
Abstract
Background: The purpose of this study was to evaluate the effectiveness and safety of intra-articular sodium hyaluronate (Ostenil®mini) compared to intra-articular triamcinolone acetonide (Trigon depot®) in the treatment of painful hallux rigidus. Methods: Thirty-seven patients (ages 40 to 80 years) with painful early stage hallux rigidus were enrolled in the study. One group received an intra-articular injection with 1.0 ml sodium hyaluronate (SH); the other received an intra-articular injection of 1.0 ml triamcinolone acetonide (TA). Patients were evaluated on days 0, 14, 28, 56 and 84. Effectiveness was measured using the following parameters: joint pain at rest or on palpation (VAS), with passive motion, and gait pain; AOFAS hallux metatarsophalangeal score; use of analgesics and global assessment of the treatment by the patient and investigator. Safety was evaluated by the outcome of tolerance to treatment and observation of adverse events. Statistical analyses were performed using the Chi-square test, Mann-Whitney U test, Wilcoxon test and Friedman test. Results: Thirty-seven patients (40 feet) were evaluated. Pain at rest or with palpation and pain on passive mobilization decreased significantly in both treatment groups in comparison to baseline (p < 0.01), but no significant between-group differences were observed (p > 0.05). Gait pain improved substantially in the sodium hyaluronate group with significant differences compared to the triamcinolone group at days 28 and 56 (p < 0.05). The AOFAS total score improved significantly in the SH group compared to the TA group (p < 0.05). This was mainly due to improvements in the pain subscale. No between-group differences were seen regarding the use of analgesics. Global assessment of treatment by patients was good in both groups, and there was a significant between-group difference favoring SH when areas under the curves (AUC) were calculated (p < 0.05). Tolerance was good in both groups. Adverse events occurred in three patients. Conclusions: Intra-articular injections of sodium hyaluronate are effective and safe in decreasing hallux rigidus pain. The AOFAS scores in the SH group were significantly better than in the TA group.
INTRODUCTION
The term hallux rigidus is used to describe certain symptoms commonly associated with degenerative arthritis of the first metatarsophalangeal (MTP) joint. 1 Because of the restricted mobility and flexion deformity involving the MTP joint, the deformity also has been called hallux limitus and hallux flexus. Depending on the stage of the disease process, several operative techniques for the treatment of hallux rigidus have been reported. For early stages, cheilectomies, phalangeal or first metatarsal osteotomies, and interposition arthroplasties have been documented. 1 Late-stage disease requires more aggressive techniques, such as resection arthroplasty, implant arthroplasty, and arthrodesis. 1
Nonoperative treatment in the early stages includes the use of nonsteroidal anti-inflammatory agents, although little mention is made of its efficacy. 19 Although the effectiveness of corticosteroid and hyaluronic acid injections in osteoarthritic knees has been investigated, 11 to our knowledge, no such study has compared their effectiveness for hallux rigidus.
The aim of this study was to evaluate the effectiveness and safety of a single sodium hyaluronate (SH) injection in the first MTP joint of patients with symptomatic hallux rigidus in early stages. The results, after a 3-month followup, were compared with those obtained after a single triamcinolone acetonide (TA) injection.
MATERIAL AND METHODS
The protocol was approved by the Ethics Committee and the Research Committee for Clinical Trials of the hospital and satisfied ethical standards as described in the Declaration of Helsinki. 6 All participating patients were informed of the study objectives and their informed consent was obtained.
Thirty-seven patients (six men and 31 women) ages 40 to 80 years with painful osteoarthritis of the first MTP joint (hallux rigidus) with or without deviation (hallux valgus) and diagnosed by clinical examination and radiography (grade I according the classification of Karasick and Wapner 6 ) were enrolled in the study. Inclusion criteria also included pain on dorsiflexion or plantarflexion of the first MTP joint of more than 30 mm as measured on a 100-mm visual analogue scale (VAS). Patients with grade II or III osteoarthritic changes, 7 foot deformities, or pain that might interfere with the clinical assessment of the first MTP joint were excluded. Patients who had infections or previous surgery, had been treated with intra-articular injections, or were hypersensitive to SH or corticoids also were excluded.
A total of 37 patients were recruited and 40 joints were treated (20 per group). The demographic data were as follows: SH 80% women, TA 90% women; average age: SH 61.3 years ± 12.9, TA 62.7 ± 11.3; average weight: SH 66.5 kg ± 9.7 kg, TA 67.8 kg ± 9.1 kg). There were no statistically significant differences between the treatment groups regarding gender distribution (X 2 ; p = 0.6614), and the other demographic data (Mann-Whitney U test; p > 0.05). Three patients from the SH group and one patient from the TA group dropped out of the study for reasons not related to treatment; (3 feet SH; 1 Foot TH) therefore, 17 patients in the SH group and 19 patients in the TA group were evaluated.
