
Abstract
Background: The Krackow locking loop technique has been used for Achilles tendon repair with documented success in allowing early range of motion with stable fixation. Previous studies documented failure at the rupture site by knot failure. We propose a modification of the traditional Krackow technique where the knots of the suture are tied away from the rupture site (aka the Giftbox technique). We compared the tensile strength of Achilles tendons repaired using the traditional Krackow technique with those repaired using the Giftbox technique. Materials and Methods: Thirteen pairs of fresh frozen cadaveric Achilles tendons were harvested. An Achilles tendon rupture was created 4 cm from the calcaneal insertion. Thirteen Achilles ruptures were repaired using the traditional Krackow technique and 13 pairs were repaired using the Giftbox technique. The Achilles tendons were then tested to failure as defined as a gap of 1 cm. Results: The mean force to failure for the tendons using the Giftbox technique was 168 N, whereas the mean for the traditional Krackow technique was 81 N (p < 0.0001). Conclusion: Based on our biomechanical study, Achilles tendons repaired using the Giftbox technique are more than twice as strong as those repaired using the traditional Krackow technique. Clinical Relevance: We recommend the Giftbox modification to minimize gap formation and improve the strength of the repair of a ruptured Achilles tendon.
Introduction
Achilles tendon ruptures are common injuries among young and middle-aged individuals. They occur in the third to fourth decade of life, mostly in men, and have an annual incidence of 18 to 37 cases per 100,000 persons. 6 Achilles ruptures usually result from non-contact injuries resulting from mechanisms including forceful push-off of the foot with an extended knee, sudden unexpected ankle dorsiflexion, or violent dorsiflexion of a plantarflexed foot. 19 Despite recent attention to surgical treatment of Achilles ruptures, the decision to treat these injuries surgically versus nonoperatively remains controversial. 2,4,12,13 Nonoperative management historically is associated with a high risk of re-rupture, ranging from 13 to 30%, but no wound complications. Operative management of Achilles tendon ruptures results in a lower re-rupture rate (0 to 6%), early mobilization, and better return to sports 7 but with the risk of wound complications (0 to 21%). 1 -4,9,10,12,13,22,23
The goal of surgical management is early mobilization which maximizes healing potential. 5,20 This requires strong suture material and a sound technique. 17 Currently, several suture techniques exist for repairing acute Achilles tendon ruptures. These include the Krackow, Kessler, Bunnell, and the triple bundle technique. 2,8,11,14,20,24 Prior studies have demonstrated that the Krackow repair is stronger than the Kessler or Bunnell. 26 The Krackow locking loop has been used for tendon repair with documented success in allowing early range of motion with stable fixation. 14,15,20,21,27 Jaakkola et al. showed that a triple bundle repair was stronger than the Krackow. 11 A portion of the improvement in strength was thought to be due to increased suture strands across the repair site which may also be a source of vascular compromise. 11 They also suggested that tying the knots at the rupture site could lead to increased stress and early failure; consequently, they suggested tying the knots away from the rupture site. 11
We propose a modification of the traditional Krackow technique where the knots of the suture are tied over the cross-limb of the counter suture. We liken this to the crisscross pattern of wrapping a Giftbox and therefore refer to this technique as the Giftbox technique. We performed a biomechanical study to compare the tensile strength of Achilles tendons repaired using the traditional Krackow locking loop technique with those repaired using the Giftbox technique. Our hypothesis was that tying the suture ends over the cross-limb of the counter suture would increase the force required to produce a gap at the injury site.
Materials and Methods
Twenty-six fresh frozen cadaveric Achilles tendons (13 pairs) were harvested from lower limbs that included the knee. There were eight female and five male specimens with an average age of 88 (range, 76 to 95) years. There was no evidence of previous injury to the Achilles tendon or fracture of the calcaneus. The tendons were harvested from just proximal to the musculotendinous junction to the Achilles insertion, including a block of calcaneal bone. The calcaneal block was approximately 1.5 cm wide, 3 cm long, and 1.5 cm thick.
Similar to previous experiments, 11,26 a tendon rupture was simulated by a transverse incision of the tendon with a scalpel approximately 4 cm proximal to the calcaneal insertion. For each pair, one tendon was placed in the traditional Krackow group while the other was placed in the Giftbox group, with left and right tendons alternated in successive pairs. All tendons were repaired with No. 2 fortified polyester non-absorbable suture (Hi-Fi™, ConMed Linvatec, Largo, FL). For both groups, the locking elements of the suture were placed along the medial and lateral edges of the tendon. There was no slack in the suture as it was placed. Each repair included four locking loops that were approximately 4 mm apart. All specimens were tied using five square knots. The same surgeon (RHR) carried out all the repairs.
Unlike the traditional Krackow technique where the transverse limb crosses over the tendon tissue, the transverse limb of the Giftbox group was placed in the middle of the tendon as it transitioned from one side to the other. Knots were tied at the rupture site for the traditional Krackow group (Figure 1). For the Giftbox group, Keith (straight) needles were used to pass the free suture ends across the rupture site on to the opposite end of the tendon. Sutures emerged one superficial and one deep to the transverse limb of the opposite Krackow suture. In addition, both sutures were passed through the tendon emerging on the superficial surface of the tendon. Thus, four suture strands were passed across the rupture site and all sutures were tied away, proximal and distal, from the repair site (Figure 2).
Biomechanical testing
