
Abstract
Background: The aim of operative treatment for ankle fractures is to allow early movement after internal fixation. The hypothesis of this study was that early mobilization would improve functional recovery in patients after surgery for ankle fractures. Methods: In a prospective randomized controlled study, 66 consecutive patients with ankle fractures that required open reduction and internal fixation (ORIF) were assigned to one of two postoperative regimens: immobilization in a nonweightbearing below-knee cast or early mobilization in a removable cast. Four patients were excluded from the study, leaving 62 for review. Results: Patients who had early mobilization in a removable cast had higher functional scores (Olerud-Molander and AOFAS) at 9 and 12 weeks postoperatively. They also returned to work earlier (67 days) compared with those treated in nonweightbearing below-knee cast (95 days), p < 0.05. There was no statistical difference in Quality of Life (SF-36 Questionnaire) at 6 months between the two groups. We had an approximately 10% postoperative infection trend (one superficial and two deep) in the early mobilization group. Conclusion: Despite the overall short-term benefit of early mobilization, we had three patients in the early mobilization group who had wound complications. Both the surgeon and patient should be aware of the higher risk of wound complications associated with this treatment, and thus the accelerated rehabilitation protocol should be individualized.
INTRODUCTION
Controversy still exists regarding the best treatment after internal fixation of an ankle fracture. The Association for the Study of Internal Fixation (ASIF) recommended early active pain free mobilization of muscles and joints adjacent to the fracture for the prevention of “fracture disease”. 19 According to the AO/ASIF group, the goals of open reduction and internal fixation (ORIF) of ankle fractures include anatomic restoration of the mortise with stable fixation and early active pain-free mobilization. 20,24 The theoretical basis for the use of functional treatment in orthopaedic practice is the fact that early weightbearing and the avoidance of complete immobilization have been shown to facilitate the restoration of range of motion of the injured joint, to decrease swelling and the development of soft-tissue atrophy, and to prevent the development of osteoporosis. 10,11,18,21 Various studies in the literature have compared different types of postoperative regimens after ankle surgery, with contradictory results and recommendations. Previous clinical studies have shown clear beneficial effects of early postoperative mobilization on functional outcome, at least in the short term, for internally fixed ankle fractures. 2,3,4,6,25,26 The benefit of early mobilization in an ankle brace was objectively shown in one study by isokinetic muscle strength measurements. 27 This has led several authors to recommend early mobilization and functional treatment. 1,2,3,4,6 Other authors concluded that early mobilization after ankle surgery did not influence the clinical outcome and made no specific recommendations regarding postoperative regimens. 5,7,8,9 Interestingly, in a prospective, randomized study Lehtonen et al. 14 reported an unacceptably high rate (66%) of wound complications with immediate (day one) postoperative mobilization in a functional ankle brace. They recommended caution in the early use of a functional brace in the immediate postoperative period after internal fixation of an ankle fracture.
In view of the existing conflicting evidence, the aim of our study was to assess the short-term effect of early mobilization on the functional outcome of internally fixed ankle fractures. This is the first prospective, randomized controlled study to compare subjective and objective, short-term outcome measures in patients who had early mobilization in a removable cast after primary wound healing compared to those in patients who had immobilization in a below-knee cast for 6 weeks (both groups being nonweightbearing).
MATERIALS AND METHODS
Patient Selection
Sixty-six consecutive patients with acute, closed ankle fractures that required ORIF between August, 2004, and March, 2005, were included in the study. They were all young and active patients, and their enrollment into the study was based on strict inclusion and exclusion criteria (Table 1). All patients were informed of the study procedure and the purpose of the study and all gave informed consent. The study was conducted in conformity with the principles of the Helsinki II Declaration and was approved by the Committee of Ethics on Human Research in our hospital. Of the patients who were initially included in the study, four were later excluded or lost to followup: one moved abroad, one did not return for followup visits, and two were noncompliant with either the weightbearing status or exercise program. All patients who were enrolled in the study were treated operatively with standard ORIF according to AO/ASIF methods. 23 Prophylactic intravenous antibiotics were given preoperatively to all patients. After the operations, patients were randomly assigned, using their odd or even day of date of birth, to one of the two postoperative regimens: early nonweightbearing mobilization in a removable cast and nonweightbearing immobilization in a below-knee cast for 6 weeks.
Inclusion and exclusion criteria used for enrollment of patients into the study

There were 62 patients between the ages of 16 and 65 years who completed the followup examinations. Baseline characteristics (age, gender, body mass index, occupation and level of activity), mechanism of injury, classification of fractures (Weber 29 and Lauge-Hansen 13 ) and rate of dislocation in the two groups are presented in detail in Table 2. The two different groups, G1-nonremovable cast and G2-removable cast and early mobilization, were comparable when assessed through the outlined baseline parameters.
Baseline characteristics of the patients.
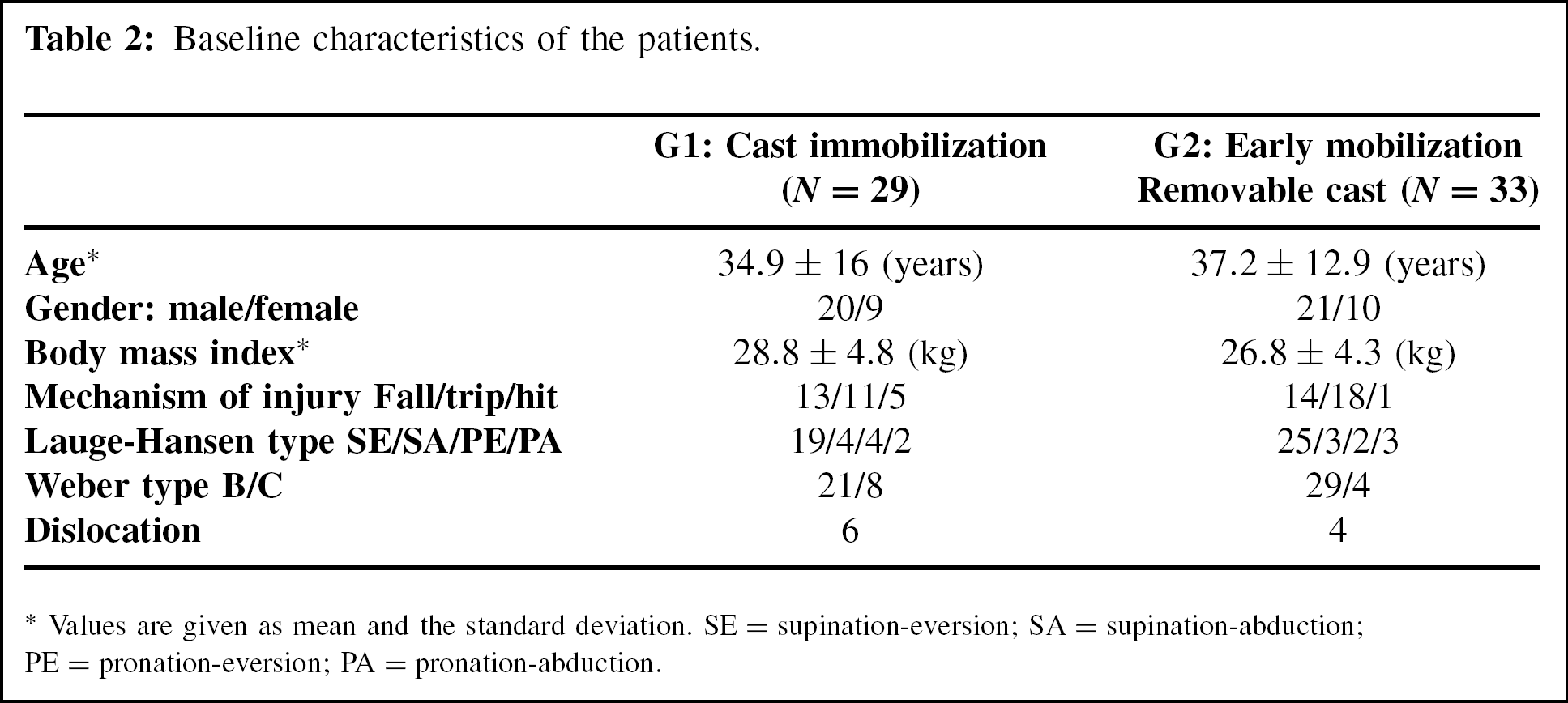
Values are given as mean and the standard deviation. SE = supination-eversion; SA = supination-abduction; PE = pronation-eversion; PA = pronation-abduction.
Postoperative Management
Both postoperative regimens consisted of an initial period of 10 to 14 days in a dorsal plaster of Paris splint with the ankle in neutral position until primary wound healing occurred and skin sutures were removed. Both groups used crutches and were nonweightbearing.
Group one (G1) included 29 patients who wore a below-knee, nonremovable fiberglass cast nonweightbearing for 6 weeks postoperatively. Group two (G2) included 33 patients who after removal of sutures were treated in a custom-made removable fiberglass cast (Figure 1). They also were nonweightbearing and were exercising the affected ankle three times a day, for 10 min. An exercise program consisted of active and passive range-of-motion exercises of the ankle and subtalar joint without the brace (flexion, extension, circumduction, inversion and eversion—open and closed chain exercises) under the supervision of a certified physiotherapist. The cost of the physiotherapy was not higher in this group compared to the group with complete immobilization, because patients were seen weekly as outpatients in the physiotherapy department. After 6 weeks, patients in both groups were instructed to partially bear weight with the aid of the crutches and to achieve full weightbearing on the affected ankle without crutches in 2 weeks. After 6 weeks patients in the group with complete immobilization were given a similar exercise program under weekly supervision of a physiotherapist. At 8 weeks postoperatively full weightbearing without crutches was encouraged.
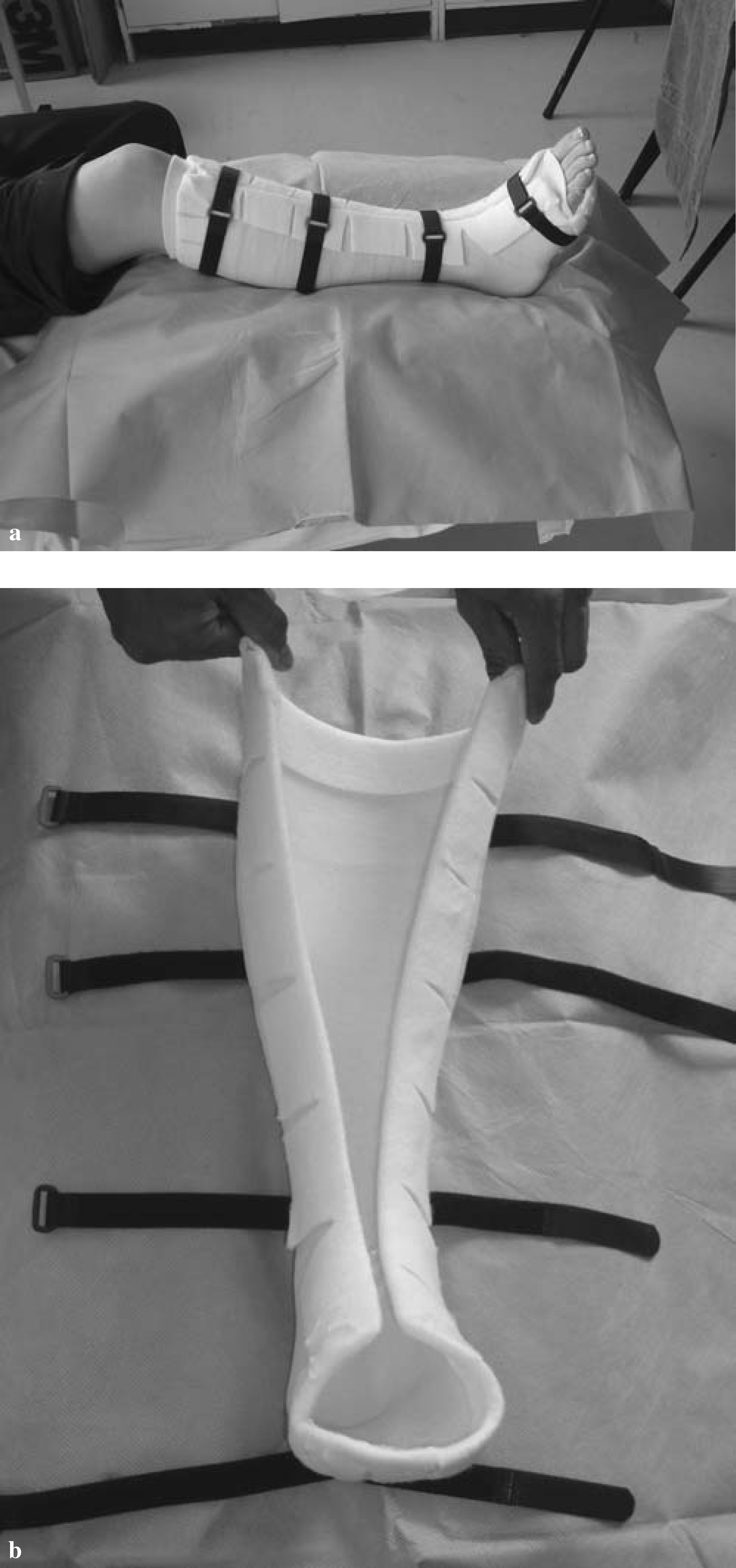
A and B, Custom-made removable fibreglass cast.
