
Abstract
Individuals who are intoxicated with alcohol (most commonly ethanol) will commonly be detained by police for a wide range of offenses. It is essential that custody staff are trained to recognize individuals with alcohol use disorders and comorbid health conditions and request medical assistance as required. Forensic physicians and other health care professionals should perform a comprehensive assessment to diagnose alcohol intoxication and ensure that the detainee is fit to be detained and interviewed by police. Forensic pathologists should be aware of the appropriate clinical management of alcohol-intoxicated persons in custody when involved in death in custody investigations.
Keywords
Introduction
Individuals may be arrested by the police and detained in police custody for a range of offenses that are “alcohol-related”: driving with excess alcohol, driving under the influence (DUI)/while intoxicated (DWI), “drunk and incapable,” and offenses where the individual is under the influence of alcohol at the time of committing an offense, in cases of assault (domestic violence, sexual assaults), robbery, or public order incidents. In this article, “alcohol” refers to ethanol unless otherwise specified.
In the United States, about three million violent crimes occur each year in which the victims perceive that the offender has been drinking at the time of the offense (1). In the 2011/12 Crime Survey in England and Wales, there were 917,000 violent incidents where the victim believed the offender(s) to be under the influence of alcohol, accounting for 47% of violent offenses committed that year—a 3% rise from the previous year of 2010/2011 (2). Alcohol intoxication is common amongst detainees in police custody; one UK study suggested that 73% of people detained at night were considered to be intoxicated (3). The consumption of alcohol, especially at high levels, is a significant risk factor for violence (4).
Forensic physicians (FP) and other healthcare professionals (HCPs) working in the UK are often called to assess detainees apparently under the influence/impaired by alcohol. It is essential that a detailed history and an appropriate physical examination, including mental state examination, are performed in order to diagnose alcohol intoxication and ensure that the detainee is safe to remain in custody (5). The guidance outlined in this article is based on clinical practice in the UK, however the principles of management apply to all alcohol-intoxicated persons recently detained by police. Where onsite health care professionals are not available in custody centers, individuals will need to be transferred to a hospital or other medical facility for assessment and treatment. Forensic pathologists should be aware of the appropriate clinical management of alcohol-intoxicated persons in custody when involved in death in custody investigations.
Alcohol is a major cause of harm to individuals and society (6) and alcohol use is an important risk factor for disease in young people aged 10–24 years (7). A significant amount of health morbidity is present among detainees in police custody and often, police screening does not detect significant health problems (8). It is essential that custody staff are trained to recognize these problems and request medical assistance as required (9). A study in London, UK, found that 25% of detainees were alcohol dependent (10). Another study looking at detainees who refused, or were unable to complete a breath alcohol test showed that they had high rates of traumatic injuries when compared to those who completed the test (22% versus 8%) (11).
Pathophysiology of Alcohol Intoxication
Alcohol is a poison and cannot be stored by the body. It produces both acute and chronic health effects. Alcohol acts as a central nervous system depressant by means of potentiating GABA activity in the brain (GABA is an inhibitory neurotransmitter) (12), with small doses affecting cortical function and larger doses depressing medullary function.
Ingested alcohol is absorbed throughout the gastrointestinal tract by passive diffusion in the stomach and with the rate of absorption maximal in the duodenum (13). A small amount of alcohol in the stomach is metabolized by its enzymes, gastric alcohol dehydrogenase. Peak alcohol concentration is reached 30–60 minutes after drinking although the range can be 20 minutes to three hours. Blood alcohol levels may rise after arrest if the detainee has been drinking immediately before arrest.