Distally each calcaneal bone block was fixed with three pins to a bone clamp. The proximal ends were fixed to a soft-tissue clamp. The fixation was reinforced on both ends of the Achilles tendon with a mechanical “C” clamp. Each tendon, in its clamps, was placed into a Mini Bionix Servohydraulic load frame (MTS Systems, Eden Prairie, MN) (Figure 3). The tendons were loaded to failure at an extension rate of 2.54 cm/s. Failure was defined as gap formation of 1 cm (as measured by digital micrometer) at the rupture site. This extension rate of 2.54 cm/s was determined in prior studies and is within the range of rates imposed on the Achilles tendon during the physiologic range of motion. 11,26 The load cell used to measure the applied force had an accuracy of 1 N.

Traditional Krackow technique - Suture knots are placed at the site of repair.
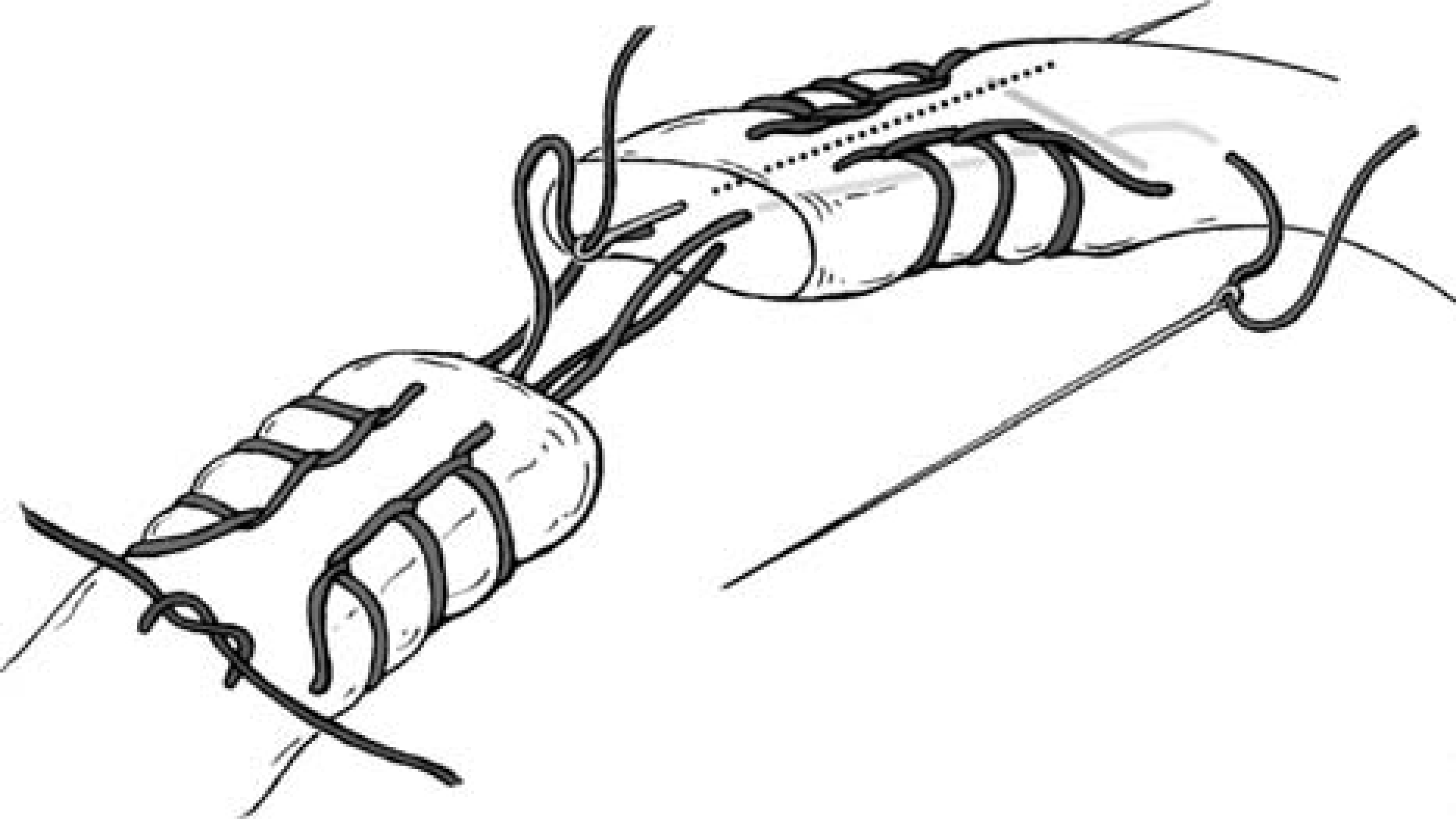
The Giftbox technique - Sutures should emerge one superficial and one deep to the transverse limb of the opposite Krackow suture. Note that the sutures are tied distal to the cross-over stitch of the other suture.

Testing apparatus.
Statistical methods
The Shapiro-Wilk test was used to test the normality of the force to failure for the Giftbox technique and the Krakow technique, as well as for the difference in the force to failure between the pairs. Means, standard deviations and 95% Confidence Intervals were reported to describe each of these outcomes. A paired t-test was used to test whether there was a significant difference between the Giftbox and the traditional Krackow techniques using a two-sided alternative and 0.05 level of significance.
Results
The Shapiro-Wilk tests suggested the assumption of normality was reasonable for all these outcomes, since all the p values were well above the 0.05 cutoff.
The mean force to failure for the tendons using the Giftbox technique was 168 N (95% CI 133, 204 N), whereas the mean for the traditional Krackow technique was 81 N (95% CI 70, 91 N), and the mean for the difference between the Giftbox and the traditional Krackow is 87 N (95% CI 55, 120 N) (Figure 4).
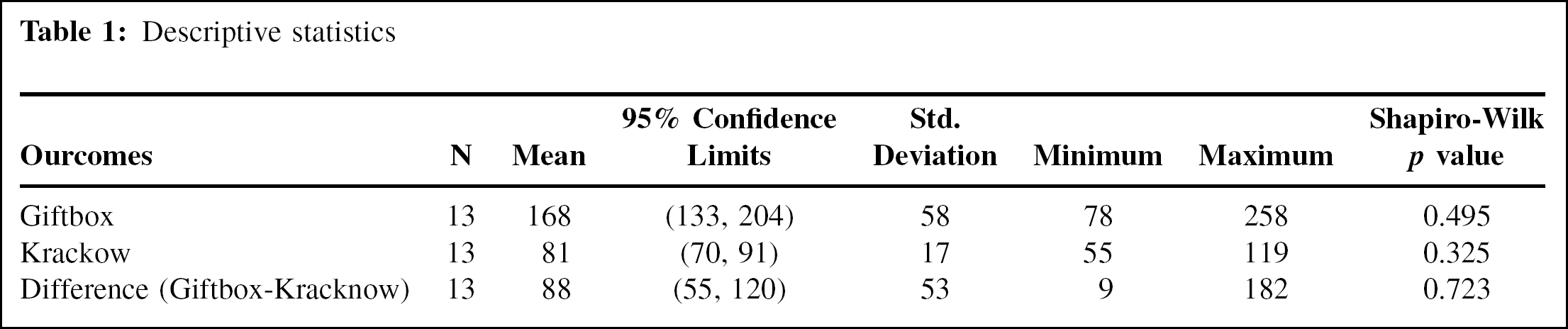
These results suggested an increase in the force required for gap formation based on the Giftbox technique as compared to the traditional Krackow technique ranges from 55 to 120 N. All 13 pairs revealed that a larger tensile force was required to produce a 1 cm gap in the Giftbox technique as compared to the traditional Krackow technique, with the range being from 9 to 182 N (Table 1).
The paired t-test showed a highly significant difference between the Giftbox and traditional Krackow techniques with a p value based on the t-distribution with 12 degrees of freedom at p < 0.0001 (test statistic t = 5.913).
Discussion
We found that the load to failure of the traditional Krackow repair was increased more than two-fold by adding the Giftbox modification. It is our contention that the Giftbox technique reduces gap formation by increasing the number of strands across the repair site and increasing tendon pullout at the suture-tendon interface. As the number of strands increase over a rupture site, the strength of repair improves. 25 However, as suggested by Jaakkola et al., 11 increasing the number of strands may also compromise tendon vascularity and healing potential. Compared to the triple bundle technique, the Giftbox technique decreases the number of strands that cross the rupture site and may limit vascular compromise during the repair. Also, tying sutures at the repair site may set up a stress riser resulting in earlier failure at the knot. 11 In addition to placing knots away from the repair site, the Giftbox technique also loops the sutures around the counter suture's transverse limb, thus possibly adding to the increase in strength.
Our study may have some limitations. As stated previously by Labib et al., 16 our model is one in which the tendon has been transected rather than ruptured. Transected tendon may hold suture better than a ruptured tendon where the ends are frequently fibrillated. However, this model is similar to other studies of repair strength in the literature and was adopted because it was easy to reproduce and thus facilitate study comparison. 11,16,26 Another problem with our study is that the average age of the cadaveric Achilles tendons was 88 years. Achilles tendon ruptures typically occur during the third and fourth decades of life. One could propose that the tissue quality of older specimens may be compromised secondary to the donor's advanced age. With younger cadavers, we may have attained a higher force at rupture that may have reached a critical point for knot failure. However, our values of force to rupture are similar to those of Cretnik et al. 8 who used specimens from adults in the age range of 30 to 50 years.
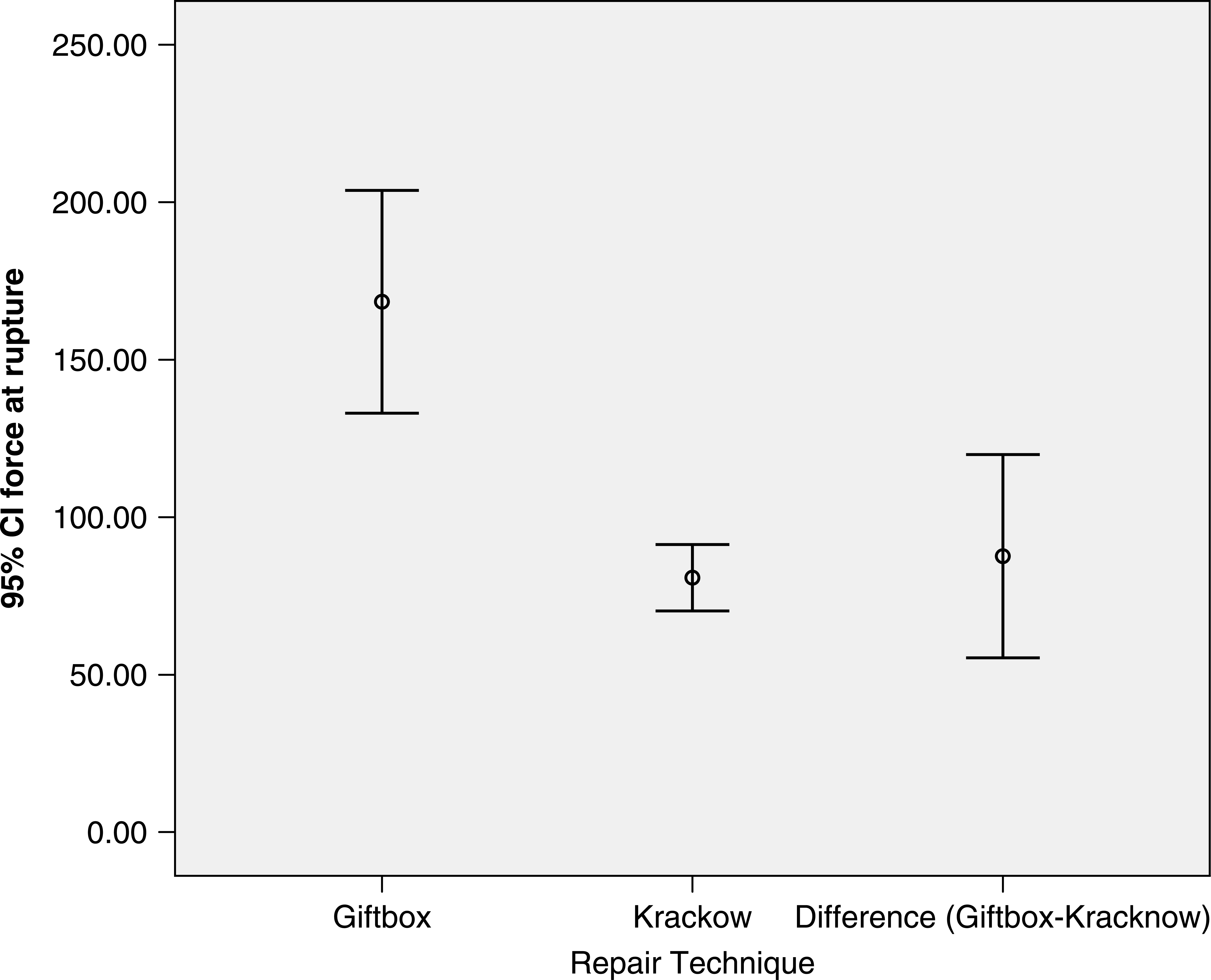
Error plots with the mean and the 95% Confidence Interval.
Descriptive statistics
We believe that the Giftbox technique is a simple and relatively quick method without constricting additional tissue during the repair. Additionally, with the demonstrated increased strength, the Giftbox technique may add to our ability to perform earlier mobilization of the tendon thus potentially improving healing and range of motion. We are currently prospectively following patients who have had their Achilles tendons repaired using the Giftbox technique. We will be comparing functional outcomes with historical standards with regard to early rehabilitation and re-rupture rates. Based on our biomechanical study, Achilles tendons repaired using the Giftbox technique are more than twice as strong as those repaired using the traditional Krackow technique. At this point, we believe that the Giftbox modification minimizes gap formation and improves the suture strength of the repair.
Editor'S Note
The authors are to be commended for a nice biomechanical study. One concern regarding the results is the acute failure model. Of at least as much concern as catastrophic failure after surgery is stretching of the repair as it is gradually stressed during rehabilitation. Cyclic, subfailure testing may be helpful to clarify the fatigue strength if a future investigation is performed. Also, clinically, it may be somewhat challenging to get the tendon ends properly opposed when the knot is being tied at a distance from the rupture site. Their proposed clinical study will help to determine if this technique is more technically difficult to perform in a ruptured, rather than a transected, tendon.