Patients were randomly allocated into two groups and received a single intra-articular injection of either 1.0 ml SH (Ostenil®mini; TRB Chemedica AG, Haar/München, Germany) or 1.0 ml TA (Trigon depot®; Bristol-Myers-Squibb S.L.: New York, USA) into the MTP joint.
Each injection was given with use of the manufacturer's prefilled 1-ml syringe (Ostenil®) or 1 ml of TA. All injections were done in a similar manner with the patient supine. The foot was prepared in a sterile fashion, and a 25-gauge needle was placed into the joint lateral to the extensor hallucis longus. No topical anesthesia or image intensification were used. Patients were encouraged to refrain from strenuous activity for a day after the injections. As rescue medication, patients were permitted to take only paracetamol tablets (500 mg) for severe pain or symptomatic deterioration (not more than 2 grams per day).
Effectiveness was measured using the following parameters: target joint pain at rest or on palpation, measured with the 100-mm VAS; target joint pain during dorsiflexion and plantarflexion (VAS); pain on walking 20 meters wearing ordinary shoes (VAS); American Orthopaedic Foot and Ankle Society (AOFAS) score for hallux evaluation, with subscores for pain (40 points), function (45 points) and alignment (15 points); 8 use of pain rescue medication; and global assessment of the treatment by the patient and the investigator using a 5-point scale (0 = worse, 1 = no difference, 2 = slight improvement, 3 = good, 4 = optimal). The pain parameters and the AOFAS scores were evaluated at day 0 (before injection), and then at days 14, 28, 56, and 84 (end of study). Rescue medication consumption and global assessment of the treatment were evaluated at days 14, 28, 56, and 84.
To maintain the single-blind nature of the study, patients were unaware of which product they received.
Comparative intragroup and intergroup analyses were performed for all the assessment parameters. The percentage responders were calculated for pain at rest or on palpation, on passive mobilization, and gait pain. A responder was defined as a patient who had at least 20 mm decrease in the VAS measurement. Safety was assessed by the outcome of tolerance to treatment and by the analysis of adverse events reported by the patient or by the investigator. The ratio between two categorical variables was determined by the chi-square (X 2 ) test. Comparison of continuous (or categorical ordinal) variables between two groups was performed using the nonparametric Mann-Whitney U test. Comparison between two continuous (or categorical ordinal) related variables was performed using the Wilcoxon's ranksum test. Comparison between more than two continuous (or categorical ordinal) related variables was performed using the Friedman test. Two-tailed contrasts with α error rate = 5% were performed. Data processing was done using the statistical package SPSS version 11.5.1 (SPSS, Inc., Chicago, IL).
RESULTS
A significant decrease in joint pain VAS scores at rest or on palpation was observed in both treatment groups. Mean VAS scores decreased from 62.2 mm ± 10.7 at baseline to 26.2 mm ± 23.9 at day 84 in the SH group and from 58.7 mm ± 11.6 to 34.1 mm ± 16.6, respectively, in the TA group (Friedman test; p < 0.01). There were no statistically significant between-group differences at each followup visit (Mann-Whitney U test; p > 0.05) (Figure 1).
