
Abstract

Introduction
Arthrodesis is the current standard treatment for various first metatarsophalangeal (MTP) joint pathologies and a salvage procedure for failed first MTP joint replacement, with an overall successful fusion rate of 95%. 2 Treatment options, such as first MTP arthroplasty for arthritis, have a high rate of complications, including component loosening. 1 Despite the widespread successful fusion rate of arthrodesis, in general, salvage of failed implants is more difficult. Mann et al. 2 found that only 68% obtained excellent or good results.
Various methods of fixation have been described in arthrodesis procedures. We describe an arthrodesis technique utilizing a 4-hole, 1/3 semi-tubular plate as a salvage procedure after failed first left MTP hemiarthroplasty (Figure 1). In order to obtain additional purchase in the bone, aside from the 4 holes in the plate, two 1.7-mm screws were placed in the Kirschner wire positioning holes. These 2 additional holes allowed us to obtain 4 cortices of additional fixation. The patient went on to have a well-positioned fusion of the first MTP joint.
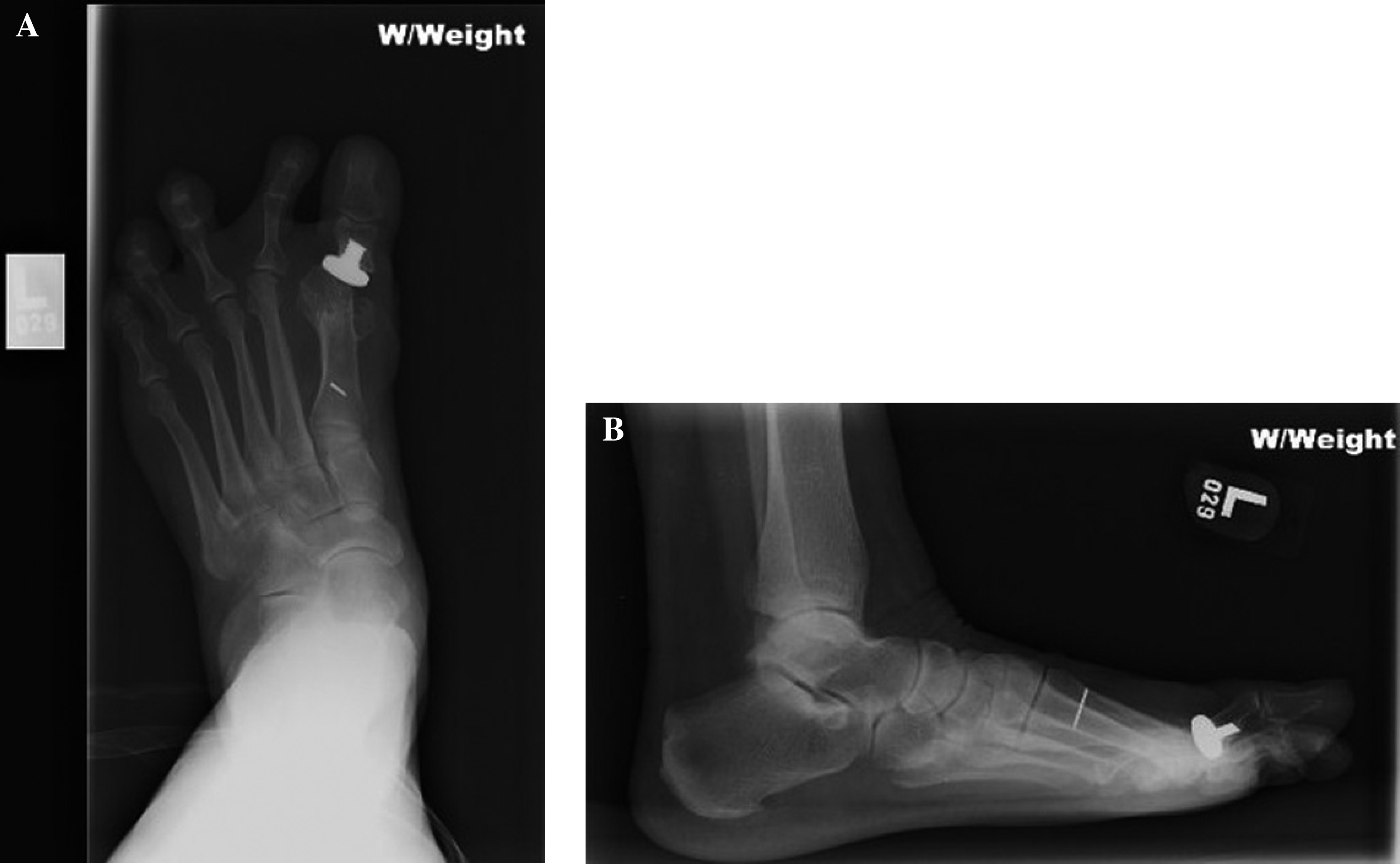
Anteroposterior (A) and lateral (B) views of the left foot demonstrating the failed hemiarthroplasty of the first MTP.
Operative Technique
An incision was made on the dorsal aspect of the first left MTP joint in the same location as the prior dorsal incision. The incision was carried through the subcutaneous tissue, and the extensor tendons were freed up and retracted laterally. A dorsal capsulotomy was then created over the head of the first metatarsal. The hemiarthroplasty component and the joint space were identified and the scar tissue was removed with a rongeur.
Dorsal subluxation of the proximal phalanx was evident. Using an osteotome, the joint space was pried open. A Cobb was placed into the first MTP joint in order to reduce the proximal phalanx and the hemiarthroplasty was removed. Using a sagittal saw, the remaining subchondral bone on the distal portion of the first metatarsal head was trimmed. The base of the proximal phalanx was also resected so that the subchondral bone of both the proximal phalanx and the first metatarsal, when opposed, left a residual valgus of 10 degrees and dorsiflexion of 15 degrees, in relation to the first metatarsal.

Intraoperative photograph demonstrating the 4-hole, 1/3 semitubular plate, with the four 3.5-mm screws in place, and the 2 Kirschner-wire holes.

Anteroposterior (A), oblique (B), and lateral (C) views of the left foot demonstrating the final fusion construct 10 weeks postoperatively.
A complete synovectomy was performed. The shortened hallux was then stretched out to a more normal length. The subsequent defect where the prosthesis had been located measured approximately 1.5 cm. Tricortical iliac crest bone was then harvested in the usual fashion. It was contoured to recreate the functional position of the first MTP, while restoring the length of the first ray. A 5-hole plate was felt to be too large and would place the screw holes in an incorrect location. Therefore, a 4-hole, 1/3 semitubular plate was used for the fusion. The plate was placed over the first MTP joint, spanning the proximal phalanx, iliac bone graft and the metatarsal head. Four 3.5-mm cortical screws were placed, one in the proximal phalanx, one in the iliac crest bone graft, and two in the distal aspect of the first metatarsal (Figure 2). It was felt that additional fixation was necessary, therefore two 1.7-mm screws were placed in each of the Kirshner-wire holes. Of the 2 screws, the distal screw was placed in the proximal phalanx and the proximal screw was directed into the metatarsal. This provided 6 cortices of fixation proximally and 4 distally (Figure 3).
The wounds were thoroughly irrigated and closed with 3–0 silk sutures. Sterile dressings were applied. The patient was made nonweightbearing for 4 weeks. Thereafter, the patient was allowed to fully bear weight in a postoperative shoe. Ten weeks following the surgery, the patient was allowed to wear a normal shoe. The patient was seen weekly for the first 8 weeks to perform weekly bunion dressing changes, a standard care for this procedure used instead of a short leg nonweightbearing cast.