
Abstract
Background: The traditional operative management of Haglund deformity and retrocalcaneal bursitis consists of an open excision of the inflamed bursa, resection of the posterosuperior calcaneal tuberosity, and debridement of the Achilles tendinopathy. In an effort to reduce morbidity and recovery time, an endoscopic technique was used for the management of this condition. Methods: Thirty consecutive patients (32 heels) who had retrocalcaneal bursitis unrelieved by nonoperative measures were treated with the endoscopic technique. Two portals were created, one laterally and one medially, over the posterosuperior portion of the calcaneus to gain access to the retrocalcaneal space. The inflamed bursal tissue was removed, and the prominent bone was resected. Patients were evaluated preoperatively and postoperatively with the American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Scale. Results: The mean followup was 35 months. Twenty-eight patients (30 heels) were available for followup. The AOFAS scores averaged 62 preoperatively and 97 postoperatively. There were 26 excellent results, three good results and one poor result. One major and one minor complication occurred: an Achilles tendon rupture three weeks after surgery and residual pain and swelling that required reoperation through an open procedure. There were no wound complications or postoperative infections. Conclusions: The endoscopic technique can be done outpatient and has a low morbidity and high patient satisfaction. The time to return to normal activity level is short. Sufficient exposure of the Achilles tendon and removal of the calcaneal prominence and retrocalcaneal bursa can be done effectively using an endoscopic technique.
Introduction
Haglund deformity, described by Patrick Haglund 4 in 1928, is an enlarged posterosuperior border of the os calcis. The etiology of this condition was originally thought to be the result of wearing rigid low-back shoes. Today, Haglund syndrome is thought to be caused by inflammation within the retrocalcaneal bursa and Achilles tendon sheath and secondarily by insertional Achilles tendinopathy. The posterior heel pain and swelling associated with Haglund syndrome are the results of mechanical irritation by the calcaneal prominence on the surrounding soft tissues. 5,6,16
Clinical evaluation may help differentiate between retrocalcaneal bursitis and Achilles tendinopathy. However, the two often coexist. The retrocalcaneal space has been described as a disc-shaped bursa covering the posterosuperior angle of the calcaneus. 2 The bursal walls may become diseased and hypertrophied with repeated hindfoot movements. Pathology within this region is detected on clinical examination with point tenderness along the medial and lateral aspects of the Achilles tendon with an associated prominence of the calcaneus. Achilles tendinopathy is a degenerative process within the tendon substance causing microtears and reactive fibrotic scar formation that causes mechanical irritation on the surrounding followed by inflammatory reactive and attenuated repair. Palpation of the affected hindfoot often reveals tenderness at the distal portion of the Achilles tendon proximal to its insertion onto the calcaneus. The pain often can be reproduced with passive and active ankle dorsiflexion and plantarflexion. 10,12,15
Conservative measures for the treatment of posterior heel pain include the use of nonsteroidal anti-inflammatory medication, shoe modifications, such as avoiding heel counters (“backless” shoes), physical therapy for stretching exercises, and pressure relief inserts. Local injections can be given into the retrocalcaneal space, but the concomitant use of local anesthetics and corticosteroids may further weaken the substance of the Achilles tendon and risk rupture of the tendon. 7
Open operative correction is an alternative for those patients in whom conservative measures have failed to relieve symptoms. Open procedures include resection of the calcaneal prominence proximal to the Achilles tendon insertion with removal of the retrocalcaneal bursal. A dorsal closing wedge osteotomy can rotate the posterior calcaneus to less prominence. Complications associated with these procedures include hematoma, tendon or skin breakdown, nonunion, Achilles tendon avulsion, tenderness around the operative scar, cosmetic problems, altered sensation around the heel, and stiffness. 1,10,13,14,17
The endoscopic technique of decompressing the retrocalcaneal space was developed to reduce the morbidity and decrease the time to recovery for patients with retrocalcaneal bursitis. 18 The endoscopic technique has been shown to have fewer complications and to produce a better cosmetic appearance when compared with an open procedure. 11 This paper describes endoscopic bony and soft-tissue decompression of the retrocalcaneal space and presents the results from our patient series.
Materials and Methods
Patients
Thirty consecutive patients (32 heels, two bilateral) had endoscopic decompression There were 14 men and 16 women. The average age was 51 (range 22 to 75) years. Seventeen procedures were done on the left and fifteen procedures were done on the right. Each patient gave informed consent prior to treatment. The time to surgery after diagnosis of retrocalcaneal bursitis averaged 20 months. Nonoperative measures, including the use of nonsteroidal anti-inflammatory medications, physical therapy, shoe modifications, the wearing of “backless” shoes, and local injections, failed to relieve symptoms in all patients. There were four patients who received a local injection by other providers and three of the four received steroid injections. All patients had been referred to the author (AMM) from other medical providers. None of the patients had had previous surgery to the affected hindfoot. Radiographs and optional MRI of the hindfoot were reviewed in all patients. Indications for operative intervention included failed nonoperative measures, history and physical examination findings consistent with retrocalcaneal bursitis, a Haglund deformity causing mechanical impingement, or Achilles tendinopathy, or a combination of the three. There was a high association of coexisting Achilles tendinopathy in patients over the age of 50 years. The procedure was not recommended for patients with marked Achilles tendinopathy or marked calcific insertional Achilles tendinosis. A lateral plain radiograph was used to determine the amount of calcific tendinosis. The endoscopic procedure was not recommended when there was spurring of more than 50% of the insertion. These patients had open debridement with tendon augmentation, depending on the degree of tendinopathy, age, and activity of the patient. MRI was helpful in examining the amount of Achilles tendinosis in the older subset of patients, but there was not a defined amount of tendinosis to strictly exclude a patient from a closed endoscopic procedure. Patients were prospectively followed from 1997 to 2003.
Scoring
Twenty-eight patients (30 heels) were located for followup. Patients were followed at two separate medical universities. The patients completed subjective and objective measurements for each heel using the American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Scale. 8 In 12 patients, preoperative AOFAS subjective scores were not documented, but they were collected retrospectively. The objective portions of the questionnaires were completed during the postoperative examinations. All patients were examined by the senior author (AMM) before and after the surgery. The postoperative subjective scoring was collected through telephone interviews by the first and second authors. Additional questions asked during the telephone interviews included: presence of contralateral symptoms, footwear limitations, and satisfaction with cosmetic appearance. Finally, patients specified the number of postoperative months before return to (a) normal daily function and (b) recreational and competitive activity as before symptoms. The scoring of the results was done by an uninvolved surgeon.
Statistical Methods
A Wilcoxon two-sample test was used to compare the preoperative and postoperative scores for all 28 patients.
Operative Technique
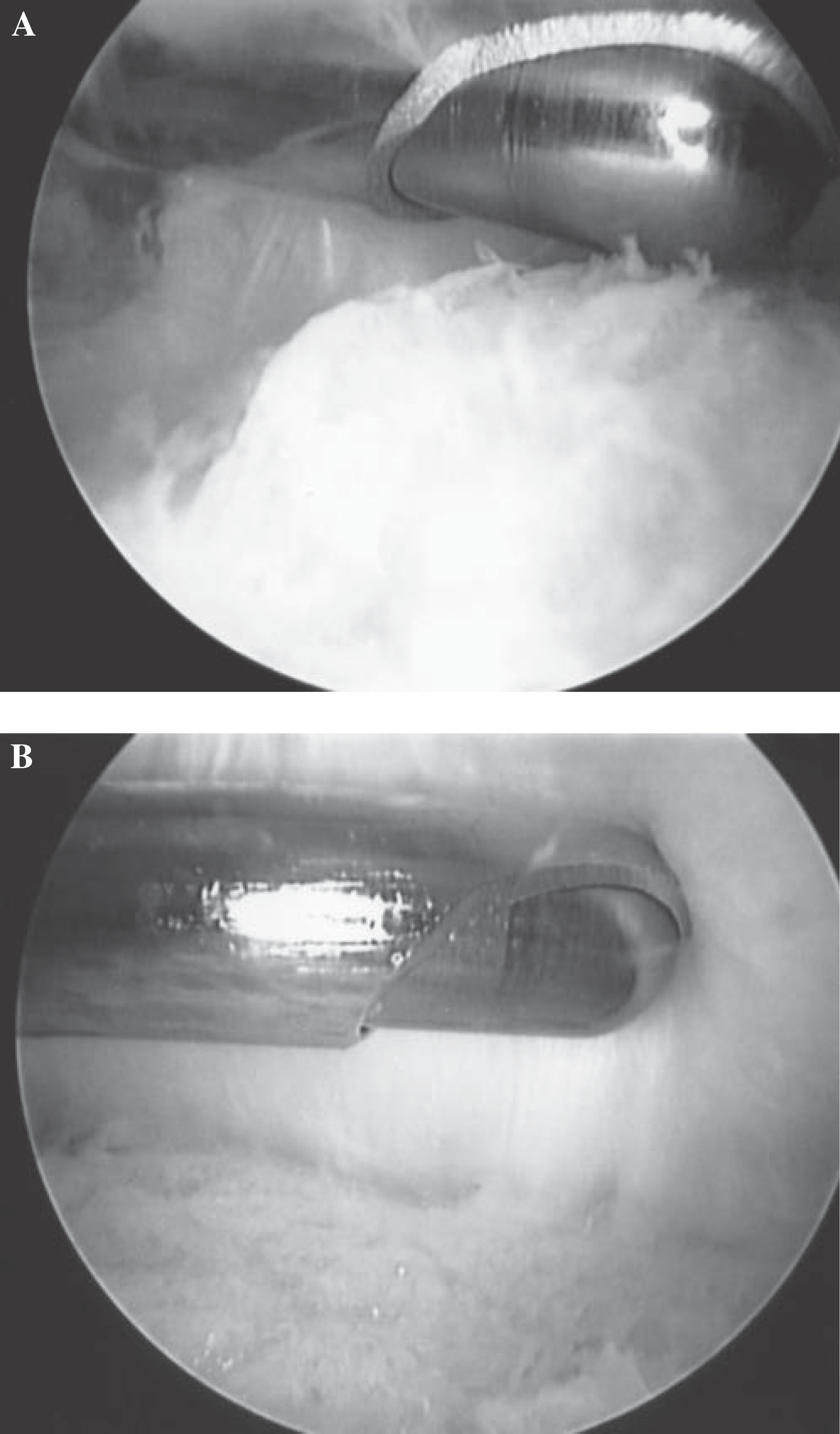
The operation was performed with the patient supine and under either general or regional anesthesia. A high-thigh tourniquet was inflated to 300 mm Hg after Esmarch ischemia. The foot was positioned at the edge of the operating table. This enabled the surgeon to place the foot against his or her body while using both hands to operate the arthroscopic instruments. The leg rested on a firm, but padded 12-in long and 4-in diameter cylindrical bump that allowed the surgeon ample room to work and control ankle dorsiflexion and plantarflexion. The prone position also can be used. Both positions allow the patient's foot to be controlled against the chest of the surgeon and leave both hands free for the instruments. A lateral portal was made through a vertical incision at the level of the superior aspect of the calcaneus. This incision was slightly anterior to the Achilles tendon and posterior to the sural nerve. It is important to bluntly dissect and spread the soft tissues when making the lateral portal to minimize the risk of injury to the sural nerve. The retrocalcaneal space was entered with a blunt trocar. A 4.0 mm arthroscope was then placed into the retrocalcaneal space (in small patients a 2.7-mm arthroscope was used). The medial portal was similarly established just anterior to the Achilles tendon using the light of the arthroscope as a guide. A 4.0-mm arthroscopic shaver was introduced into the medial portal, and the bursal tissue was removed. Once working space had been created there was access to the posterior calcaneus and Achilles tendon attachment (Figure 1). Depending on the quality of the bone, either the arthroscopic shaver or a 4.0 mm arthroscopic burr or both were used to resect the posterosuperior calcaneal prominence. The hooded portions of the instruments were kept toward the tendon to protect the tendon. Bone resection was done systematically usually from a posterior to anterior direction (Figure 2). The resection was carried out both medially and laterally into the sulcus of the calcaneus and down to the attachment of the Achilles tendon. Adequate exposure and resection of the osseous prominence were generally possible with visible and tactile guidance. In a small percentage of cases, a mini C-arm (Mini 6600 series; GE OEC Medical Systems, Salt Lake City, Utah) was used to determine and document the extent of the resection fluoroscopically. Damaged or diseased Achilles tendon was selectively exposed, identified, and removed with the arthroscopic shaver. In some cases an 18-gauge needle was inserted several times into the tendon. The rationale for this technique was to initiate a vascular response within the tendon for healing and was performed after debridement. An arthroscopic probe was inserted into the retrocalcaneal space to confirm attachment of the Achilles tendon. The foot was then hyperplantarflexed and dorsiflexed to verify any last areas of impingement. The retrocalcaneal space was irrigated and suctioned to remove any loose tissue. The portal sites were closed with two or three 4-0 nylon skin mattress sutures. A local anesthetic (0.25% Marcaine without epinephrine) was then injected into the portal sites. A compressive dressing was applied, and the foot was splinted in slight equinus.
Postoperatively, the patient was instructed to remain nonweightbearing in the splint for 10 to 14 days. The splint was then removed and exchanged for a walking boot for 2 to 3 weeks. Normal walking was resumed at 4 weeks, and the patient was able to resume wearing normal shoes as tolerated. Athletic activity was generally resumed 6 to 12 weeks postoperatively.
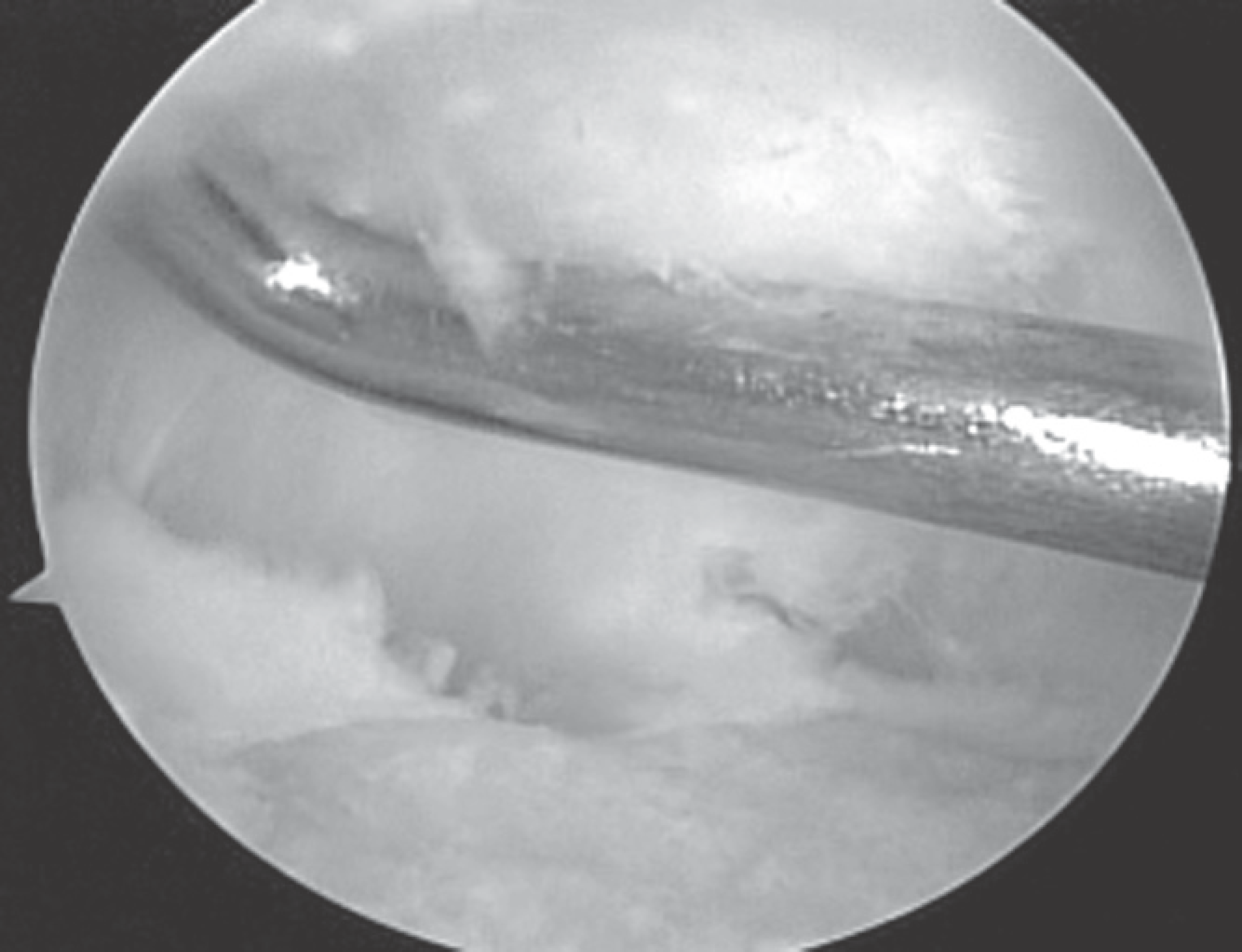
An arthroscopic probe demonstrates the working space created to see the posterior calcaneus and Achilles tendon attachment.
Results
Completed questionnaires were collected from 28 patients (30 heels). Two patients were lost to followup. The mean followup was 35 (range 3 to 62) months. Twenty-eight patients had a preoperative average AOFAS score of 62 points (range 36 to 77, standard deviation, 12.7; standard error of the mean 2.3). Postoperatively the AOFAS averaged 97 points (range 78 to 100, standard deviation, 6.1; standard error of mean, 1.1). The distribution of preoperative and postoperative pain scores is shown in Figure 3. Twenty-six feet had excellent results and three had good results. There was one poor outcome and one major complication. An excellent result was defined as pain-free activity with complete return to activity, and a poor result was defined as having persistent symptoms and the inability to return to activity.
The patient with the poor outcome had residual pain and swelling postoperatively and required an open procedure with resection of a portion of the calcaneus and Achilles tendon augmentation with the flexor hallucis longus. This patient's contralateral foot had previously had several open procedures for nonunion of a calcaneal osteotomy and had Achilles tendinopathy requiring extensive debridement and tendon augmentation. The patient returned to work as a radiology technician without an orthosis or shoe limitations.
One major complication occurred in 30 heels. The patient sustained an acute Achilles tendon rupture (of an unprotected tendon) 19 days after endoscopic decompression. This patient had primary repair of the tendon and returned to her preoperative activity level. The patient had a good result from the procedure with minimal residual weakness. She is able to perform a unilateral toe raise, has a normal gait, and is able to wear shoes with a heel counter.
There were no intraoperative complications. There were no skin or soft-tissue complications, wound dehiscence, or postoperative infection. There were no painful scars or neuroma type symptoms. All patients reported satisfaction with the cosmetic appearance of the portal sites. The number of patients who had debridement of the tendon was not adequately documented, and the depth of the debridement was difficult to judge endoscopically.