Following gastrointestinal absorption, the alcohol is carried via the portal vein to the liver. Some of the alcohol is metabolized there, the remainder being transported throughout the body via the systemic circulation where it is distributed around the body tissues according to their water content. Tissues with higher water content will take up more alcohol. Diffusion continues between the blood and tissues until equilibrium is reached. A large number of factors can influence how alcohol is metabolized (
Factors Affecting the Metabolism of Alcohol
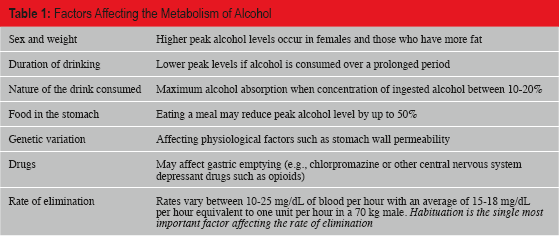
Elimination of alcohol occurs mainly by metabolism through enzyme activity in the liver (approximately 95%). The remainder, approximately 5%, is eliminated unchanged in breath, sweat and urine – an important factor that allows the estimation of blood alcohol concentration (BAC) from the level in breath. However the presence of alcohol in urine only proves that alcohol is present in the body and cannot reliably indicate the blood level due to the fact that alcohol may have accumulated in the bladder over a prolonged period and urine concentration will depend on the hydration of the individual.
Assessment of the Potentially Intoxicated Detainee
The diagnosis of alcohol intoxication requires that there must have been recent ingestion of alcohol associated with behavioral or psychological changes and the necessary physical signs along with the proviso that there are no medical conditions that may account for the condition (15). The terms “alcohol intoxication” and “drunkenness” are often used interchangeably. However, a distinction between these terms is justified as people may exhibit behavioral changes associated with drunkenness when they believe they have consumed alcohol but actually have not (16).
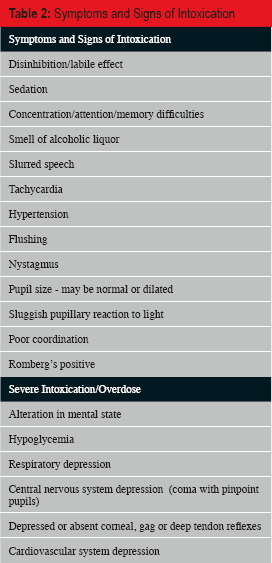
The amount of alcohol taken in the previous 24 hours as well as the usual amount taken each day should be documented. As polydrug use is common, a specific inquiry should be made about the use of other substances, such as benzodiazepines and opiates, which may complicate the assessment. A medical history, including a psychiatric history, should be obtained. The physical examination involves looking for signs of intoxication (
Symptoms and Signs of Intoxication
Symptoms and Signs of Withdrawal
The prevalence of psychiatric comorbidity, mental illness and substance use disorder, is significant. A U.S. survey on drug use and health found 9.2 million adults in the U.S. (4% of the adult population) met the criteria for both a mental illness and substance use disorder in the past year (17). Bradley also highlighted the importance of mental health awareness and learning disabilities to be a key component in police training because of the prevalence of mental illness in the police detainee population (18).
Individuals who have alcohol problems are at an increased risk of self-harm and suicide (19). The National Confidential Inquiry into suicide and homicide by people with mental illness found that the majority of the suicide cases it investigated (58%) were alcohol dependent, 39% were drug dependent and 29% heavily misused both (20). It is essential that a risk assessment is performed as intoxication and withdrawal can increase the risk of self-harm.
