or not to release jurisdiction. The findings from this exploratory study suggest that information gathered during the postmortem examinations (i.e., BMI and history and/or presence of decubitus ulcers) could be used to determine whether cases need further investigation regarding the potential involvement of abuse and/or neglect among older decedents. Knowing that certain forensic markers can help predict APS history is a beginning for perhaps developing checklists within the medical examiner system for inquiry for select cases.
However, before we can determine the full utility of the markers identified in this study, more data on known cases are needed for designing randomized studies. We need to better understand how different variables may stand alone and also interact with other variables to improve the prediction of older death cases with prior APS history. The future development of investigative tools based on forensic markers of EM and SN has the potential to advance prosecution of offenders as well as design effective intervention and prevention programs.
Footnotes
Acknowledgements
The authors would like to thank the Texas Department of Family and Protective Services, Division of Adult Protective Services, and the Harris County Institute of Forensic Sciences for providing the data used in this manuscript.
Research was funded by the Borchard Foundation Center on Law and Aging.
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest.