
Abstract
While diabetes mellitus (DM) has historically accounted for substantial worldwide morbidity and mortality, new and evolving epidemiologic trends are forcing the scientific community to view it as a type of emerging disease. This review will summarize the pathophysiology of the disease, present an update of current national statistics and changing epidemiologic patterns, discuss how DM might specifically lead to acute deaths falling under the jurisdiction of the medical examiner/coroner, and suggest a medicolegal standard of practice to maximize their capture and reporting.
Keywords
Introduction
There is little doubt that diabetes mellitus (DM) represents a tremendous source of morbidity, mortality, and health care costs in the United States. It is equally clear that as a matter of public health, obesity is reaching alarming, even epidemic proportions across all age groups in the United States and abroad (1). As a result, type 2 diabetes is a burgeoning problem within the adolescent population and threatens to present significantly greater challenges to our societal health and the cost to maintain it. In 2012, the Centers for Disease Control and Prevention (CDC) reported that the direct and indirect costs of DM totaled $245 billion. As diabetic adolescents progress into young adulthood and middle age, expected comorbidities such as hypertension, coronary artery disease, peripheral vascular disease, blindness, neuropathies, hypertriglyceridemia, and renal disease will only amplify this problem (1-5). Early onset DM has a well-known correlation with premature mortality (5). In addition, the increased prevalence of DM among schizophrenic patients treated with atypical/second generation antipsychotic agents has been increasingly recognized with the widespread administration of these drugs. Moreover, in reports of DM-associated fatalities in these patients, the overwhelming majority carried no diagnosis of diabetes prior to death (6-10).
From the perspective of the medical examiner/coroner (ME/C), DM has historically constituted a substantial proportion of primary as well as contributory/secondary causes of deaths, given its well-recognized association with cardiovascular disease. In New York City, for example, diabetes mellitus was listed as the cause of death in Parts I or II of the death certificate in 17% of the deaths reported to the Office of Chief Medical Examiner in 2014. If calculated as a percentage only of natural deaths, this proportion would be far greater. When considering mortality related to DM, however, it is more common to think of it in terms of the long-term sequelae of a progressive and protracted chronic illness. Diabetes mellitus is not traditionally viewed as a common primary cause of sudden, unexpected death in and of itself. As a result, it is not necessarily considered by the ME/C when investigating acute deaths, particularly when there is no preexisting diagnosis of diabetes. Yet, in a retrospective analysis of all deaths caused by diabetic ketoacidosis (DKA) over a six-year period in Baltimore, Ali et al. found that nearly a third occurred in individuals in whom no prior history of DM was known (11).
In the context of emerging epidemiologic trends, this review will attempt to address the following medicolegal questions: 1) under what specific circumstances do deaths related to DM occur so suddenly and unexpectedly that they fall under the purview of the ME/C and constitute the mechanism/primary cause of death; 2) whether we expect these “acute” deaths caused chiefly by DM to increase over time; and, 3) if so, how we should as ME/C approach the autopsy so that they are worked up in a standardized and thorough manner to minimize under diagnosing and underreporting.
Discussion
Background: The Pathophysiology and Epidemiology of Diabetes Mellitus
The CDC and National Vital Statistics System ranked DM as the seventh leading cause of mortality in the United States in 2014, citing 75 578 deaths attributable to diabetes as the primary cause, relative to the more than 2.5 million fatalities reported overall. It is also estimated that while 21.1 million people in the United States alone carry a diagnosis of DM (9.3% of population), another 8.1 million people remain undiagnosed (i.e., 27.8% of all people with DM). Moreover, studies have indicated that diabetes is underreported as a cause of death. In 2010, for example, it was listed as a cause of death in just 234 051 persons. Only an estimated 35% to 40% of fatalities among diabetics had “diabetes” listed anywhere on the death certificate and in only 10% to 15% was it listed as the underlying cause. Regardless, after adjusting for other potentially confounding variables, rates of death from all causes are estimated to be at least 1.5 times higher among known diabetics as compared to the general population (12).
Diabetes mellitus is a group of diseases characterized by hyperglycemia resulting from defects in insulin production, insulin action, or both. In adults, type 2 DM accounts for about 90-95% of all diagnosed cases. It affects men slightly more than women and is disproportionately found in African-Americans, Hispanics/Latinos, American Indians, and Pacific Islanders. Other risk factors for developing type 2/adult-on-set diabetes include obesity, family history, older age, physical inactivity, and a history of gestational diabetes (1, 12, 13).