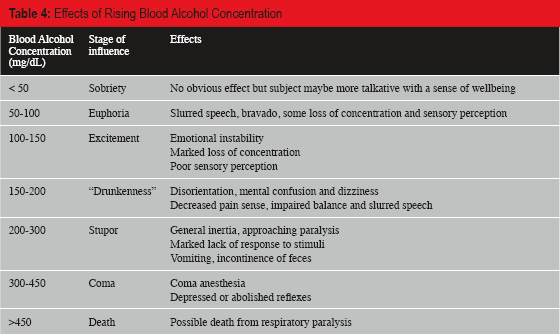
Tolerance occurs to alcohol and so the effects are variable; a guide is provided in
Effects of Rising Blood Alcohol Concentration
It is essential that the FP excludes other conditions (
Differential Diagnosis of Alcohol Intoxication
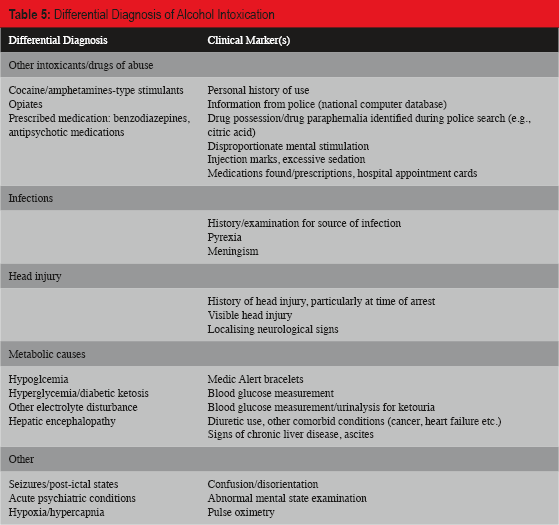
All detainees who are not rousable, are hypoglycemic, hypothermic, have localizing neurological signs, or evidence of head injury or have had seizures, should be referred to a hospital urgently. While awaiting hospital transfer, hypoglycemia may be treated with oral glucose such as “Hypo-stop” in the conscious detainee or intramuscular glucagon in the unconscious detainee, followed by immediate oral glucose once consciousness returns. Glucagon may not be effective in a detainee with liver disease. Intravenous dextrose may be given but may be difficult to administer in the custody environment because of poor venous access.
Those who have severe Alcohol Use Disorder (AUD) may be at risk of Wernicke's encephalopathy, a triad of confusion, ataxia, and nystagmus that may be irreversible. Consideration should be given to offering thiamine to detainees at risk (23).
Detainees suffering from simple intoxication with alcohol without significant comorbidity and who are not judged to be a risk of alcohol withdrawal syndrome may be allowed to detoxify or “soberup” while remaining in police detention.
Any decision regarding fitness to be interviewed should be made on a full, functional assessment of an individual rather than a single specific blood alcohol level (24). However, a hand-held breath testing device may be a valuable tool to confirm the alcohol concentration, thus informing any decision. Salivary alcohol measurement devices may also be of use (25).
Acute intoxication is usually transient and so in the initial period of detention detainees must be checked and roused regularly as per the four “R's” to ensure that the blood alcohol level is falling and the detainee is improving (
Detained Person: Observation List (26)
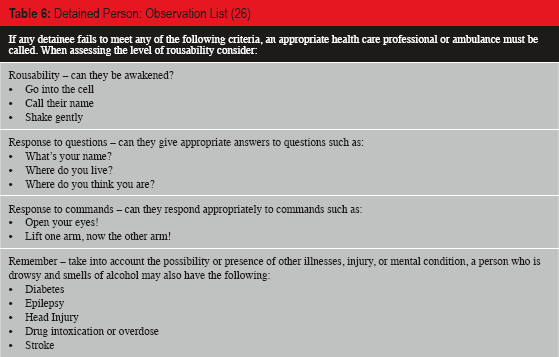
In a review of 58 deaths in police custody over the period 2000–2001 in England and Wales, it was concluded that those with gross alcohol intoxication were not cared for adequately in police custody (27). This was reflected in the failure to implement the FP's instructions regarding the checking and rousing of detainees. If the level of risk is such that increased supervision is needed, the police station is unlikely to be a suitable location for these detainees. Any severely intoxicated detainees, unable to walk and talk, should be transferred to hospital for observation by trained health care professionals and should receive a full assessment.