Followup Evaluation
Clinical assessment of the patients was performed by one of the authors conducting the study using subjective, objective, and radiographic evaluation criteria at 2, 6, 9, 12, and 24 weeks postoperatively. Standard anteroposterior and lateral radiographs were taken at 2, 6, and 9 weeks to assess fracture healing and alignment of the affected ankle joint. The recorded objective outcome measurements were swelling of the ankle, calf wasting, and range of motion of the ankle. Swelling of the ankle was determined by the difference between the injured and the uninjured leg. The figure-of-eight method for assessing ankle swelling also was used. This has been described as a reliable and valid indirect method of measuring ankle edema. 22 Wasting of the calf muscle was determined by the difference between the injured leg preoperatively and the same leg at 6 weeks postoperatively with respect to the circumference of the leg 10 cm distal to the tibial tuberosity. The measurement of the circumference was proximal to ankle swelling because of fracture or surgery. We believe that the measurements are more reflective of muscle wasting than the swelling. In the group treated with complete immobilization we included two patients who developed deep vein thrombosis (DVT) and had some degree of calf swelling. A goniometer was used to determine the maximal active dorsiflexion and plantarflexion of the operated ankle. Patients' functional recovery was subjectively evaluated using two well-recognized, standard rating systems for the ankle: Olerud and Molander 22 and the American Orthopaedic Foot and Ankle Society (AOFAS) 12 scoring system. Functional scores were obtained at 9 and 12 weeks postoperatively. The time to return to work or to the preinjury activity level was documented for all patients. At 6 months after surgery, a standard Quality of Life, SF-36 questionnaire was sent by mail and completed by the patients.
Statistical Analysis
The data were analyzed with the use of MINITAB, version 13.1 statistical analysis software (Minitab, Inc., State College, PA). As a normal distribution cannot be assumed, the nonparametric Mann-Whitney U test (two samples with correction for ties) was used for quantitative data. Also, a Student t-test comparing mean values and standard deviation was used in presenting the data in the tables. A significance level less than 0.05 was assumed. The study groups were large enough to provide statistical significance of the measurements (ankle swelling, calf circumference, range of motion).
RESULTS
Clinical Assessment
Objective outcome measures, swelling of the ankle, wasting of the calf muscles and active range of motion at the 6 and 9 weeks followup examinations, are shown in Table 3. At 6 weeks there was no statistically significant difference between the two treatment groups when comparing ankle swelling, measured by either the figure-of-eight around the ankle joint or the circumference at the level of the malleoli.
Results data
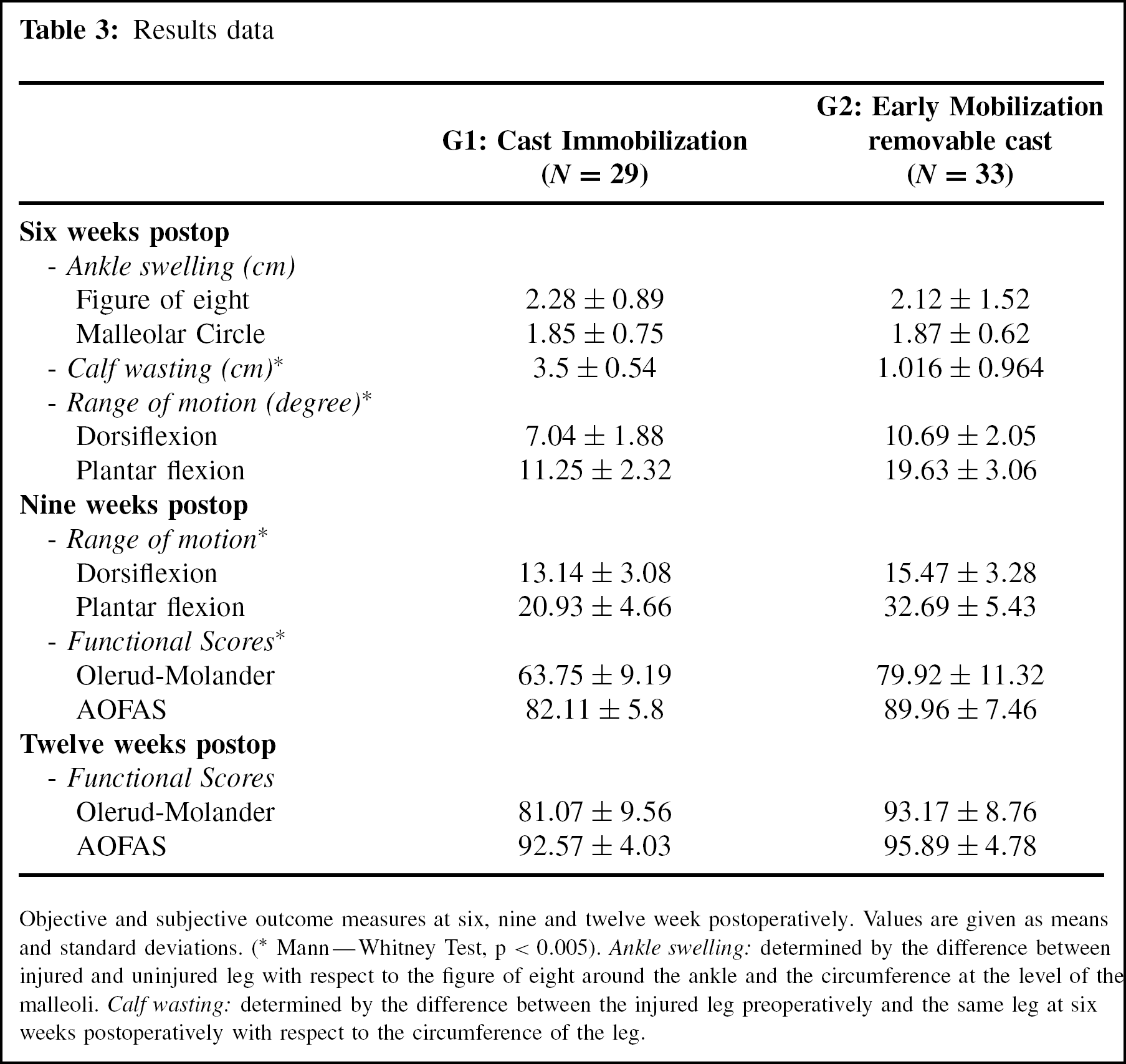
Objective and subjective outcome measures at six, nine and twelve week postoperatively. Values are given as means and standard deviations.
(Mann—Whitney Test, p < 0.005).
Ankle swelling: determined by the difference between injured and uninjured leg with respect to the figure of eight around the ankle and the circumference at the level of the malleoli. Calf wasting: determined by the difference between the injured leg preoperatively and the same leg at six weeks postoperatively with respect to the circumference of the leg.
There was significantly less calf muscle atrophy (approximately 2.5 cm difference), p < 0.005 Mann Whitney test, at 6 weeks postoperatively in patients who had been exercising their ankle when compared with the patients who had been immobilized for 6 weeks. Calf muscle atrophy was appreciated by comparing the circumference of the injured leg 10 cm below the tibial tuberosity measured preoperatively and 6 weeks after surgery. Since swelling of the ankle was not significantly reduced at 6 weeks, we believe that measurement of the leg circumference is more representative of calf muscle atrophy than of decrease in swelling.
As expected, patients in the early mobilization group had better active dorsiflexion and plantarflexion at 6 and 9 weeks, when compared to patients treated with immobilization postoperatively (p < 0.05 Mann Whitney) test. However, as shown in Figure 2, the difference is probably temporary and present in the short-term recovery period, as patients treated with immobilization will improve ankle range of motion once starting and progressing through their rehabilitation program.
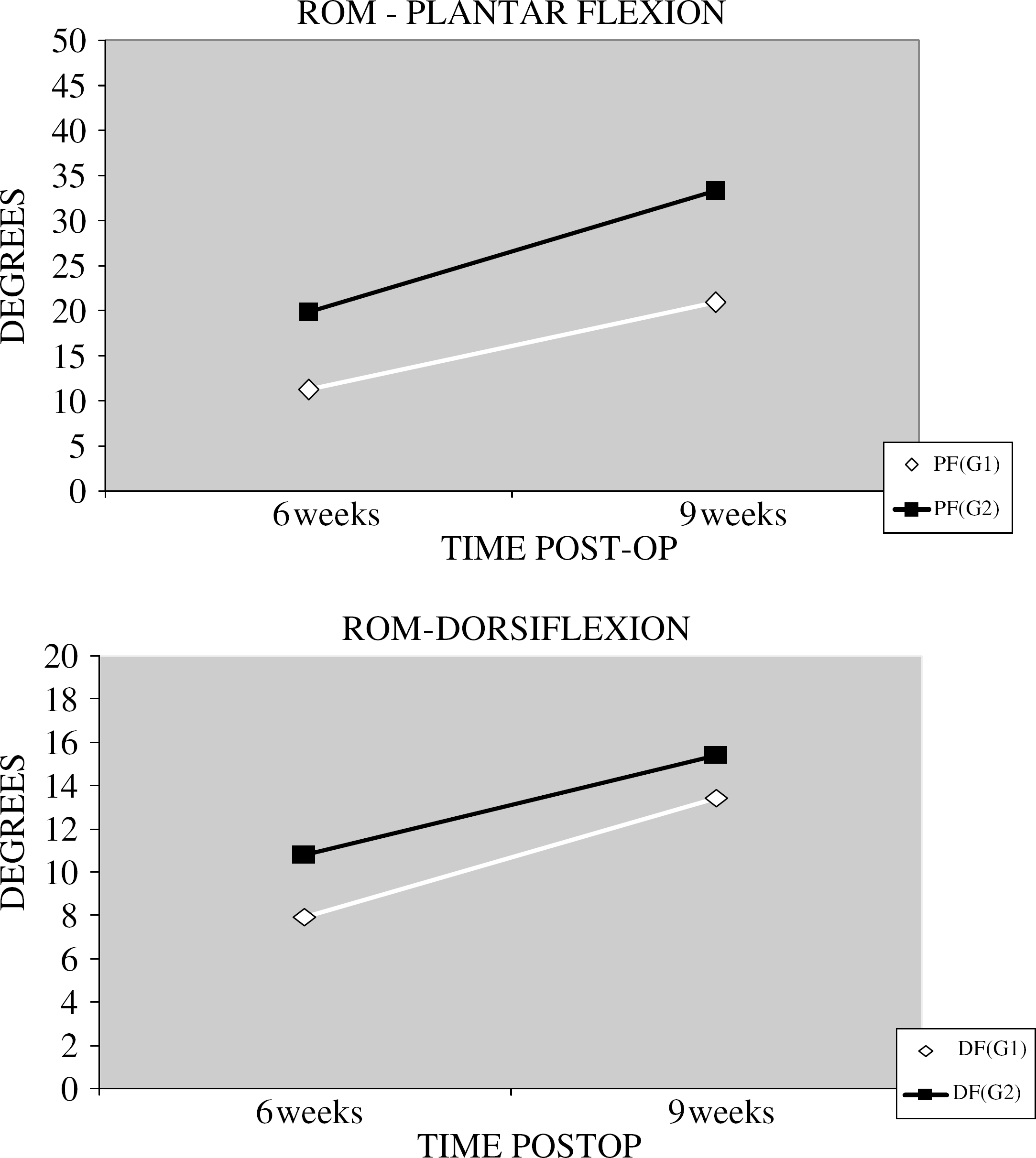
Dorsiflexion and plantarflexion in the two groups at 6 and 9 weeks.
Functional Outcome
Functional recovery, according to the scoring systems of Olerud and Molander and the American Orthopaedic Foot and Ankle Society, is graphically presented in Figure 3. Patients who had early exercises in a removable cast had better functional outcomes at 9 and 12 weeks postoperatively, p < 0.05 Mann Whitney test (Table 3). The difference between the two groups was less at 12 weeks.
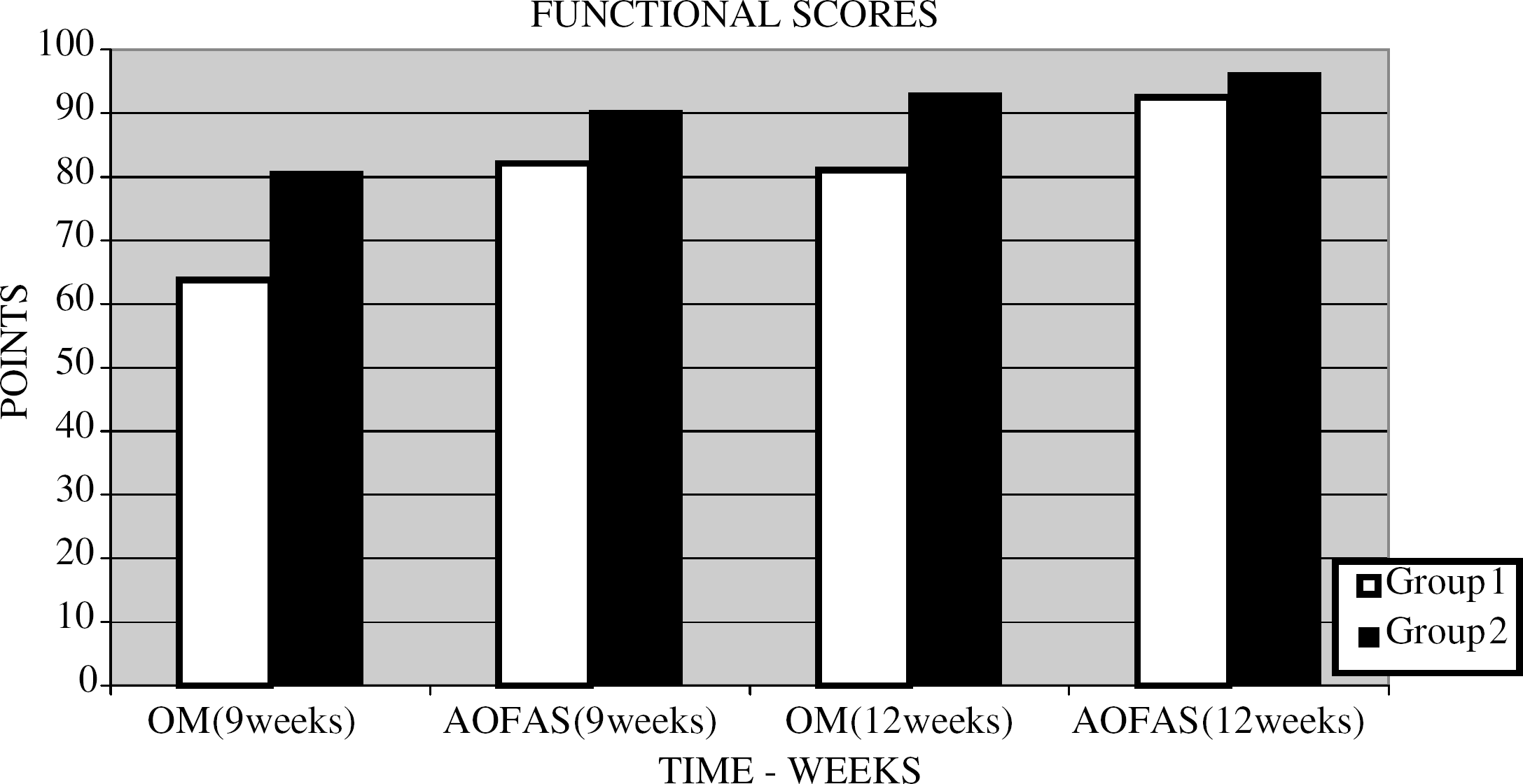
Functional scores in both groups G1, immobilization in cast, and G2, early mobilization in removable cast, at 9 and 12 weeks.
There was no statistical difference between the two groups in Quality of Life (SF-36) at 6 months. We had a 70% response rate to the SF-36 questionnaires sent by post to the patients.
Return to Work
When measuring time to return to work or to preinjury activity level (not applicable for students, housewives, or unemployed) we found that patients in G2 returned faster (mean 67 days, SD 18.7) than patients in G1 (mean 94.9 days, SD 24.4) (p < 0.05 Mann Whitney test).
Complications
In the group treated with nonremovable casts, two patients had deep vein thrombosis (DVT) of the popliteal vein in the postoperative recovery period. Both complications were clinically diagnosed and confirmed by Doppler ultrasound. They were treated with low molecular weight heparin subcutaneously followed by administration of warfarin for 3 months with an uneventful recovery. Doppler ultrasound was not routinely performed. DVT was found in the two patients in the immobilization group during clinical and functional assessment.
In the group treated with early exercise in a removable cast, three patients developed wound healing complications. One patient developed a superficial wound infection treated uneventfully with a 7-day course of oral antibiotics. Two patients developed deep soft-tissue infections. They subsequently had reintervention for removal of metal. One patient was a 16-year old boy who presented in the fifth week postoperatively with break down and subsequent infection of the wound. He was admitted to the hospital for intravenous antibiotics. His improvement was closely monitored as an outpatient. Clinically, he was improving, but he had a persistent discharging sinus. He returned to his preoperative level of activity after 11 weeks despite the discharging sinus. To eliminate further risk of developing osteomyelitis, at 5 months postoperatively the hardware was removed. There was no bone infection, and the fracture was fully healed. He made an excellent functional recovery. Of note, this patient had a pre-existing eczema around the ankle at the wound site, which could have been the cause of his deep soft-tissue infection.
The other patient, a 47-year-old woman developed at 8 weeks postoperatively a wound infection (Staphylococcus aureus). She improved on intravenous antibiotics, but the wound was still discharging serous fluid. Hardware was removed at 10 weeks postoperatively. There was no sign of deep bone infection intraoperatively. The soft-tissue infection persisted and subsequently resolved after 2 weeks of intravenous antibiotics. She was a poorly compliant patient with regards to the nonweightbearing status, and she was a smoker. She returned to work and to her preoperative level of activity after 4 months.
DISCUSSION
An early return to function is one of the principal aims of fracture treatment. Continuous pressure by the patients and society is exercised on medical personnel to deliver the best medical care in the shortest possible time. In light of this, assessment of short-term results that reflect the efficacy of fracture management are, therefore, important.
In the present study, we evaluated the short-term benefit of early mobilization on the functional outcome in patients who had ORIF of an ankle fracture. We assessed functional outcome through a number of variables: ankle swelling and range of motion, calf wasting, pain level, stiffness, functional ability, being able to return to previous activity level or occupation, and quality of life.
For the patients' safety, and to minimize the risk of loosening of the stable internal fixation, we recommended nonweightbearing to both groups for 6 weeks. There are studies in the literature that have shown the benefit of early mobilization combined with early weightbearing in the outcome of ankle fractures. 1,15 In our opinion, to reduce the risk of complications for such postoperative regimen, a more strict inclusion criteria and very reliable and compliant patients are needed. As patients included in both groups in our study were nonweightbearing for 6 weeks, we cannot comment on the influence of early weightbearing on the recovery after internal fixation of ankle fractures.
Based on the findings of Lehtonen et al., 14 who reported an unacceptably high risk of wound complications with immediate mobilization, and other authors' recommendations 1 we decided to mobilize the patients in a removable cast after primary wound healing. Immediate postoperative early mobilization in a premanufactured boot could be the cause of wound irritation and subsequent infection after surgery for ankle fractures. 14 To reduce the risk of wound irritation, a custom-made, light, removable fiberglass cast was used. The aim of this brace was to protect the ankle and the operative wound from further accidental injuries.
The results of our study indicate that early exercise after ORIF of ankle fractures does not reduce ankle swelling significantly at 6 and 9 weeks postoperatively. Patients who actively exercised their operated ankle early had significantly less calf muscle atrophy (approximately 2.5 cm) when compared to patients who were immobilized for 6 weeks. This would reflect a higher strength and a better function in the ankles at 6 weeks postoperatively. It has been estimated that during normal walking a capacity of dorsiflexion and plantarflexion of at least 10 and 15 degrees, respectively, is needed. 27,30 At 6 weeks postoperatively all ankles, except one in the early exercise group, reached a capacity exceeding these values. A single patient in the immobilization group was able to reach these range of motion values at 6 weeks postoperatively. The difference of range of motion of the ankles between the two groups was smaller at 9 weeks and it will probably reduce further in time, as patients in the immobilization group progress through their exercise program. This indicates a short-term improvement in range of motion of patients who actively exercised their ankle early postoperatively.
The benefits of a removable fiberglass cast also are subjective. The wearer is more comfortable and can remove the brace for personal hygiene and during the night. Doing daily exercises certainly has a motivational effect on these patients, and they are psychologically ready to return earlier to being active and to work. Our study showed that patients who exercised their ankle early postoperatively returned to work or to their initial level of activity approximately 3 weeks earlier. To our knowledge, at the time of the last followup visit, this finding was not influenced by workers' compensation incentive. A short-term benefit in functional outcome, assessed both subjectively (Olerud Molander and AOFOS scoring systems) and objectively (calf muscle wasting, range of motion, and time to return to work), has been seen in patients treated postoperatively with early exercise in a removable cast.
A relatively high incidence of DVT was seen in patients treated with total immobilization for 6 weeks postoperatively. This complication had no effect on the functional outcome of their ankle.
Despite the overall short-term benefit of early mobilization, we encountered three patients in the early exercise group who had wound complications. One had a superficial wound infection and two had deep soft-tissue infections. The two patients with deep soft-tissue infection did not see the benefit of early mobilization, because they required antibiotics, reintervention, and removal of hardware to prevent further bony infection. These were unexpected and potentially catastrophic complications that prolonged the postoperative recovery and delayed return to function.
It is very difficult from only two cases to draw conclusions with respect to the etiology of the deep soft-tissue infections. When looking individually at the two cases of deep wound infection, factors other than early mobilization could be contributing to the incidence of infection.
However, the rate of wound complications in our study group was significantly less when compared to the 66% rate of wound complications reported by Lethonen et al. 14 They exercised patients' ankles from the first day postoperatively in a premanufactured boot. Mobilizing our patients after primary wound healing and using a custom-made removable splint might have played a role in reducing the rate of infection in our study. Further prospective, randomized studies in bigger series with higher statistical power groups are needed to elucidate this.
The limitations of the study include the fact the investigators were not blinded to the treatment procedures when performing the followup examination. As we did not perform a power calculation to find the proper sample size before initiating the study, a flaw that is common to virtually all orthopaedic clinical trials, 29 caution is warranted in interpreting our data in this regard.
The results of the present study are in keeping with a recent systematic review of the literature related to the issue of immobilization compared to early mobilization after upper and lower-limb injuries. 21 The authors of the review concluded that early motion is consistently beneficial for all outcomes, including pain relief, range of motion, swelling, and return to work. 18 The results of our study indicate that early mobilization after primary wound healing in operatively fixed ankle fractures could be associated with potentially catastrophic complications, such as deep wound infection. Such postoperative regimens should be individualized, and both the surgeon and patient should be aware of a possible risk of wound complications associated with early mobilization after operative fixation of ankle fractures.