
Abstract
Background
Cooling may induce nasal obstruction. In our previous study, we showed low temperature induced a rapid relaxation of isolated human nasal mucosa and it was independent of vasoconstriction. The aim of this study was to elucidate the mechanism responsible for such findings.
Methods
Nasal mucosa strips were prepared from inferior turbinate samples. Decellularization of human nasal mucosa was achieved by treatment with sodium dodecyl sulfate 0.1% for 15 hours at 37°C in a shaking water bath. Then, the effect of cooling (37-10°C) on the isometric tension change of decellularized nasal mucosa was evaluated. In addition, the presence of elastic fibers within the nasal mucosa was identified in both histological section and scanning electron microscope.
Results
Results indicated cooling induced a relaxation response of isolated decellularized human nasal mucosa and it was similar to that of intact nasal mucosa. The elastic fibers formed in wavy lines and were distributed throughout the submucosal layer.
Conclusion
Cooling induced a similar relaxation response both in the absence or in the presence of cellular components in isolated human nasal mucosa, suggesting that this response is mediated by the abundant extracellular matrix.
Keywords
In a cold climate, nasal resistance tends to increase both in literature and in clinical observation.2,3 In our previous study, we showed that cooling induced a rapid “relaxation” in isometric tension recording of human nasal mucosa both in the absence and in the presence of α1-adrenoreceptor agonist, methoxamine, 10 μM, suggesting that this cooling-induced relaxation was independent of vasoconstriction. 4 This is consistent with the clinical observation of nasal obstruction in a cold climate. However, its mechanism is not well understood. Thus, the aim of this study was to elucidate the mechanism of cooling-induced relaxation of human nasal mucosa in vitro. In addition, an explanation of the tendency of increased nasal resistance in a cold climate was proposed.
Materials and Methods
Patients
Nasal mucosa strips were prepared from inferior turbinate samples. Nasal surgeries were performed on patients (8 men, 21-37 years old) who suffered from chronic nasal congestion. The study was approved by the Institutional Review Board of Tri-Service General Hospital.
Isometric Tension Recording of Isolated Human Nasal Mucosa
The preparation for recording isometric contraction of nasal mucosa was as described previously.4,5 Briefly, turbinate mucosa were trimmed to a length of 10∼12 mm and a width of 5∼7 mm. One end of the strip was tied to an adjustable steel holder and placed in a water-jacketed 30-mL glass chamber containing Krebs’ buffer solution of the following composition (mM): NaCl, 118; KCl, 4.7; MgSO4, 1.2; CaCl2, 2.5; KH2PO4, 1.2; NaHCO3, 25; and glucose, 11.1. The solution was aerated continuously with 95% O2/5% CO2 gas. The other end of the strip was attached with a 3-O silk ligature to a Grass FT-03 force displacement transducer (AstroMed, West Warwick, RI). The tension changes of tissues were continuously recorded by using Chart V4.2 software analysis (PowerLab, ADInstruments, CO Springs, CO) and passive tension of 1.0 g was applied to the turbinate strips and they were allowed to equilibrate 60 minutes at 37°C. When analyzing the influence of cooling on turbinate strips, the temperature reduction was achieved by a thermocontrolled water pump (First Scientific, Taipei, Taiwan) that circulated water through the water-jacketed glass chambers. Approximately 1 minute was needed to reach each desired temperature in a stepwise manner from 37 to 10°C (37, 30, 25, 20, 15, and 10°C).
Decellularization Method
The extracellular matrix (ECM) of human nasal mucosa was made according to a method described earlier. 6 The specimen was placed in detergent solution (sodium dodecyl sulfate, 0.1%) in a 37°C shaking water bath for 15 hours to remove the cellular components. The nasal mucosa was then washed with agitation 5 times in phosphate-buffered saline for periods of 10 minutes each and then was used for an isometric tension study.
Elastic Fiber Stain
The elastic fiber stain of human nasal mucosa was performed according to the manufacture's instruction (Sigma, St Louis, MO). The frozen section of the nasal mucosa specimen was performed by cryostat (Leica, Wetzlar, Germany) with slice thickness of 12 μm. Next, the slice was placed in working elastic stain solution, which contains hematoxylin solution, ferric chloride solution, and Weigert's iodine solution, for 10 minutes and then rinsed. The slice was differentiated in working ferric chloride solution for 1 minute and rinsed in tap water. Then, the slice was rinsed in 95% alcohol to remove iodine and rinsed in deionized water. The slice then was stained in Van Gieson solution for 1 minute and rinsed in 95% alcohol. Finally, the slice was dehydrated to xylene and mount.