Alcohol Dependency
Police arrest and detention is often the first presentation of an Alcohol Use Disorder (
Diagnostic and Statistical Manual (DSM) 5 Alcohol Use Disorder (AUD) (28)
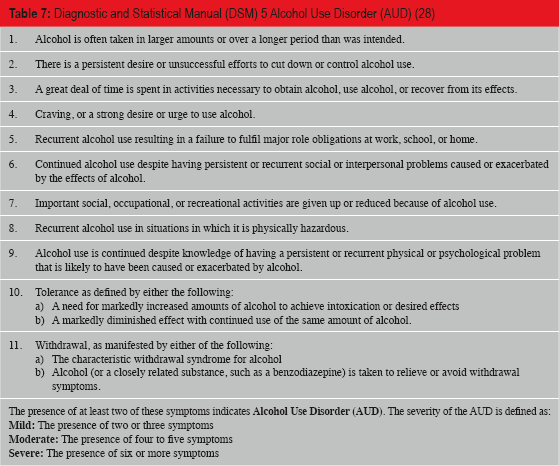
The presence of at least two of these symptoms indicates
Accurate and reliable information about a person's intake of alcohol is difficult, as heavy drinkers tend to underestimate or deliberately lie about their alcohol consumption (30). The use of an alcohol screening questionnaire is essential in identifying alcohol problems including alcohol use disorder. There are a number of tests available: the Alcohol Use Disorders Identification Test (AUDIT) (31) (probably the best screening instrument in this environment) (32), self-report questionnaires – MAST (33,34) and CAGE (35,36), and the Paddington Alcohol Test (PAT) used by accident and emergency departments to identify patients presenting with injuries that may be due to problem drinking (37).
Police custody offers a setting in which there is scope for the early identification of AUD (38). It is possible that such interventions could be administered by healthcare professionals or other custody staff to the detainee prior to release, when the detainee is sober (39), although in a recent study in France, only around 20% of detainees were willing to accept such advice (40).
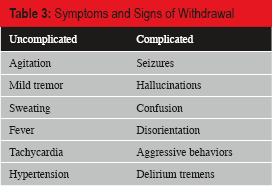
Recognition and Treatment of Alcohol Withdrawal
Alcohol withdrawal symptoms and signs (
It is essential that alcohol withdrawal is recognized and treated promptly in police custody. If unrecognized, there is a significant morbidity and mortality. A long-acting benzodiazepine such as chlordiazepoxide 15–30 mg tid or diazepam 10 mg tid should be used to prevent the complications of withdrawal, such as seizures and delirium tremens. Consideration should be given to prescribing vitamin B compound.
Frequent reassessment by the FP is required. Detainees with significant comorbidity such as liver disease, pregnancy, or a previous history of severe withdrawal symptoms should not undergo detoxification in custody but referred to a hospital.
In hospital settings, the Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) scale is used to quantify withdrawal symptoms and signs and guide treatment (41,42). The application of this score to a custody setting has not been determined and the score requires repeated evaluations to determine the response to treatment. However, patients with a score of over 15 are at increased risk of seizures and the authors recommend that these detainees are referred to a hospital.
Fitness to Interview
A detainee may be at risk in a police interview if conducting the interview could significantly harm the detainee's physical or mental state or if anything the detainee says in the interview about their involvement or suspected involvement in the offense about which they are being interviewed might be considered unreliable in subsequent court proceedings because of their physical or mental state (43).
In cases of intoxication, a period of observation may be required before the detainee is sober and fit to be interviewed. Treatment for alcohol withdrawal may be required prior to interview. Reassessment may be considered necessary after a period of time to establish fitness. Individuals who have AUD may have comorbid conditions that may need treatment prior to interview and/or certain psychological vulnerabilities or risk factors such as mental disorder or intellectual disability (44).
Individuals with severe alcohol use disorder are at risk of false confessions (45), in particular, coerced-compliant confessions, where suspects are fully aware of not having committed the crime but will confess in an attempt to escape from an intolerable situation, and coerced-internalized false confessions, which may occur when suspects believe that they have committed the crime of which they are accused, perhaps temporarily. Individuals with severe AUD may come to distrust their own memory or have memory impairment either due to acute temporary alcohol intoxication or permanent damage are suggestible to external cues. Those with comorbid severe mental illness are also at risk of this type of confession.
Conclusion
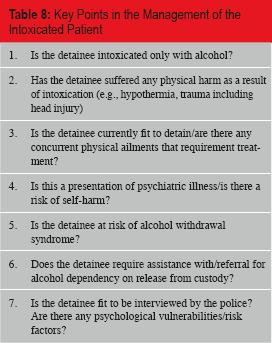
In summary, the key points for the management of the alcohol intoxicated detainee are given in
Key Points in the Management of the Intoxicated Patient
Footnotes
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest.