
Abstract
Background
Nasal valve (NV) stenosis is a well-known cause of nasal obstruction (NO) and congestion but it is often overlooked because the typical surgical therapies are complex and often associated with cosmetic changes. A simplified surgical procedure is needed to address straightforward stenosis of the NV in patients with no need of cosmetic improvement or cartilage grafting. The purpose of this article is to describe a simplified surgical procedure to relieve symptoms of NO without extensive surgical dissection, sedation, cartilage grafting, or cosmetic change.
Methods
This article describes a retrospective consecutive case series of patients that underwent a surgical procedure to correct NV stenosis in the office setting. The procedure is described in detail along with patient outcome assessment using a visual analog scale of patient satisfaction and a questionnaire regarding perceived postoperative cosmetic changes.
Results
Of 190 patients that underwent the procedure, 36 were done in the office setting and 28 completed the questionnaires. Six patients (21%) reported an improvement score of 10, a score of maximal improvement in breathing. The mean breathing score was 4.4, indicating an overall improvement in breathing ability after correction. No patient reported a major cosmetic change and three patients reported a subtle change. The remainder (89%) reported no perceived change in cosmesis.
Conclusion
In-office surgical correction of the NV specifically targeting the mucosa, fibrous tissue, and caudal upper lateral cartilage was feasible, safe, and reliable in relieving complaints of NO due to uncomplicated NV stenosis.
The original description of the NV is credited to Mink (1903) who defined it anatomically as the narrowest portion of the nasal cavity. 1 It is the two-dimensional slit-like opening between the caudal edge of the upper lateral cartilage (ULC) and the septum. Deformities of the NV are a well-recognized cause of complaints of NO. However, because of the plethora and complexity of procedures described to open the NV, this cause of NO is often neglected. Most of these complex procedures involve significant surgical dissection and cartilage grafting and are indicated for patients with iatrogenic, traumatic, or congenital narrowing of the NV that would benefit from relief of their subjective complaints and a cosmetic improvement. These techniques add stiffness and volume to the lateral nasal wall and middle vault resulting in cosmetic as well as functional changes. However, a large population of patients exists with primary uncomplicated NV obstructions that do not desire a complex procedure, need cartilage augmentation, or cosmetic improvement. For these patients a more targeted approach is warranted without the use of cartilage grafting, extensive dissection, or cosmetic change.
We describe an in-office surgical technique of correcting NV stenosis that is targeted with minimal surgical dissection requiring only local anesthesia. This method results in negligible cosmetic changes while achieving relief of NO in the majority of patients.
Methods
This report describes a retrospective case series of all patients who underwent in-office surgical correction of NV stenosis performed at our institution between September 2003 and October 2006. Charts were reviewed to identify all patients who underwent correction of NV stenosis during this period and those that underwent in-office correction were selected.
The age and sex of the patients were recorded along with the date of the in-office correction of NV stenosis. Note was made on whether the procedure was bilateral, right-sided, or left-sided. Any simultaneously performed interventions were also recorded. Paper and electronic charts were reviewed for all other nasal and upper airway procedures performed either before or after correction.
Patient satisfaction regarding improvement in breathing and change in appearance were assessed using an anonymous questionnaire. A visual analog scale (-10 to +10) was used to quantify improvement in breathing after the procedure and the patients were given three choices regarding their perceived change in appearance and a numeric value was assigned to each of the responses: no change = 1, subtle change = 2, and major change = 3 (Fig. 1). With regard to the visual analog scale, a score of -10 was maximal worsening of breathing and a score of +10 was maximal improvement in breathing.
Questionnaire 1 is the visual analog scale that was provided to patients to rate their surgical result. The patients were asked to place an “x” somewhere along the line. Questionnaire 2 was used to rate the patients’ perceived change in their appearance.
All patients included in our study underwent in-office correction of NV collapse using a standardized protocol. Figure 2, A-D, is a schematic representation of the procedure. The procedure is performed with the patient in a recumbent position and Betadine paint (Seton Scholl Healthcare, Oldham, Lancs., U.K.) is applied to the nasal tip and nostrils. Local anesthesia consisting of 1% lidocaine with 1:100,000 epinephrine is injected over the prominence of the caudal ULC on the treated side taking care not to distort this landmark. Two parallel incisions are made on either side of the caudal ULC (Fig. 2 A). The strip of mucosa between the cuts and underlying fibrocartilaginous connective tissue is removed (Fig. 2 B). The caudal ULC is grasped and ∼1-2 mm is resected (Fig. 2 C). The final step is to close the incision with three interrupted 4-0 chromic sutures (Fig. 2 D).
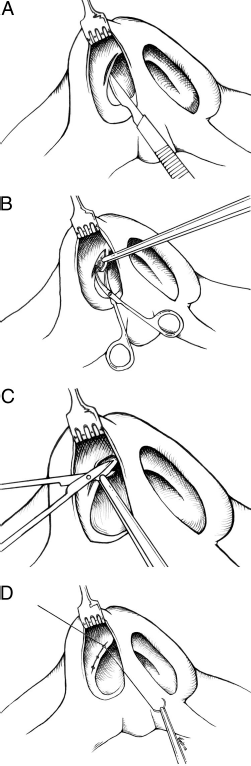
(A) The initial incisions are performed ∼2 mm apart on either side of the caudal ULC through the mucosa and underlying fibrous tissue. (B) The mucosa and underlying fibrous tissue is grasped with a fine-toothed forceps and removed with scissors. (C) Approximately 2 mm of caudal ULC is excised. (D) Three 4-0 chromic sutures were used to close the incision.
Our selection of patients for in-office repair versus repair under a general anesthetic included the following considerations:
Whether the patient required other procedures that in our practice requires general anesthesia including endoscopic sinus surgery, septoplasty, or nonnasal procedures such as tympanoplasty or uvulopalatopharyngoplasty—in these cases the repair would be done under general anesthesia coincident with the procedure requiring a general anesthetic.
If the patient was a significant operative risk due to an underlying medical condition(s)—in these cases the repair was performed in-office as a low risk alternative to general anesthesia.
Results
A total of 190 patients underwent repair of uncomplicated NV stenosis at our institution during the study period. Thirty-six patients (19%) had in-office procedures. Of these 36 patients, 28 (78%) completed the study by responding to the questionnaires. Range of follow-up was 19-55 months (median, 30 months).
A total of 21 men and 15 women underwent in-office correction of NV collapse. Of those responding to the questionnaires, approximately one-half were men (54%). The average age of respondents was 59 years.
Sixteen patients had bilateral procedures. Ten patients had right-sided procedures and the remaining 10 patients had left-sided procedures. Of the respondents, 11 patients had bilateral procedures, 9 patients had left-sided procedures, and 8 patients had right-sided procedures.
Breathing improvement scores ranged from -5 (one patient) to +10. Only one patient reported a decrease in breathing ability (the single “-5” score). Six patients (21%) reported an improvement score of + 10, a score of maximal improvement in breathing. The mean breathing score was 4.4, indicating an overall improvement in breathing ability after correction. Improvement scores for bilateral procedures versus unilateral procedures were 4.5 and 4.2, respectively.
No patient reported a major cosmetic change while three patients reported a subtle change. The remainder (89%) reported no perceived change in cosmesis. Two patients had undergone prior rhinoplasty and reported no changes in cosmesis (score of “1”). Each of these patients reported a “3” in their breathing improvement score. Twenty patients (71%) had a history of nasal surgery including turbinate reduction, functional endoscopic sinus surgery, septoplasty, and pillar implants (a total of 20 procedures overall) before correction of NV stenosis.
Of the 164 patients that had undergone the NV procedure in the operating room, 64 patients returned the questionnaires. All of these patients had undergone additional procedures that in our practice requires general anesthesia including endoscopic sinus surgery, septoplasty, or nonnasal procedures such as tympanoplasty or uvulopalatopharyngoplasty. The average breathing improvement score was 3.42 and no patient reported a major cosmetic change (mean score for cosmetic change was 1.20).
Discussion
In-office surgical correction of the NV specifically targeting the mucosa, fibrous tissue, and caudal ULC was feasible, safe, and reliable in relieving complaints of NO due to uncomplicated NV stenosis. Respondents reported their satisfaction with the described procedure on a visual analog scale similar to a method previously described in this journal. 2 This study shows that the procedure possesses unique advantages including minimal access, convenience, simplicity, and low risk.
There exists a variety of causes of static obstruction in the NV area including inferomedial displacement of the ULC as addressed in this article, scarring or mass at the NV, turbinate hypertrophy, septal deviation, and narrowing at the piriform aperture. Static narrowing at the NV is common after overresection associated with reduction rhinoplasty. However, static dysfunction is a common reason for complaints of congestion and NO in patients with no history of trauma or surgery and it is the anatomy at the scroll that is key to understanding this pathology. The scroll describes the interdigitation of the ULC with the lower lateral cartilege (LLC). In its normal anatomic configuration, the caudal ULC sweeps medial to the cephalic LLC at the NV. At its very distal extent the ULC curves laterally to interlock with a medially curling LLC. Static dysfunction and closure of the NV may be present for a variety of reasons including excessive scrolling, inferomedial displacement of the caudal ULC, and medial displacement of the entire ULC (common after rhinoplasty). Gray reviewed a variety of anatomic configurations at the scroll that can result in NV narrowing, the most obvious of which is inferomedial displacement of the caudal ULC that occurs in ∼20% of cases. 3 Physiological airflow measurements have indicated that airflow is greatest through the NV at the level of the scroll during inspiration. Even minor changes in the opening of the valve can disrupt this airflow and lead to complaints of NO. 4 Although excessive resection of either the ULC or the LLC at the scroll could result in weakening and exaggerated collapse of the NV during inspiration, a conservative resection of caudal ULC and its overlying mucosa as described in this article will sufficiently open the valve relieving obstruction while minimizing excessive collapse.
Clinical assessment of patients complaining of NO should address the three main components of the NV area including the septum, inferior turbinates, and NV (internal NV). If significant septal deviation or inferior turbinate hypertrophy exists, then these abnormalities should be corrected before targeted correction of the NV. Septal deviation at the NV should be addressed as a part of routine septoplasty. Treating the septum and turbinates first is important because even in patients with narrow NVs these procedures often adequately relieve their nasal obstructive symptoms. For patients with persistent complaints of NO with NV stenosis after septoplasty and/or turbinoplasty or for patients with primary NV stenosis without septal or turbinate pathology, targeted correction using the technique described in this report should be considered. This technique obviates the need to return to the operating room and can be done conveniently as an outpatient procedure in the office.
Assessment of NV pathology always requires direct observation of the NV area with or without an endoscope. The valve angle is normally open between 15 and 20° in the static state. The patient with complaints of NO only on sniffing or deep nasal inspiration but has a statically open valve should be observed for dynamic narrowing, which is a normal physiological function. Those with collapse on normal or slightly labored inhalation require stiffening of the lateral nasal wall and are not candidates for the procedure described here. Patients with closed or severely narrowed valves at rest or during normal nasal inspiration that improve with manual opening of the valve are candidates for the described technique. These patients invariably report relief with the Cottle maneuver and often report the use of nasal strips.
Resection of the caudal ULC for alleviation of nasal obstructive symptoms was first described in an obscure article by Gray in 1970 and cited by Kern (1978) in his extensive review of NV surgery.3,5 Kern described two fundamental goals of NV surgery 1 : reconstitute the normal anatomy and 2 improve airflow without increasing the rigidity or collapsibility of the NV. One additional concern is cosmetic change that may be desirable in some circumstances. Since the publication of Kern's review 5 a plethora of procedures have been described to address pathology at the NV most involving augmentation techniques including cartilage grafting often after classic reduction rhinoplasty. The patient with cartilage deficiency may need the added rigidity of a cartilage graft and may also benefit from the changes in the appearance of the nose associated with cartilage grafting. However, in our patients, Kern's fundamental goals apply and contemporary techniques that involve cartilage grafting are not indicated.
Our technique is a modification of Gray's consistent with Kern's goals. Gray described removing a triangular segment of the medial and caudal ULC via an intercartilaginous incision. The “returning” caudal ULC was excised if necessary followed by an excision of a small triangular segment based medially with its apex at the junction of the ULC and septum. Gray stated that conservative ULC resection (2-4 mm) was necessary to avoid destabilization of the NV. Interestingly, excision of a triangular segment of caudal ULC has been performed for cosmetic narrowing of the upper lobule along with more a conservative complete strip from the lower lateral cartilage to achieve a cosmetic improvement of the nasal tip (The Rhinoplasty Society Meeting, San Diego, CA, personal communication, May 2008). Potential cosmetic complications of resecting the cartilages at the scroll include excessive narrowing and pinching along the lateral nasal walls, alar retraction, and contour irregularities. By resecting only the caudal-most ULC and leaving intact the cephalic LLC cosmetic consequences are minimized most likely because the cephalic LLC is positioned laterally and shelters the caudal ULC. We modified Gray's technique to include resection of the entire 1-2 mm of the caudal ULC to establish the position the ULC deeper in the nose—a maneuver that mimics the effects of the Cottle maneuver on the position of the NV. 6 We also resect a bridge of mucosa to eliminate redundancy and flaccidity of the NV to address the concern of excessive valvular function during moderate inspiration. Despite removing cartilage along the lateral aspect of the caudal ULC cosmetic changes were minimal probably because the lower lateral cartilages were not altered. Although not tested in our study we agree that the limitations of this technique, also stated by Gray, include the inability to significantly widen the NV angle because of congenital, iatrogenic, or traumatic causes. In these cases cartilage and/or mucosal grafting should be considered. 7
Footnotes
Acknowledgments
The authors gratefully acknowledge the assistance of Joanne Bilmazes in data collection and organization.