Elastic Fiber Preparation for Scanning Electron Microscope
Elastic fiber preparation was made according to a method described in a previous study. 7 The nasal mucosa from inferior turbinates were cut into cubes of 5 X 5 X 5 mm and fixed with 4% paraformaldehyde in a 0.1-M phosphate buffer overnight. The tissue pieces were treated in a 90% formic acid aqueous solution at 45°C for 3-4 days. Then, they were rinsed in Mcllvaine buffer diluted with the same volume of distilled water at room temperature for several hours and fixed with a 0.5% tannic acid for 2 hours. After rinsing with distilled water, they were fixed in a 1% OsO4 aqueous solution for 2 hours and then dehydrated through graded concentrations of ethanol, freeze-cracked in liquid nitrogen, and freeze-dried using t-butanol.
The specimens were fixed overnight in 2% paraformaldehyde-2.5% glutaraldehyde in 0.1 M of cacodylate buffer adjusted to pH 7.4. After being washed in 7% sucrose in cacodylate buffer, the specimens were cut from the center to the edge with clean single-edge razor blades into 1-mm-wide strips. Postfixing was done in the dark in a 1% aqueous osmium tetroxide solution (Polysciences, Warrington, PA) for 1 hour. The specimens were dehydrated via a graded series of 25, 50, 75, 70, 80,90, 95 X 2, and 100% X 3 ethanol. The ethanol was displaced with carbon dioxide, and the tissues were critical-point dried in a Critical Point Dryer (HCP-2; Hitachi, Tokyo, Japan). After coating them with gold platinum using an Ion Coat (IB-2; Hitachi), all specimens were placed on mounts by use of double-stick tape and examined in a scanning electron microscope (S-2400; Hitachi) equipped with a high-resolution CCD camera and operated at 15 kV at a working distance of 15 mm and a magnification of X300∼1000.
Results
The postdecellularization nasal mucosa was mechanically strong. Grossly, postdecellularization nasal mucosa appeared pale and larger with normal consistency and handling characteristics similar to fresh nasal mucosa. The decellularized nasal mucosa showed no vasoconstrictive response after nor-epinephrine, 10 μM, in isometric tension study, when compared with intact nasal mucosa (Fig. 1).
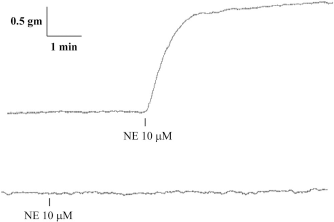
Original recordings of the vasoconstrictive response induced by norepinephrine (NE) in isolated intact (top) and decellularized (bottom) human nasal mucosa.
Cooling (from 37 to 10°C) induced a rapid relaxation in isolated decellularized human nasal mucosa (Figs. 2 and 3). The response to cooling in decellularized nasal mucosa was very similar to that of intact nasal mucosa in our previous study. 4 However, the variation of tension change, as reflected by the standard deviation, in response to cooling in decellularized nasal mucosa was much smaller. Also, there was no overshoot response (i.e., in the intact nasal mucosa, the tension increased much more in the beginning of rewarming and gradually returned to the baseline) in the decellularized nasal mucosa.
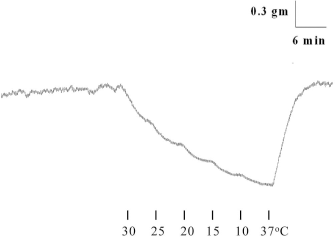
Original recording of cooling-induced relaxation of isolated decellularized human nasal mucosa.
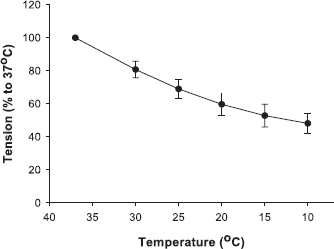
Effects of cooling on the tension of isolated decellularized human nasal mucosa. Each point represents mean ± SD (n = 8).
The elastic fibers formed wavy lines. They were distributed primarily in the submucosal layer of nasal mucosa (Fig. 4). In the electron microscopy view, the elastic fibers formed a three-dimensional scaffold-like structure (Fig. 5).
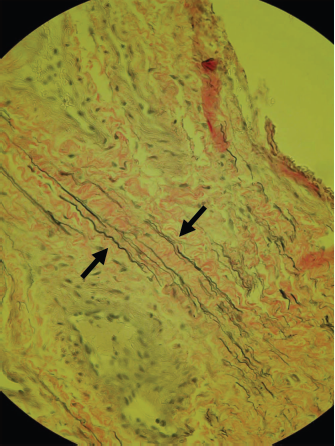
Histological section of human nasal mucosa showing the elastic fibers (arrows) within the submucosal layer (X200).

Scanning electron microscope of human nasal mucosa showing the three-dimensional structure of elastic fibers (bar = 50 μm).