Pediatric disease has historically constituted a unique presentation in the form of type 1 DM (juvenile-onset, “insulin-dependent”), previously maintaining a relatively stable prevalence over many years (5% of all known diabetics), although over the last decade or more, it has experienced a steady rise (21% in eight years) (4). It accounts for the overwhelming majority of diabetes in children less than ten years old, the majority of whom are non-Hispanic Whites. It is distinctly uncommon among minorities. Over 200 000 people under the age of 20 had diabetes in 2012 (12).
Type 1 DM is caused by the autoimmune destruction of pancreatic β cells. Classically, symptoms appear abruptly, often in early adolescence, after most of the β cell population has been destroyed. This leads to hyperglycemia manifesting as polydipsia, polyuria, constant hunger, fatigue, weight loss, and even the precipitous onset of diabetic ketoacidosis (DKA). The diagnosis is usually not subtle and the initiation of insulin treatment tends to be swift.
With the emergence of childhood obesity and increasing inactivity, however, the national prevalence of pediatric type 2 DM has been steadily climbing over the last decade and overwhelmingly and disproportionately affects children and adolescents of minority ethnicities, specifically African-Americans, Hispanics, American Indians, and some Asian and Pacific Islander-Americans. The highest prevalence is found among the Native Americans between the ages of 15 and 19 years (1, 3). Of note, greater than 75% have a family history of DM, a potent risk factor. While its prevalence in the pediatric population is still eclipsed by type 1 DM, its rate of increase has been much swifter than that of type 1 during the same time period (30% over eight years). Until ten years ago, type 2 DM accounted for less than 3% of all cases of new-onset diabetes in adolescents; currently, 45% of new cases are attributable to type 2 in that age group (1). By 2050, a further four-fold increase is projected. The mean body mass index (BMI) of pediatric type 2 diabetic patients in the United States ranges from 27 to 48 kg/m2, although recent data do suggest the first plateau since the 1960's (2, 4). Obesity is undoubtedly the hallmark of type 2 DM, but other disorders such as acanthosis nigricans and polycystic ovarian syndrome are also not uncommonly diagnosed in this setting. Pediatric type 2 DM is also not a uniquely American phenomenon; published data are emerging worldwide. Japan reports that 80% of all new cases of DM in children and adolescents are type 2. In Taiwan, the rate is 54.2%. Similar trends have been reported in Australia, Canada, Libya, and Bangladesh, to name a few (1, 2).
To exacerbate this further, an increase in gestational diabetes is directly associated with the risk experienced by today's youth in developing type 2 DM at a relatively young age. Moreover, diabetic children will become sexually active diabetic adults, themselves becoming at risk for severe gestational diabetes, further aggravating this epidemiologic cycle for the next generation. In Europe, where neither obesity nor gestational diabetes has seen such dramatic increases, studies have shown that type 2 DM remains rare among the predominantly white population (4). A parallel, but less dramatic increase in DM and obesity has also been observed in American adults (1, 4, 12).
In contrast to type 1 DM, type 2 DM often presents more insidiously, making its diagnosis less obvious. Some patients show no symptoms at all for an extended period. As central obesity leads to peripheral insulin resistance, the pancreatic β cells gradually and increasingly become exhausted and ultimately fail to compensate appropriately. Given that the onset and course of this disease is traditionally encountered in the adult population, type 2 DM manifesting early in life presents new and vexing challenges to pediatricians and epidemiologists alike. Adolescents are at an increased and unique risk due to the counterregulatory hormonal effects of puberty (primarily growth hormone). This sets the stage for the development of insulin resistance if the associated risk factors of obesity and family history coexist with it (2, 3). As such, the overwhelming majority of pediatric type 2 diabetics are older than ten years of age (mean age 12-16 years) (2). The challenges of dietary, exercise, and medication compliance during adolescence poses additional potential obstacles to successful medical intervention.
Schizophrenic patients carry a similar heightened risk for type 2 DM relative to the general population, independent of treatment with psychotropic drugs. But, with the added diabetogenic risk of the commonly prescribed atypical antipsychotic agents, they too have become increasingly and uniquely vulnerable to acute onset DM, with or without DKA. Despite this, these drugs continue to be widely prescribed due to their extreme efficacy in treating psychotic symptoms coupled with their greatly diminished motor and sexual side effects relative to the older/first generation medications (6).
Diabetic ketoacidosis is one of the most dreaded of the acute diabetic complications and is more typically associated with type 1 (roughly two-thirds of DKA patients have type 1 DM), but it has been increasingly encountered in type 2 diabetics, particularly when involving the pediatric and schizophrenic populations (13). Regardless of diabetes type, DKA is clinically defined as a venous pH of less than 7.3 or serum bicarbonate lower than 15 mmol/L and serum glucose greater than 200 mg/dL, with ketonemia/ketosis. It results from an absolute or relative deficiency of circulating insulin combined with the effects of increased counterregulatory hormones. This in turn leads to an accelerated catabolic state and intracellular starvation, ultimately leading to the death spiral of severe hyperglycemia, hyperosmolality, ketogenesis, acidosis, osmotic diuresis, loss of electrolytes, and severe dehydration, often exacerbated by vomiting. If this cycle is not interrupted with swift medical intervention, including exogenous insulin and fluid and electrolyte replenishment, sudden death, defined here as death within 24 hours of symptom onset, will likely ensue from any one or more of these many toxic-metabolic derangements. Diabetic ketoacidosis is the most common cause of death in children and adolescents with type 1 DM and accounts for half of all deaths in diabetic patients under the age of 24 years (13).
Acute Fatalities and Diabetes Mellitus: Causes of Sudden, Unexpected Death
Expected deaths related to DM that follow complex sequelae and a protracted course or that occur at home in persons with advanced age and/or comorbidities often do not prompt ME/C involvement. Even if the ME/C does become involved, an external examination will likely represent the extent of the postmortem workup.
By contrast, sudden, unexpected, and otherwise unexplained “acute” deaths in younger persons predictably lead to ME/C involvement, including the performance of a full autopsy with toxicological analysis. Among this group, there are specific scenarios in which DM/DKA should at least be considered as a potential cause of sudden death warranting further analysis. These include, but are not limited to, the following: any death occurring suddenly and unexpectedly in an individual with documented type 1 or 2 DM, any sudden and unexplained death occurring in a clinically obese person with or without an antemortem diagnosis of DM, and any sudden and unexplained death in patients carrying a diagnosis of schizophrenia or schizoaffective disorder who are/have recently been treated with atypical antipsychotic agents. A family history of DM (if known) and/or any reports of generalized malaise, nausea, vomiting, upper respiratory or other infections, psychiatric stress, or drug use shortly preceding the death should only serve to further heighten the index of suspicion for DKA.
If vigilant, the forensic pathologist may not uncommonly render a primary diagnosis of DM at autopsy. The younger the patient, the less likely it is that he/she will have been diagnosed prior to death, particularly when it is type 2, a disease which is typically associated with a much more protracted and insidious onset. Many who are obese, but who have not otherwise been exposed to or educated about the common signs and symptoms of DM, can harbor the disease for months before suffering a sudden death in which DKA or nonketotic hyperosmolar hyperglycemic syndrome (NKHHS) is the mechanism. With further investigation, an inciting physiologic stressor or prodrome might become apparent, but, in a large proportion, no such precipitant is identified at autopsy or by history (6). This is particularly true of acute onset diabetes mellitus associated with atypical antipsychotic agents in schizophrenic patients. This type of iatrogenic DM tends to have a more telescoped course and can present more acutely and severely, with death due to DKA as the ostensible first “presentation” in the absence of the classic antecedent physiologic stressors, signs, or symptoms. This is a particularly typical scenario when there is no ongoing monitoring of serum glucose levels, HbA1c, triglycerides, and weight in the months preceding death and/or when the patient is a poor historian due to severe psychiatric disability. It is unclear, but plausible, that recent acute psychiatric stress/psychosis may play a precipitating role, but this is admittedly difficult to identify in the postmortem setting. In a large case series from the New York City Office of Chief Medical Examiner (OCME) in 2011, only one out of 17 schizophrenic patients dying from DKA had previously diagnosed DM (6-10). Similar to schizophrenics, adolescents dying from DKA with previously undiagnosed DM commonly have no classic or identifiable acute physiologic precipitants. Relative to their type 2 adult counterparts, adolescents also tend to have a more accelerated course from prediabetic to frank diabetes and DKA, leaving less time for detection and anticipation of full-blown disease (1).
Certain segments of diagnosed and undiagnosed diabetics are at a disproportionate risk for repeatedly developing DKA. Like pancreatitis or upper gastrointestinal hemorrhages, DKA carries a very high mortality rate and, if survived, often involves an extended stay in an intensive care unit. The three risk factors most highly correlated with repeated episodes of DKA are noncompliance with diabetes medications, Hispanic ethnicity, and recreational drug use, among which cocaine is far and away the most culpable. Of these three risk factors, acute active cocaine abuse is the one most recently reported in the literature and, as such, is the least recognized by clinicians and pathologists alike. It is also the one most highly correlated with recurrent DKA admissions (14-17). Overall, hospital admissions for DKA are rising at a rate that exceeds even that of the diagnosis of diabetes (13).
In retrospective reviews of large urban medical centers, those patients with acute or recent cocaine intoxications represented as many as 14-26% of all DKA admissions (15-17). It is believed that in addition to associated lifestyle dysfunction potentially exacerbating medication noncompliance, cocaine also serves as an independent risk factor of DKA. As a stimulant, it augments counterregulatory hormones, such as catecholamines, that acutely inhibit insulin secretion, thereby increasing hyperglycemia and glucagon and ketoacid production, even in the absence of a precipitating underlying illness. Arguably, cocaine itself serves as a physiologic stressor mimicking an intercurrent infection that might otherwise precipitate DKA in diabetics. Although to a less dramatic extent, other drugs of abuse, including heroin, methylenedioxymethylamphetamine (MDMA), and amphetamine all have been reported to influence insulin and glucose metabolism, thus potentially enhancing the risk of DKA (14, 18-20).
The relatively young are at greater risk for death related to recreational drug use, the identification of which may derail the forensic pathologist from considering the workup of DKA in the appropriate setting. Given that illicit drug intoxication deaths often occur suddenly and in younger persons, such death investigations will likely fall under the purview of the ME/C. But in a study measuring recurrent DKA admissions in Florida, more than 30% of men and 20% of women between the ages of 26 and 34 years and up to 38% of the psychiatric patients reported active cocaine abuse (15). As such, in the young and obese, with or without a preexisting diagnosis of DM, and in whom DKA is identified at autopsy, the concomitant toxicologic identification of cocaine has the potential to represent both the precipitant and a contributory cause of death, and DKA, the primary cause. If acute cocaine intoxication is included anywhere in the cause of death statement, then the manner of death will also be affected.
Another poorly recognized mechanism by which DKA can suddenly kill is by pulmonary thromboembolism (PE). In this issue, Scordi-Bello et al. report a case series out of the New York City OCME in which seven sudden, unexpected deaths in relatively young persons, only two of which were known to be diabetics, had PE and deep vein thromboses with DM/DKA as the proximate cause through putative prothrombotic/hematologic factors and/or severe DKA-associated dehydration with hyperviscosity. Interestingly, all were males of Hispanic or African-American ethnicity, all but one were younger than 55 years of age (range, 29-52), only two had a slightly prolonged hospital stay, and most had BMI's of less than 32 kg/m2 with no associated thrombotic, surgical, oncologic, or genetic risk factors (21). Like cocaine intoxication, PE is fairly commonly encountered by the ME/C, but is not traditionally viewed as being causally related to DM/DKA. More typically, DKA and PE have been seen as mutually exclusive, competent mechanisms of death in and of themselves with no causal relationship to one another.
While DKA is arguably one of the more common mechanisms by which DM suddenly kills, others reported in the literature deserve mention here, including those related to the much less prevalent type 1 DM. There is some overlap in the types of acute complications related to type 1 versus type 2 DM, but the dead-in-bed (DIB) syndrome is a rare and devastating complication seemingly exclusive to type 1 DM and has gained increasing attention in the literature in the United States and abroad (22-24). After first being described by Tattersall and Gill in 1991, several large-scale, population-based studies have further established definitional criteria and the putative pathophysiologic mechanism (24, 25). Apparently otherwise healthy type 1 diabetics succumbing to this syndrome tend to be young (<40 to 50 years old) and, as such, still free of any of the long-term sequelae classically associated with type 1 DM. Most studies also have identified a male preponderance. These patients are found suddenly and unexpectedly dead in bed with neither antecedent illness nor the identification of DKA or any other demonstrable pathologic or toxicologic cause of death by autopsy. Scene investigations apparently do not suggest perimortal seizure activity.
Compared to the general population, type 1 diabetics less than 40 years of age have a four- to ten-fold rate of sudden, unexpected death (23, 24). The precise mechanism of DIB is not fully understood, but growing evidence over the last decade suggests that it may be related to sudden, unexplained, sleep-related instability in glycemic control and/or a sudden increase in severe nocturnal hypoglycemia, the latter experienced by up to 50% of type 1 diabetics and caused by the autonomic failure of the body to respond to hypoglycemia with counterregulatory hormones (glucagon and adrenaline).
Nocturnal instability of glycemic control is caused by an apparent autonomic neuropathy, which can be related to chronic hyperglycemia in poorly controlled DM, further causing impaired parasympathetic activity, resulting in nocturnal sympathetic predominance. Normally, during sleep, there is physiologically increased parasympathetic tone with a concomitant sympathetic dampening. When the reverse occurs, it can result in a higher mean hourly heart rate and abnormal cardiac repolarization, potentially leading to a transiently prolonged QTc interval, setting the stage for a ventricular tachyarrhythmia and sudden death. In addition, severe hypoglycemia alone can also stimulate the sympathetic system, causing abnormal cardiac repolarization, with or without autonomic instability. These theories are further supported by the disproportionate DIB risk observed in those diabetic patients having both a higher HbA1c and daily insulin requirement, indicative of chronic hyperglycemia, but a lower BMI (23, 24).
Also worth mentioning, despite its rarity, is fulminant type 1 diabetes mellitus (FT1DM), a rare subgroup of type 1 diabetes mellitus. It is characterized by an extremely rapid progression of hyperglycemia and ketoacidosis caused by the hyperacute autoimmune destruction of pancreatic β cells. Because of the rapidity with which this subtype kills (within 24 hours, if untreated), the death will usually fall under the jurisdiction of the ME/C, given its sudden and unexpected nature. Admittedly, the diagnosis of this specific subtype of DM/DKA is more challenging in the postmortem setting than the nonfulminant type (26-28). Finally, electrolyte derangements in both type 1 and 2 diabetics with end stage renal disease have the potential to lead to sudden arrythmic deaths.
In light of the epidemic of adolescent and adult obesity, the steady use of cocaine, the widespread distribution of atypical antipsychotic agents, and the estimated proportion of Americans with undiagnosed diabetes, the forensic pathologist may increasingly be on the forefront of identifying DM as an acute and primary cause of death, as well as an emerging public health problem. But, the ability to make the postmortem diagnosis is only as accurate as our index of suspicion, postmortem laboratory technology, and consistent standards of forensic practice.
Postmortem Diagnosis: Current Practices, Limitations, and Emerging Methods
The postmortem diagnosis of DKA lies primarily in the biochemical analysis of vitreous humor (VH), as opposed to any morphological method (necropsy, histology, and immunohistochemistry). Given that blood glucose decreases by 12.6 mg/dL per hour in the postmortem milieu, the definition of elevated glucose in the autopsy setting diverges substantially from that of the clinical (29). In terms of postmortem blood testing, it is widely accepted that postmortem blood is unsuitable for the diagnosis of hyperglycemia (11).
While vitreous humor is the fluid of choice, urine can be substituted when VH is unavailable (e.g., advanced putrefaction). In the appropriate context and at the exclusion of an efficient intervening and unrelated cause, the combination of acetone (ketones) and substantially elevated vitreous/urine glucose concentration is sufficient to render a diagnosis. Incumbent upon this detection, however, is the reflexive laboratory quantitation of VH glucose once acetone is detected during routine screening, with or without a specific request made by the forensic pathologist. With this in place as standard operating procedure, unexpected DKA will not go undetected, even if the index of suspicion is low.
A caveat in the diagnosis of postmortem hyperglycemia, however, is the fact that, even in VH, glycolysis causes a marked decrease in glucose concentration (11, 30). By contrast, markedly reduced environmental temperatures, such as that found in hypothermic deaths, slow the rate of glycolysis, potentially spuriously elevating glucose concentrations, as may the purported agonal adrenaline response (31, 32). Similarly, the detection of acetone alone in the blood and/or VH is nonspecific, as it can be found in starvation, alcoholism, isopropanol ingestion, and putrefaction. As such, only elevated VH/urine glucose (typically greater than 200 mg/dL) in combination with the presence of vitreous/serum acetone (typically greater than 0.01 g/dL) is a reliable indicator of antemortem hyperglycemia and ketosis (i.e., DKA). When marked elevations in vitreous glucose are found in the setting of very low or absent acetone, the possibility of nonketotic, hyperosmolar, hyperglycemic syndrome (NKHHS) should be considered if the context dictates. Finally, it must be emphasized that when DM/DKA is related to atypical antipsychotic agents, the mechanism of death is not one of a dose-related acute toxicity, per se, but rather of chronic metabolic derangements. As such, the putative psychotropic drug may or may not be detected at the moment of death and its absence does not necessarily exculpate the medication of its potential causal association, depending upon history.
Adjuncts to the above diagnostic strategies include routine histologic evaluation in which characteristic pathology such as Armanni-Ebstein renal lesions (complete clear cell change due to renal tubular cytoplasmic glycogen deposition, as opposed to subnuclear/basal lipid vacuolization;
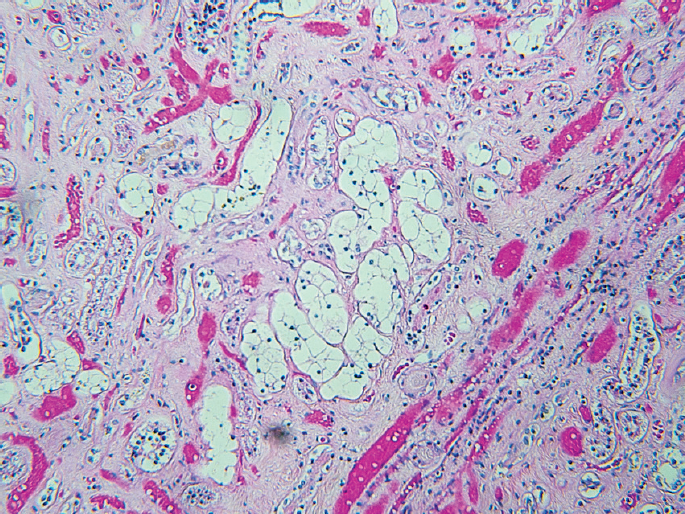
Typical Armanni-Ebstein lesion: renal tubular clear cell change due to complete intracytoplasmic glycogen deposition in patient with diabetic coma (H&E, x100). Image courtesy of the collection of Dr. Chong Zhou.
Arguably equally important to the above in terms of arriving at an accurate and clinicopathologically correlative diagnosis is the thoroughness with which the medicolegal death investigation is conducted. Medicolegal death investigators and forensic pathologists alike must be knowledgeable of the pathophysiology of DM/DKA and the disparate demographic, sociologic, and clinical circumstances in which it may arise, thus maintaining a high index of suspicion. Pertinent positive and negative answers to questions related to unexplained recent weight gain or loss, polydipsia, polyuria, family history of DM, psychiatric diagnoses and medications, recent dosage changes, illicit drug use, and antecedent prodromes such as nausea, vomiting, malaise, and upper respiratory infections must be assiduously sought and documented.
Conclusion
Looking to the Future
The convergence of an increasingly obese population, widely prescribed atypical antipsychotic agents, a high prevalence of undiagnosed diabetics, and steady/ongoing illicit drug use in the young creates the medicolegal equivalent of a perfect storm for the potential growing incidence of sudden/acute diabetic deaths.
Specific sets of circumstances under which sudden, unexpected diabetic deaths are most likely to occur have been described in this review. Many constitute new and emerging and/or previously minimally reported epidemiologic trends, primarily with regard to type 2 DM. As such, medicolegal death investigators might reasonably expect to encounter DM as an increasing cause of or contribution to sudden death, viewing it not just through the lens of the multiple sequelae of chronic disease. If vigilant, forensic pathologists might similarly expect to make a primary diagnosis of DM at autopsy, often with DKA as the mechanism. Like the postmortem diagnosis of hypertension, the ME/C mustn't be hindered from rendering such an opinion simply because of the absence of an antemortem diagnostic workup and they should routinely initiate testing in even moderately obese adolescents who die suddenly and unexpectedly. A high index of suspicion combined with consistent and thorough postmortem biochemical analyses and medicolegal death investigations will only enhance the capture and confidence rate of these metabolic derangements, particularly if a specific emphasis is placed on automatically testing for VH/urine glucose once acetone is detected.
Because of the significance of tracking the morbidity and mortality of DM, the medical treatment of schizophrenia, and the risks of drug abuse, these death certifications take on a potentially much greater importance from public health and epidemiologic perspectives. Forensic pathologists must recognize the critical role they may play in the identification of many of the 8.1 million diabetics who remain undiagnosed prior to death. Also, adverse events related to atypical antipsychotic agents, when reported to the Food and Drug Administration Medwatch program, can potentially decrease morbidity and save lives in the long run. Strict accounting of these sudden deaths can only aid in our evolving understanding of diabetes mellitus, its detection and varied presentations and modified risk factors, and its future cost to societal health, both epidemiologically and financially.