
Abstract
Having served as a board-certified forensic pathologist in the southern tier of New York for over 23 years, the author has received cases from over a dozen rural New York State coroner counties. While some coroners are physicians, none of them is a pathologist, and most are not in the medical profession. Some are appointed by their county legislature, whereas others are elected. Levels of coroner training and experience in death investigation, terms of office, multiple coroners per county, and turnover of coroner staff are all challenges for the consultant forensic pathologist. Functioning as an autonomous independent contractor, a forensic pathologist can bring standardization, medical knowledge, and reliability to the determination of cause, mechanism, and manner of death, even when resources are less than optimal. As fewer hospital pathologists perform autopsies, and as community hospitals opt to close their morgues entirely, regional centers emerge to absorb the workload. In such a setting, the forensic pathologist must establish a working relationship with an institution such as a regional hospital to support an adequate physical plant for an autopsy service. Until such time as adequate manpower and financial resources are available, a coroner-based death investigation system is still a necessary complement to the medical examiner system in New York State. There are both drawbacks and advantages to such a practice for the independent forensic pathologist. Yet the citizens of this area of New York State are served by a death investigation system that is functional and meets basic needs.
Keywords
Introduction
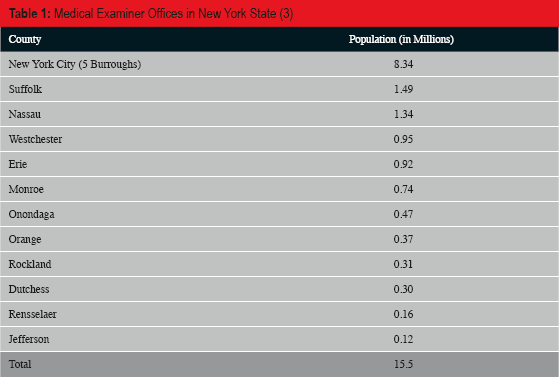
In spite of the existence of numerous well-established, fully functioning medical examiner systems, a sizeable proportion of the U.S. population is serviced by coroner systems (1, 2). In New York State, where twelve county medical examiner offices exist in the 62 counties (
Medical Examiner Offices in New York State (3)
Methods
Data are derived from the U.S. Census Bureau, and individual County Medical Examiner web sites, and the author's 23 years of experience of working with the coroners of multiple counties which often have more than one coroner per county, a unique situation in the United States except for Texas, in which multiple justices of the peace fulfill coroner duties in some counties (4, 5).
Discussion
Metropolitan areas in New York State account for the vast majority of the population of 19.6 million individuals. The five boroughs of New York City alone hold over 8.3 million people (3). Although we are fortunate to have one of the oldest, largest and most comprehensive of the death investigation systems in the world at the Office of the Chief Medical Examiner in New York City, as well as several medical examiner offices in cities including Buffalo, Rochester, and Syracuse, and in the counties near New York City (Westchester, Nassau, Suffolk, Dutchess, Rockland, Orange), many legal authorities call upon county coroners and local resources to examine deaths in their communities. This hybrid system of medical examiner offices and coroner offices allows for adaptation to population density in the state, while creating differences in practice patterns for pathologists.
Having served as a board-certified forensic pathologist in the southern tier of New York for over 23 years, the author has received cases from over a dozen rural New York State counties and routinely from eight such counties (
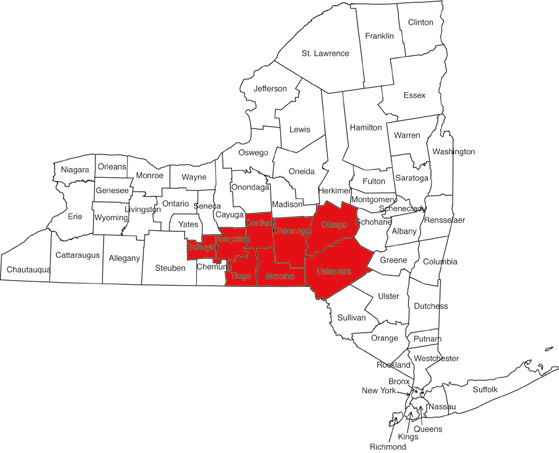
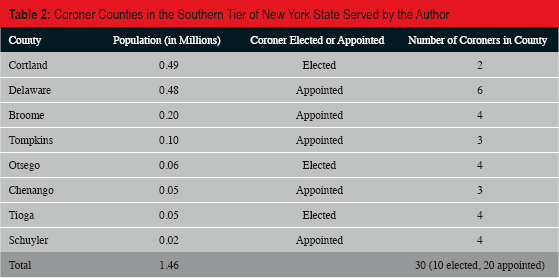
New York counties served by the author, as listed in Table 2
Coroner Counties in the Southern Tier of New York State Served by the Author
Presently, New York State has no requirement for coroner training. We are fortunate to have a non-profit organization, the New York State Association of County Coroners and Medical Examiners (NYSACCME), that provides introductory and continuing education meetings twice each year at venues throughout upstate New York. Many of the coroners who take advantage of the training offered through NYSACCME do so voluntarily, on their own time, and at their own expense. Levels of coroner training and experience in death investigation, terms of office, multiple coroners per county, and turnover of coroner staff are all challenges for the consultant forensic pathologist. Death certification is ultimately the coroner's responsibility, and usually incorporates the autopsy findings correctly, although the precise verbiage is often out of the forensic pathologist's control. Neither is there any legal requirement to collate death statistics for the betterment of society.
Functioning as an autonomous independent contractor, a forensic pathologist can bring standardization, medical knowledge, and reliability to the determination of cause, mechanism, and manner of death, even when resources are less than optimal. As fewer hospital pathologists perform autopsies, and as community hospitals opt to close their morgues entirely, regional centers emerge to absorb the workload. In such a setting, the forensic pathologist must establish a working relationship with an institution such as a regional hospital to support an adequate physical plant for an autopsy service. Individual rural counties are unlikely to build free-standing offices akin to those in larger population centers.
Issues distinguishing a medical examiner's office from a coroner's office are numerous. Perhaps the most obvious issue is the lack of trained medical investigators. Since an independent forensic pathologist is likely to have other duties, such as hospital-based surgical pathology, he or she will not often attend the scene of death, but will depend on the coroner and/or law enforcement for information about the scene. Trained forensic photographers are not always available, whether at the scene or in the morgue. Although New York State requires that a coroner attend the scene of death, that is simply not always possible, leaving the forensic pathologist with fragmentary information about circumstances surrounding the death. Hence, building a trusting relationship with local, county and state law enforcement personnel is vital in order to reach accurate conclusions about a death.
Support services for performance of autopsies are also problematic in the independent setting. Qualified autopsy technicians/assistants are hard to find or require on-the-job training, and may not stay on the job for long. Clerical support is often shared with other regular inpatient pathology services, which may take priority. Transportation of decedents depends primarily on funeral directors rather than on a dedicated vehicle. Delays in transportation can lead to tissue preservation issues and difficulty in determining an accurate time of death. Forensic toxicology in the rural setting depends on a local hospital chemistry laboratory or on a commercial reference laboratory in most cases, although the New York State Police Department has a forensic laboratory that is available for high profile cases such as homicides. Another unfortunate byproduct of independent practice in a low volume rural area is lack of coverage for the forensic pathologist during vacations and illnesses, a situation which may necessitate long-range transport of homicide cases to overburdened offices, or the performance of potentially litigation-bound cases by a non-forensic hospital pathologist. Research and publication about forensic cases and statistics are not the primary roles of the independent service-oriented forensic pathologist, although they are not out of the question.
In the southern tier of New York State, some 440 complete autopsies are performed each year at two morgues within hospitals in Binghamton (Broome County). Approximately 95% of the autopsies are coroner cases, as opposed to natural in-hospital death cases. Of those autopsies, 80–100 are performed by the author himself, including virtually all of the homicides (6–12/year) and almost all of the infants and children. Partial autopsies and external exams are discouraged, in order to obviate the lack of control over medical investigation. Communication between coroners and attending physicians varies by coroner, such that unattended natural deaths may eventuate in autopsy more often than necessary.