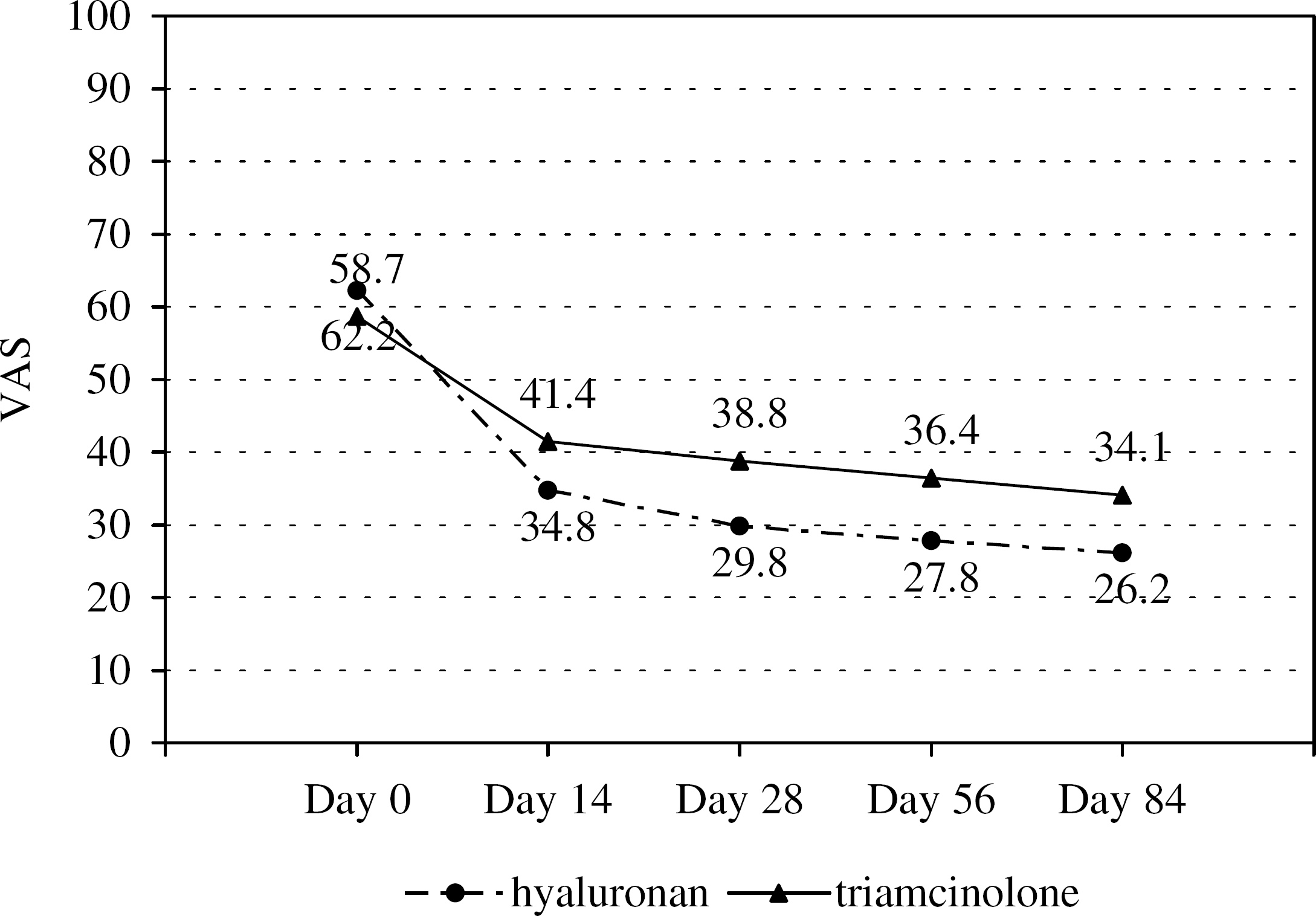
Pain of the first MTP joint at rest or on palpation. (0: no pain/100: pain ++++).
At day 14, nine (52.9%) of the patients in the SH group were considered as responders for pain at rest or on palpation, and this figure increased to 11 patients (64.7%) from day 28 to 84. In the TA group, there were six (31.6%) responders at day 14, seven (36.8%) at day 28, and nine (47.4%) at days 56 and 84. No statistically significant between-group differences were observed (X 2 ; p > 0.05) (Figure 2).
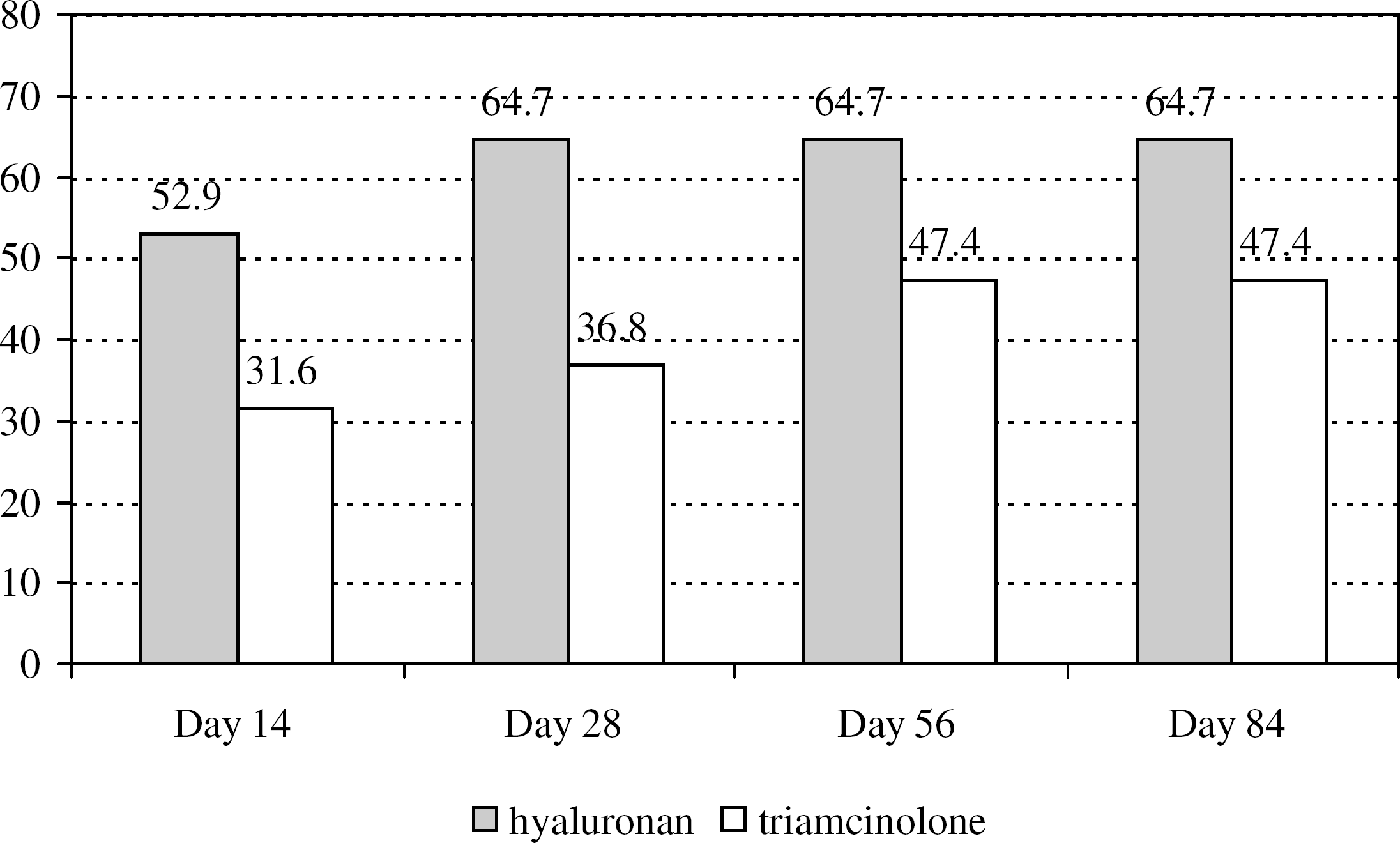
Responders in pain relief of the first metatarsophalangeal joint at rest or on palpation. (Values are expressed in % of patients) chi-square test; p > 0.05.
A significant decrease in dorsiflexion or plantarflexion VAS pain scores was observed in both treatment groups compared to baseline. Mean VAS scores decreased from 67.5 mm ± 10.7 at baseline to 39.4 mm ± 25.6 at day 84 in the SH group and from 64.2 mm ± 8.0 to 41.6 mm ± 16.5, respectively, in the TA group (Friedman test; p < 0.01). There were no statistically significant between-group differences at each followup visit (Mann-Whitney U test; p > 0.05).
The percentage of responders for pain on dorsiflexion or plantarflexion was globally greater in the SH group than in the TA group: eight (47.1%) of the SH patients were responders at day 14. This increased to nine (52.9%) at days 28, 56 and 84. In the TA group, seven (36.8%) of the patients were responders at day 14, nine (47.4%) at days 56 and 84, and 10 (52.6%) at day 84. No statistically significant between-group differences were observed (X 2 ; p > 0.05).
A significant decrease in joint VAS pain scores on walking 20 meters was observed in both treatment groups compared to baseline. Mean scores decreased from 61.4 mm ± 13.0 at baseline to 24.2 mm ± 24.1 at day 84 in the SH group and from 59.3 mm ± 12.2 to 36.8 mm ± 19.7, respectively, in the TA group (Friedman test; p < 0.01). There were statistically significant between-group differences in favor of SH at the followup visits on day 28 and day 56 (Mann-Whitney U test; p < 0.05) (Figure 3).
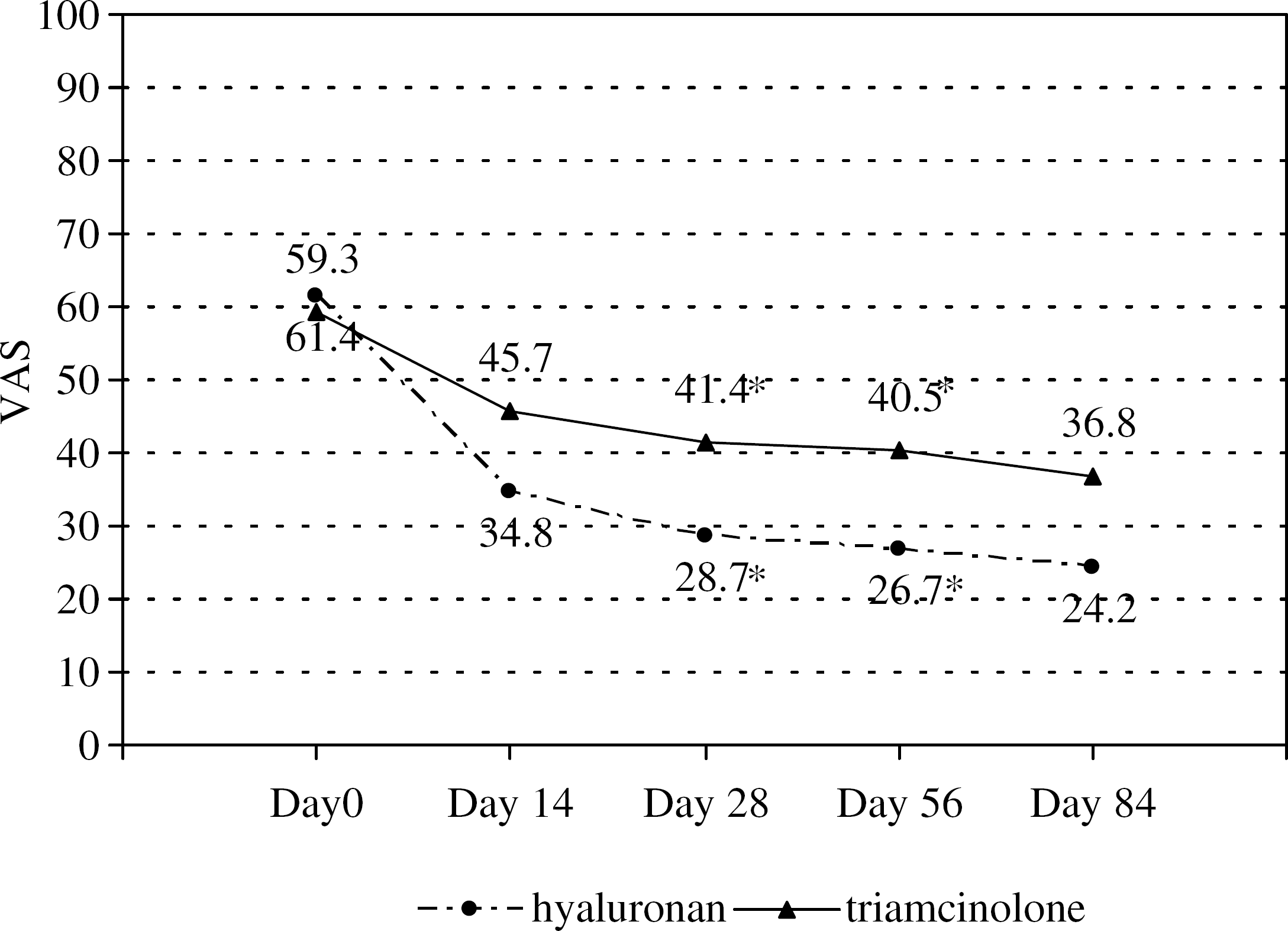
Pain on walking 20 meters wearing ordinary shoes. (0: no pain/100: pain ++++). *Statistically significant (Mann-Whitney U test; p < 0.05).
The responder rates for pain on walking 20 meters in the SH group were 58.8% (10 patients) at day 14 and 64.7% (11 patients) at days 28, 56 and 84. In the TA group, they were 31.6% (six patients) at day 14, 42.1% (eight patients) at day 28, 47.4% (nine patients) at day 56 and 52.6% (10 patients) at day 84. No statistically significant between-group differences were observed (X 2 ; p > 0.05) (Figure 4).
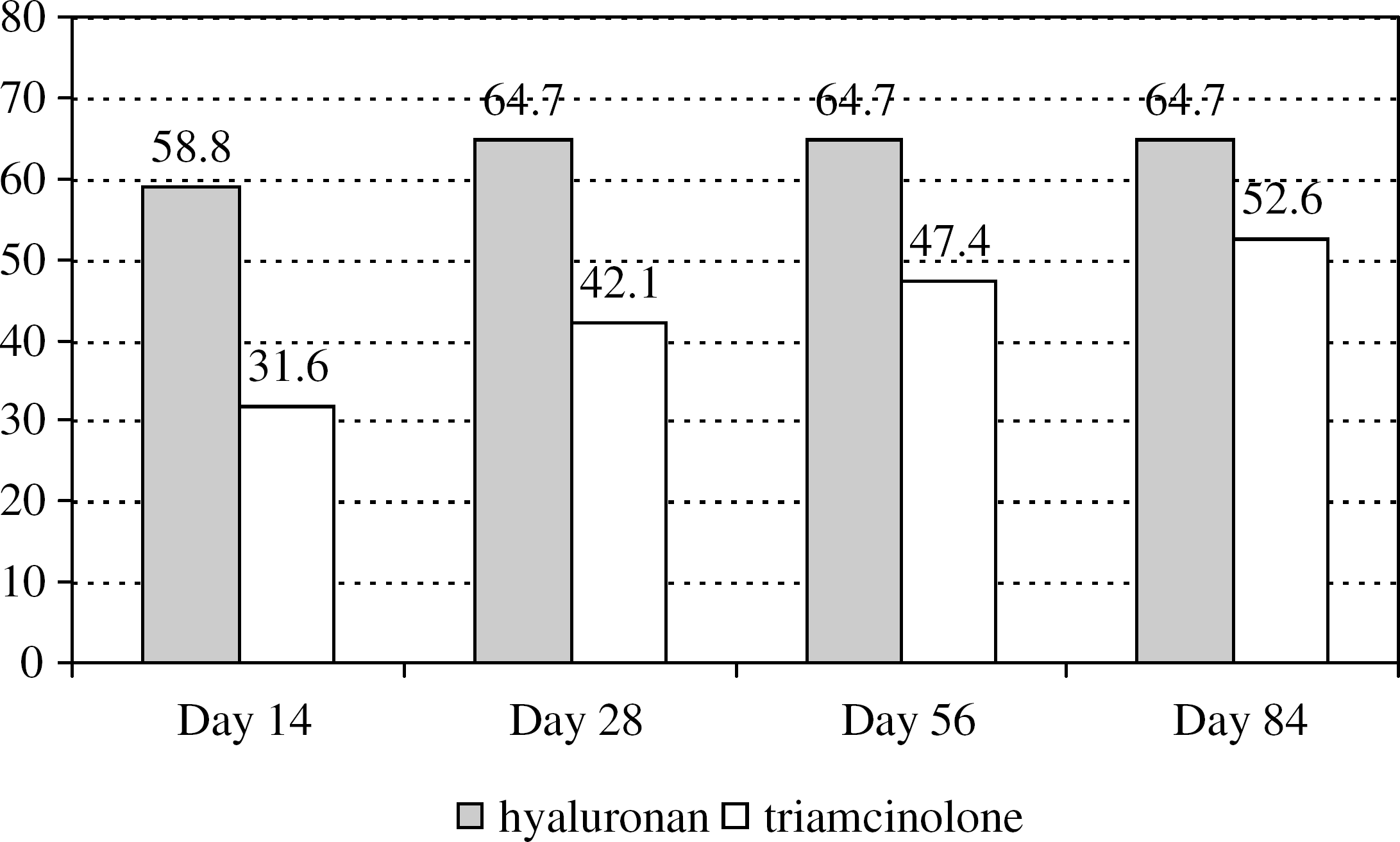
Responders in pain relief on walking 20 meters wearing ordinary shoes. (Values are expressed in % of patients) chi-square test; p > 0.05.
The analysis of the AOFAS hallux metatarsophalangeal score (0 to 100) showed a significant (p < 0.01) improvement in the mean total score in both treatment groups compared to baseline values. The mean total score increased from 51.0 ± 18.8 at baseline to 77.6 ± 15.8 at day 84 in the SH group and from 48.2 ± 16.9 to 64.3 ± 16.9, respectively, in the TA group (Friedman test; p < 0.01). While values for this parameter were similar at baseline, there were statistically significant (p < 0.05) between-group differences at all followup visits in favor of SH (Figure 5).
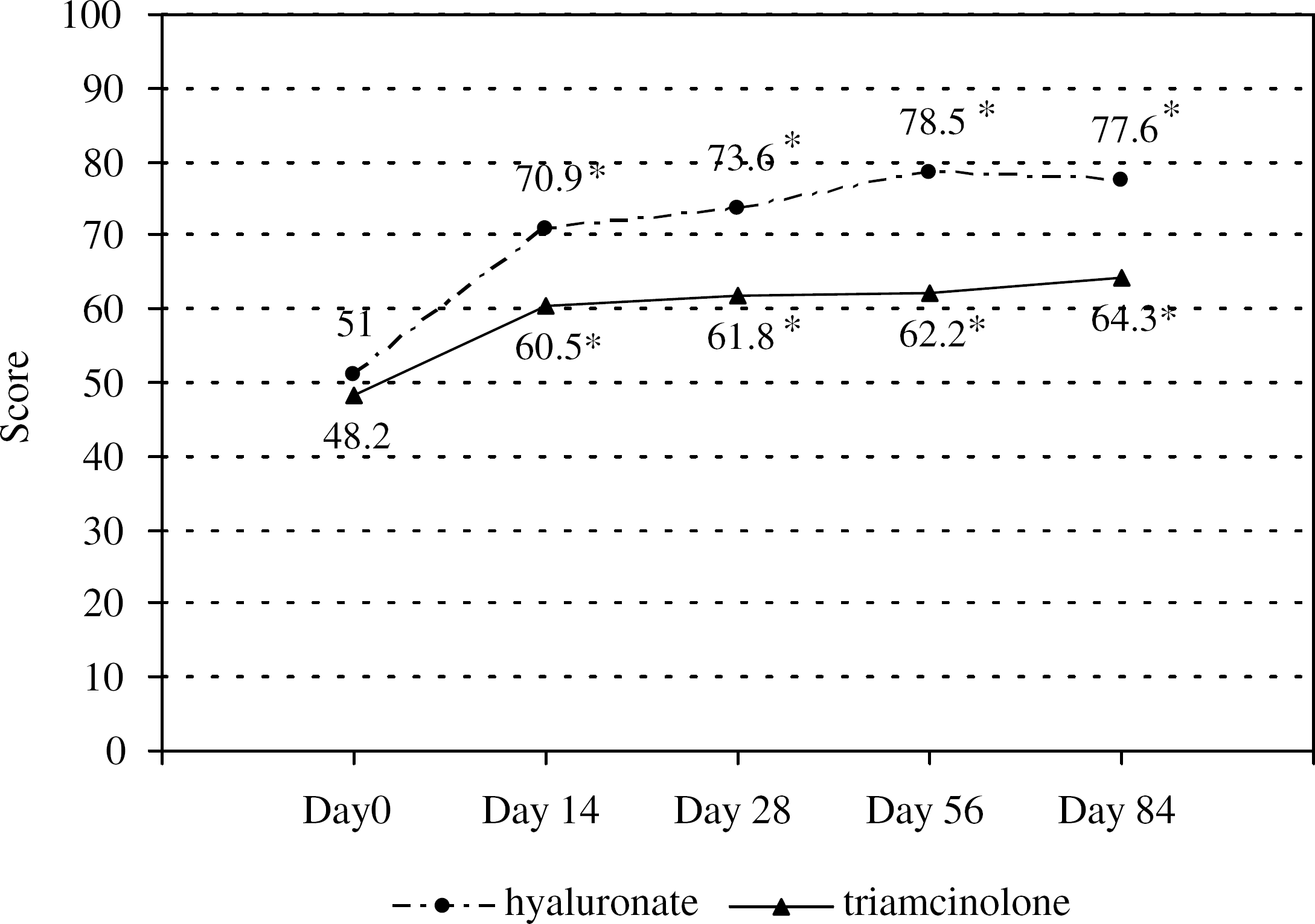
AOFAS-Hallux total score (0–100). *Statistically significant (Mann-Whitney U test; p < 0.05).
The detailed analysis of the variables according to AOFAS-hallux score showed a significant (p < 0.01) improvement in the pain subscore (0 to 40) in both treatment groups. The mean subscore increased from 14.7 ± 10.1 at baseline to 31.9 ± 7.5 at day 84 in the SH group and from 14.2 ± 10.2 to 25.8 ± 9.6, respectively, in the TA group (Friedman test; p < 0.01). There were statistically significant between-group differences in favor of SH at the followup visits on days 14, 28 and 56 (Mann-Whitney U test; p < 0.05) (Figure 6).

AOFAS-hallux pain subscore (0–40). *Statistically significant (Mann-Whitney U test; p < 0.05).
A significant improvement (p < 0.01) in the AOFAS-hallux function subscore (0–45) was observed in both treatment groups. The mean subscores increased from 27.4 ± 7.6 at baseline to 35.7 ± 6.5 at day 84 in the SH group and from 27.1 ± 7.5 to 31.2 ± 8.3, respectively, in the TA group (Friedman test; p < 0.01). No statistically significant between-group differences were found at the followup visits (Mann-Whitney U test; p > 0.05).
No significant changes in the mean alignment subscores (0 to 15) were observed in either group compared to baseline values. (Friedman; p > 0.05). In addition, there were no statistically significant between-group differences at the followup visits (Mann-Whitney U test; p > 0.05).
The consumption of rescue medication was negligible in both treatment groups, and no between-group differences were observed (Friedman; p > 0.05).
The mean score for global assessment of treatment by the patient at the end of the study (day 84) was 3.0 in the SH group and 2.2 in the TA group. The mean score for global assessment of treatment by the investigator at day 84 was 2.9 in the SH group and 2.3 in the TA group. For both parameters, the only significant difference (p < 0.05), compared with day 14, was seen at day 56 in the SH group. However, there was a significant between-group difference favoring SH when areas under the curves (AUC) were calculated (Mann-Whitney U test; p < 0.05).
Tolerance to treatment as rated by the patient and the investigator was reported to be good or excellent in both treatment groups with no between-group differences (Friedman; p > 0.05). The adverse events reported were restricted to pain or swelling at the injection site (two SH patients and one TA patient, X 2 ; p > 0.05).
At 1-year of followup, four patients were lost (two from each group) and seven of 15 in the SH group had required surgery (46.6%), while nine of 17 in TA group had required operative treatment (52.9%). There were no statistically significant between-group differences in 1-year operative procedure requirement (X 2 ; p > 0.05).
DISCUSSION
The intra-articular injection of corticosteroids is widely used in the palliative treatment of osteoarthritis. The longlasting effect of corticosteroids, such as triamcinolone acetonide, provides pain relief lasting weeks or months. This effect is believed to be due to the elimination of the inflammatory feedback loop, but there is no evidence that this pain relief modifies the progression of articular cartilage degeneration caused by osteoarthritis. 17
Hyaluronic acid or sodium hyaluronate therapy has been used for over 2 decades in the management of different medical problems, such as the treatment of degenerative arthropathies, wound healing, prevention of postoperative adhesions, ophthalmic surgery, plastic surgery, and other processes. 8,16 The results of various studies in animal models with osteoarthritis have suggested that hyaluronan therapy is capable of modifying the course of the disease and producing certain beneficial effects on the protection of articular cartilage. All these studies provide biochemical, morphological and histopathological evidence of such effects. 8,20
Most studies have involved the knee joint. Frizziero et al. 3 evaluated the morphological effects of sodium hyaluronate injections in osteoarthritic knees and observed an increase in chondrocyte density, a decrease in synovial inflammation, an increase in synovial repair, and a decrease in the extent and degree of cartilage lesions at 6 months. Using the same treatment, Pasquali Ronchetti et al. 15 reported a reduction in the hypertrophic lining cells of cartilage, an increase in fibroblast-like lining cells; reductions in macrophages, lymphocytes, mast cells, adipocytes, and edema, and increases in the number of fibroblasts and collagen. In a prospective study, Leopold et al. 11 compared the results of corticosteroids and hyaluronic acid in osteoarthritic knees and did not observe any significant differences between the groups for improvement of pain or function at 6 months.
Recent studies have shown the effectiveness of SH in other synovial joints, including the first metacarpophalangeal joint, 2,14 the shoulder (with osteoarthritis 4,18 and after arthroscopic subacromial decompression 5 ), the hip (with Osteoarthritis), 12,13 and the ankle. 8,10
To our knowledge, the present study is the only randomized, prospective trial that compares the effectiveness of intra-articular injections of sodium hyaluronate and a longlasting corticosteroid in patients with osteoarthritic degeneration or hallux rigidus of the first MTP joint. It also is the first study of this type to use the validated criteria of the AOFAS-hallux score. 9
A decrease in pain scores at rest or on palpation and in dorsiflexion and plantarflexion was seen in both groups, without significant between-group differences. The improvement in gait pain was significantly better in the SH group than in the TA group at days 28 and 56.
The AOFAS total score showed an improvement in both groups, with significantly better scores in the SH group at all visits after intra-articular injection; this was mainly due to improvements in the pain subscore.
Both patients and the investigator judged the treatment to be good, with a significant between-group difference in AUC favoring SH. No serious adverse events occurred and there were no between-group differences in the occurrence of adverse events.
In conclusion, an intra-articular injection of sodium hyaluronate or triamcinolone acetonide in patients with hallux rigidus resulted in a decrease in pain and an improvement in function at 3 months after the injection. However, the difference in pain relief was significantly better in the SH group at days 28 and 56. However, it should be noted that at 1-year followup a high percentage of patients in both groups had required surgery because of continued pain and reduced function (SH, 46.6%, TA 52.9%).