Discussion
In our study, the postdecellularization nasal mucosa revealed loss of nuclei in H&E stain and showed no vasoconstriction in response to norepinephrine, 10 μM. The similar response of both intact and sodium dodecyl sulfate-treated nasal mucosa proved that the ECM was responsible for the cooling-induced relaxation observed in our previous isomet-ric tension study. However, the ECM is a complex structural entity surrounding and supporting cells. Among the various components of ECM, elastin, which is the backbone of mature elastic fibers, is a cross-linked, very hydrophobic protein that provides elasticity in connective tissues. Interestingly, elastin undergoes an “inverse temperature transition” and the protein becomes smaller, or “hydrophobic association,” as the temperature increases. This paradoxical phenomenon is more apparent under the condition of isometric tension recording.8,9 It has been shown that vessels with a great amount of elastic fibers showed dilatation during cooling.10–12 Furthermore, the cooling-induced relaxation of isolated vessel was still present after the NaOH-digested procedure, in which only the elastic fiber components remained intact. 13 In this study, we showed that the elastic fibers formed three-dimensional, scaffold-like wavy lines in human nasal mucosa and it could be an important factor of the in vitro cooling-induced relaxation.
In previous literatures, both the nasal mucosal blood flow, which was measured by radioactive xenon washout method, and nasal patency in healthy subjects decreased in response to cold ambient air temperature (6°C). 2 Also, nasal mucosal temperature and blood flow, which was measured by laser Doppler flowmeter, decreased via neural reflex when subject's feet were immersed in cold water (10°C). 14 Theoretically, the decreased blood flow of nasal mucosa in response to cooling either means direct vasoconstriction or stagnant blood flow that is assumed to result from “throttle veins,” which regulate drainage of blood from the venous sinusoids. 15 To the latter, this should lead to an increase in hydrostatic pressure in the venous sinusoids and a worsening situation in case of epistaxis. Nevertheless, it is generally considered helpful to apply cold compresses or ice on the bridge of the nose or neck during nose bleeding. A study also showed that an ice pack on the neck decreased the nasal cavity volume measured by acoustic rhinomanometry, 16 suggesting a direct vasoconstriction of nasal mucosa in response to local cooling. If the decreased blood flows in response to cooling stands for direct vasoconstriction, it should lead to a decrease in nasal mucosal volume and a subsequent decrease in nasal resistance. However, this seems not to be the case. As mentioned previously, the nasal resistance tends to increase in a cold climate. Furthermore, swelling of the nasal mucosa as reflected by a decrease in nasal cavity volume measured by acoustic rhinomanometry was noted during the immersion in a 15°C cold-water bath. 3 This suggests that the increased nasal resistance during cooling is caused by volume change of nasal mucosa. On the other hand, the nasal mucosal temperature and blood flow measured by laser Doppler flowmeter increase in response to passive body warming.17,18 In addition, after exposure to hot room temperature (40°C), the increased nasal patency was registered. 2 These aforementioned studies suggest a discrepancy between nasal mucosal blood flow and nasal resistance in response to different temperatures.
Our studies may give an explanation of the foregoing discrepancy. We hypothesize that in cold ambient air temperature, the inspiratory cold air causes cooling of nasal mucosa and induces the relaxation and assumed expansion of ECM with its cellular components. Cooling also activates the sympathetic tone and, by our previous study, moderate cooling (24°C) also enhanced the contractile vascular responsiveness of human nasal mucosa at the postjunctional level. 19 Thus, during cooling, the volume change of turbinates may be a dynamic balance between the shrinking effect caused by sympathetic-innervated vasoconstriction and the enlarging effect caused by the ECM, probably the elastic fibers. The net result is an increase of turbinate volume and nasal resistance. Such phenomena may be caused by the abundant connective tissue constituents (>50%) in human inferior turbinate. 20
The physiological meaning for the tendency of increased nasal resistance in a cold climate may be as follows. As the nasal resistance increases, it will cause more expiratory turbulent airflow and thus facilitates heat exchange between the expiratory warm humid air and the cooler nasal mucosa. The cold ambient air, along with the mucosal vasoconstriction, will further cool the nasal mucosa and increase the temperature gradient between expiratory air and nasal mucosa and enhance the reuptake of body heat. A previous numerical simulation study also suggested that cooling of the expiratory air primarily takes place in inferior and middle turbinates. 21 In addition, the cooler nasal mucosa will lead to condensation of humid expiratory air and prevent excessive water loss.
Our study had its limitations. First, the formic acid-digested nasal mucosa was too mechanically weak to be studied by isometric tension recording and thus the formic acid digestion method was only used for scanning electron microscope. Consequently, the cooling-induced relaxation of elastic fibers can not be directly observed by isometric tension study. Second, although the isometric tension recording is a well-documented experimental tool with quantification of force development, the correlation between in vitro tension change and in vivo volume change of nasal mucosa is still a debatable issue.
Conclusions
Our study showed that cooling induced a similar relaxation response both in the absence and in the presence of cellular components in isolated human nasal mucosa. We suggested this response was mediated by the abundant ECM. The elastic fibers might play an important role in such cooling-induced relaxation.