Interacting with multiple coroners, even within a single county, does not necessarily complicate the forensic pathologist's role. Many of the counties have a primary coroner to whom the legal authorities turn for most of the cases in that county, although there may be no official designation as a Chief Coroner. Coordination of coroner duties within a county is left to the coroners themselves, who work out their call schedules and regions of county covered. Regularly scheduled meetings between groups of coroners and the forensic pathologist are rare to nonexistent, as are any requirements for an annual report or statistical analysis of data. Budgeting for coroner autopsies, including coroner compensation, pathologist fee, morgue fee, radiographs, toxicology, transportation, etc., is negotiated by the coroners with their individual county legislatures, and bills are paid out of county treasuries. Some counties require a contract and documentation of insurance coverage by the pathologist.
County coroners exhibit variable levels of training and experience, from virtually none to those that rival a seasoned medical examiner. Most coroners take advantage of the educational opportunities and networking available to them through statewide and national courses. Part of the role of the independent forensic pathologist includes on-the-job education of coroners, most of whom greatly appreciate our input and cooperation.
Despite all of the potential drawbacks of forensic pathology in an independent coroner-based environment, there are several advantages. Unlike the typical medical examiner forensic pathologist, an independent forensic pathologist has more autonomy. Scheduling is at his or her discretion. Reimbursement is negotiated with each county, and mainly fee-for-service. Administrative duties may be left to hospital personnel. There is freedom regarding which cases to accept, how to handle certain types of cases, decisions about record keeping, and ability to perform outside legal consultations or private autopsies.
While regional medical examiner offices may seem to be a logical or even preferable alternative to independent hospital-based forensic pathology practice, concerns over cost, transportation, overburdened medical examiners, and communication systems have combined to make the independent forensic pathologist a satisfactory model of practice. The availability of a forensic pathologist is certainly preferable to having none. The adequacy of such a model is judged by the local legislatures, District Attorneys (DA), law enforcement, and the citizens of the community.
There is no coroner-DA in the author's region of New York State, although such a position does exist. The author has not experienced any significant conflicts of interest related to coronial background; the investigators are all trying to do the best job they can, with limited resources. Coroner-MD's make some of the best investigators, as they understand natural disease processes and can usually separate trauma from postmortem artifact or disease. In cases where manner of death is unclear, even after gross dissection, the author advocates to the coroner that “pending” is the preferred designation, until all other studies are completed. Rarely has there been a disagreement over this approach. Lay coroners are thankful to be guided in such decisions and take the heat off their shoulders. A decision about manner of death isn't made without the forensic pathologist's input; otherwise future cases would be going elsewhere.
The independent forensic pathologist has the option of performing other pathologist functions, such as teaching, research, consultation, and/or service work. These duties make for a more variable practice than full-time death investigation and allow the chance to supplement one's income, as well as the chance to be separate from a fully employed model. Independence creates a sense of worth and entrepreneurship. In this region, medical investigators are replaced by law enforcement and coroners who, at least in the author's experience, have done a fine job documenting scenes and communicating salient information, although the author makes himself available to the authorities to attend scenes when special circumstances arise. An independent forensic pathologist can educate lay investigators about documentation. Indeed, in this day and age of electronic communications one can virtually be present at the scene of death.
While the author conducts the vast majority of autopsies in those cases which are liable to wind up in a courtroom, most of the autopsies conducted in the southern tier of New York State are performed by non-forensic hospital pathologists. Indeed, many pathology colleagues may prefer not to involve themselves in the legal system when given the choice. The author makes himself available for forensic supervision and consultation, free of charge. If out of town, selected cases are transported significant distances, often at significant expense, in terms of money, time and communication. As a result, there are occasional cases where a busy forensic pathologist/medical examiner may have to travel back to the region for grand juries or trials, thus disrupting their own practices.
Contrary to popular understanding, coroners are not necessarily in the driver's seat about the necessity for an autopsy. Through continuous feedback and education, the pathologists are able to control the sorts of cases that come into the hospitals for autopsy. At times we have even encouraged coroners to speak to attending physicians about signing death certificates, to convince them that county tax dollars shouldn't be expended for unnecessary investigations.
In summary, until such time as adequate manpower and financial resources are available, a coroner-based death investigation system is still a necessary complement to the medical examiner system in New York State. There are both drawbacks and advantages to such a practice for the independent forensic pathologist. Yet the citizens of this area of New York State are served by a death investigation system that is functional and meets basic needs.
Footnotes
The author, reviewers, editors, and publication staff do not report any relevant conflicts of interest.