
Abstract
It may be argued that the singular skill that defines the profession of psychiatry is the ability to conduct a psychiatric interview. That said, the qualities of a good interview are far from clearly defined, often considered more akin to the “art” than the “science” of medicine. 1 In Australia, if there is a standard, it is defined by the Royal Australian and New Zealand College of Psychiatrists through the training curriculum and instructions for the college exams, 2 although these provide only broad guidance. In this context it is useful to review a foundation of the psychiatric interview, George Engel's “hypothesis-driven interview”, 3 relate it to current trends in medical interviewing, and reflect on its relevance to conducting a contemporary psychiatric assessment.
The focus of the hypothesis-driven interview is an exploration of “what is wrong” and “how this came about”. 4 This is achieved by raising and testing hypotheses in the process of building a biopsychosocial formulation, and determining the most likely diagnostic hypotheses. In the service of this task, the doctor–patient relationship is nurtured and the patient encouraged to “tell their story”. 3 Elements of the hypothesis-driven interview are shown in Box 1. The advantages of this approach are seen to be improved validity, “getting to the real problem”, and an inherent efficiency in concentrating on the central dilemma and its antecedents. These concepts presaged current trends in medical interviewing and, by association, the contemporary psychiatric assessment. 5
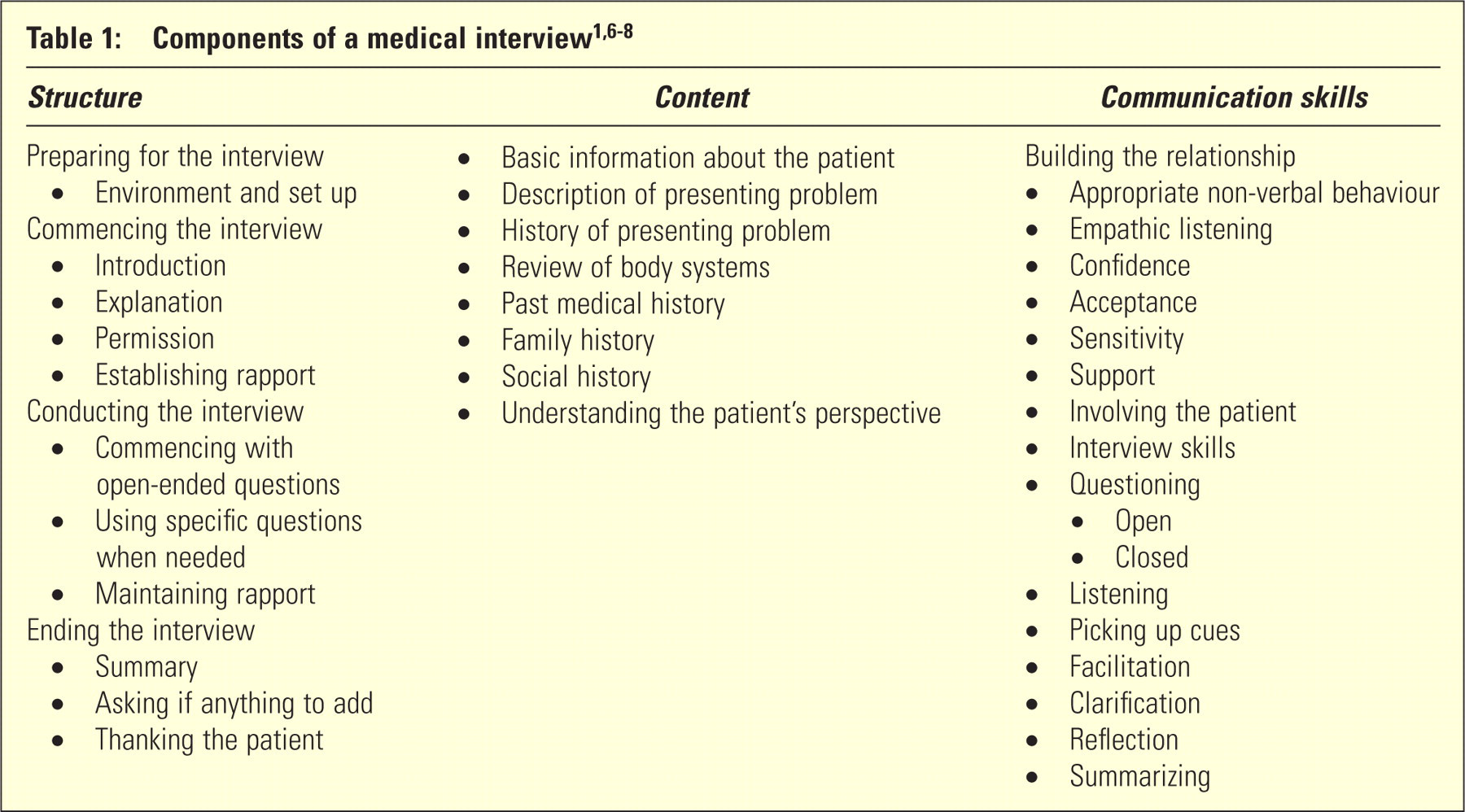
In the modern medical interview, distinction can be made between the aims, the structure, the information collected, and the skills used to elicit that information 6 (Table 1). The aims are commonly cited as (i) to develop and maintain a therapeutic relationship, 7,8 and (ii) to elicit the necessary information to make a diagnosis. 7–9 To these, some authors have added (iii) to provide information, 8,10 and (iv) to manage the patient's problems. 7 The structure of the interview acknowledges the importance of the beginning and end of the interaction, as well as suggesting an order in which information is collected. The skills used to achieve these aims fall under the rubric of “communication skills”, which entered medical education in response to a public perception that doctors did not communicate effectively. 11 A key strategy in communication skills is supporting a narrative, “allowing the patient to tell their story”, 6 facilitated by the use of “open-ended questions”, “listening” and “picking up the cues”. The application of these skills has been shown to lead to greater validity, improved rapport, and decreased physical and psychological distress. 12 Enhanced communication has also been positively related to improved illness outcomes, and to increased satisfaction among patients and physicians. 12 By way of contrast, poor communication has been related to malpractice suits and patient decisions to leave practices. 13
Box 1: Elements of the hypothesis-driven interview
A more recent development in the medical interview has been the articulation of diagnostic reasoning. 14 Applying this method, the initial task of the interview is problem identification. For each problem, diagnostic hypotheses are then generated (differential diagnoses), data methodically collected (hypothesis evaluation and analysis) and, finally, the significant clinical findings are organized, synthesized, and prioritized (hypothesis assembling). 15 Transcripts of physicians thinking aloud have revealed a vocabulary of clinical reasoning, a sequence of iterative steps, and the application of analytic and non-analytic processes. 16 Analytic reasoning approaches, often used by novices, include Bayesian reasoning (probabilistic), 17 causal reasoning (often bioscience based) and deterministic reasoning (rules based). 14 Working diagnoses are made only after they are assessed as adequate in explaining all positive, negative, and normal clinical findings, and for their pathological coherence. 17 Non-analytic reasoning is used mainly by expert clinicians and is a rapid process most akin to pattern recognition. 16,17
The psychiatric interview shares many features with the contemporary medical interview. 5 If there are differences, they relate to the nature of the patient being interviewed, the focus on mental illness, and the additional aim of building a formulation. 5 Although not unique to patients with psychiatric disorders, the psychiatric interview is often made more difficult by the patient being unable to articulate the true nature of their problem, by employing defences to protect them against new insights, or by being impaired in their capacity to share a common reality. The focus on mental illness directs attention to symptoms described in emotional, rather than physical terms, requiring additional vocabulary. The formulation is a unique product of the psychiatric interview. It is an explanatory hypothesis, commonly delivered in a biopsychosocial framework. It addresses the question, “Why does this patient suffer from this (these) problem(s) at this point in time?” 18 If successful, the formulation underpins the development of an individualized management plan promoting a range of therapeutic strategies.
The methods described in the hypothesis-driven interview complement the contemporary medical interview and appear well suited to the specific challenges of the psychiatric assessment. The first key element is building rapport. Rapport refers to the presence of trust, mutual understanding and emotional attunement in the relationship. 19 It is enhanced by using communication skills such as non-judgemental acceptance, acknowledgement, empathy, and offers of partnership and care 11,20 . In the hypothesis-driven interview, the collaborative exploration of the patient's problem increases their experience of being understood, further enhancing rapport. In addition, there is identification and management of the transference and counter transference in order to maintain a positive alliance. This awareness may also aid in the development of the formulation, through the assumption that aspects of the doctor patient relationship may reflect relationships in other areas of the patient's life.
The form of “letting the patient tell their story” adopted by Engel was termed “associative exploration”. 4,21 The interviewer strives to avoid disruption of the patient's train of thought and resists the urge to “prematurely impose his ideas”. 4 The associations which emerge are the sentinel clues to the patient's real concerns and precursors to the hypotheses. The interview then progressed by investigating these concerns “formulating each successive question on the basis of what the patients has just said”. 4 Communication skills (listening, picking up cues, facilitation) are used in this process, not only to build rapport, but to develop a collaborative understanding of “the world as the patient would see it”. The interviewer is less a practitioner extracting information or even just encouraging the patients to speak freely, but rather a partner, “sitting on a bench”, helping to describe the world they see together. This skill extends beyond empathic attunement, as it requires the interviewer to concurrently engage the patient on an emotional level, but at the same time observe the patient, themselves and the relationship “from the outside”, a concept not dissimilar to Ogden's notion of the analytic third. 22
The formulation is developed through building and testing hypotheses. These hypotheses are speculations in the psychological as well as the pathophysiological realm. As each hypothesis is raised in the mind of the interviewer, it is pursued in a way similar to diagnostic hypothesis evaluation and analysis. The hypothesis is “assembled”, put to the patient and their response gauged. This may require little more than clarifying the order of events. Alternatively, it may require re-exploration and development until it develops “psychological coherence” and becomes a formulation. The capacity to develop a formulation will differ between practitioners. It requires the ability to “stand in the shoes of the other”, as well as a practical understanding as to how different people respond to common challenges. This understanding is often informed by a wide array of theories 23 , and is developed through clinical and life experience. This capacity, although to some degree innate, can be fostered through identifying each clinical interaction as an opportunity to build a greater knowledge of “the way things go”, and a commitment to self-reflection and personal growth.
Elements of the hypothesis-driven interview are illustrated in a simplified and de-identified example:
Sarah is a 37-year-old single lady admitted to hospital for nasogastric feeding in the context of a chronic malabsorption syndrome. The written referral requests an “assessment of depression and competence”. The verbal referral includes concerns that she is refusing feeding which may be life threatening.
“Close the door”. (Preparing the environment)
“Good morning. My name is Dr George”. (Introduction)
“I have been asked to see you to see if we can better understand how your condition may be impacting you”. (Explanation)
“Is that alright?” (Permission) – “Yes”.
“I guess you are a bit tired of having to tell your story over and over” (Building rapport, hypothesis based on chronic illness) – “A bit”.
“I wonder if you could say a little about how things have been going”. (Commencing with open-ended questions) – “It has been a long year. There is work, my illness and my father dying. I think I have managed pretty well. It is hard to deal with it all together. I work for three days, then have all these appointments and admissions. I feel like I just need a break from it”. (Sentinel cue) “I have run out of sick leave. The last time I came in I was supposed to see two specialists, but I did not see any.” (Provisional hypotheses relating to refusal to have Naso-gastric (NG) feeds: (1) related to depression and grief; (2) a covert eating disorder; (3) “needs to have a break” in the context of chronic illness and difficulties in her relationship with the treating team).
“Your father passing would have been very difficult. Can you say a little about how it felt, how it feels” (Exploring grief) – “Sometimes when you see things that remind you of him you feel, ah, you know. But otherwise I have felt OK”.
“You mentioned the difficulties you face relating to your illness and wanting a break” (Testing hypothesis, building rapport through identification and reflection of “sentinel cue”) – “They want me to come in and have the feeding. I understand that being underweight increases my risks, but they do not understand what it is like to use all this time and then nothing happens” (Evidence to support the hypothesis relating to difficulties in the doctor–patient relationship)
“The unit don't seem to understand the impact and control the treatment has over your life” (Reflecting back the hypothesis) – “No they don't, but I do not let it worry me.” (Interviewer experiences hostility, which is disowned by the patient – is this a reflection of the nature of the relationship with the treating team?).
“Can you say a little about your childhood and upbringing?” (exploring developmental antecedents of her current relationships) – “It was normal, fine. No problems. My parents weren't around much. They both worked and pretty much left us to our own devices”
“They were not as engaged as you would have like them to be.” (Testing hypothesis that significant others were experienced as inattentive) – “I guess, but they were alright, they were just busy” (Acknowledges disappointment, but resists criticism)
“It seems that in the past and even now you have struggled with having to run to someone else's timetable” (testing the formulation) – “Yes, that's why I just want a break”.
A final formulation is as follows:
Sarah is a 37-year-old single lady presenting with the problem of refusing recommended treatment. She describes limitations resulting from her illness and disappointment with failed commitments by the treating team. She does not describe symptoms of major depression or anorexia nervosa. Her developmental history is notable for an experience of her parents as busy and absent. Putting this together, we may hypothesize that her refusal to take treatment arises out of her frustrations with the treating team which resonate with her earlier developmental experiences. As with her parents, she is unwilling to voice these complaints, leading her to act them out.
CONCLUSION
The hypothesis-driven interview shares much with the contemporary medical interview. In addition it provides a rationale and method for the application of communication skills and allows the interviewer to build a formulation during the course of the interaction. This approach allows diagnostic reasoning and the narrative approach to occur concurrently, processes which have been thought by many authors to be incompatible. To do this, however, requires the real time ability, to collect, collate and analyse both bio-medical and psychological data, a skill which is grown during a long period of apprenticeship. Consequently, interview skills need be as much a part of advanced training as at the introduction to clinical practice. This already occurs in psychiatry training, but may also be the case for other branches of medicine.
A key focus of the psychiatric interview, the formulation, is not beyond criticism. The primary concern is one of validity. In theory, any number of plausible explanations can be formulated for the presenting problem, with no objective standard available to determine which is correct. In reality, no formulation is going to be fully correct, although some are better than others at bringing the information together and promoting an effective management plan. If the aim then is for the psychiatric interview to generate a formulation that is plausible and useful, the hypothesis-driven interview is one method well suited to this aim.
The interview will continue to evolve, adapting to changes in patient expectations, medical knowledge and the use of language in specific roles. That said, the task of collecting valid information within a working alliance will remain central. Our success in this is informed by the heritage of clinical practice. The hypothesis-driven interview is an important part of that heritage and is one articulation of the “art” of medicine.
DISCLOSURE
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.