The average time to full weightbearing was 4 weeks. The average number of weeks at which patients reported wearing shoes with a heel counter and return to normal daily function was 8 weeks. The cohort was stratified into athletic (daily athletic activity) and nonathletic groups, and the groups were compared. No statistical differences in outcome between the two groups existed. All athletes returned to their previous levels of activity in an average of 12 weeks. These results compare similarly with those of published by van Dijk. 19 In their group of 20 patients, sports resumption took place at an average of 12 weeks. 19
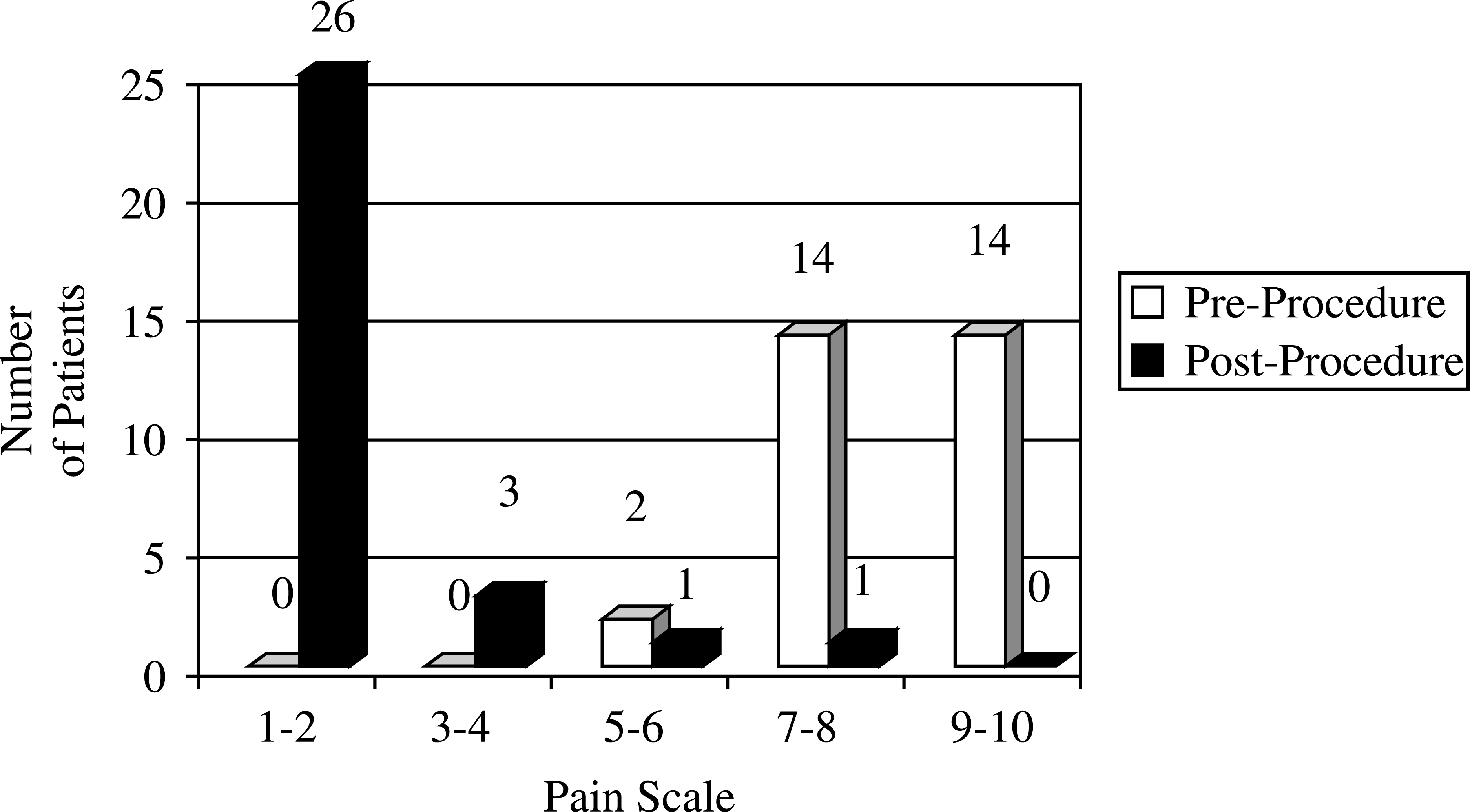
Distribution of preoperative and postoperative subjective pain scores.
Discussion
The goal of treatment of Haglund deformity is to remove the calcaneal prominence and to decompress the inflamed surrounding soft tissues. It can be difficult to determine whether the etiology of a patient's symptoms, is retrocalcaneal bursitis or insertional Achilles tendinosis/tendinitis. Watson et al., 20 in a study of 38 patients, compared outcomes in patients with a diagnosis of retrocalcaneal bursitis to patients with a diagnosis of calcific Achilles tendinosis and found lower satisfaction rates and greater time to reach maximal improvement in the Achilles tendinosis group. 20
In the current study, the clear distinction between the two diagnoses was not defined and the two often coexisted. MRI was used preoperatively in several patients to better demonstrate the coexistence of the two diagnoses. MRI was obtained in these patients because they had not shown any response to a 6-month nonoperative program, including physical therapy and anti-inflammatory medication. Normal appearing and diseased tendon could be distinguished endoscopically. Tears within the tendon were debrided or a technique was used to initiate a healing response. The two diagnoses were not distinguished; however, most patients in this series reported good or excellent outcomes.
The success rates for patients undergoing an open calcaneal resection have been reported to be between 50% to 100%. Angermann, 1 in a series of 40 heels that had open resection of the calcaneus, reported that 70% of the patients believed they were cured or improved. Within that series, 20% were unchanged and 10% were worse. There were several minor complications including superficial infection, hematoma, and delayed healing of the skin. Pauker et al. 14 published a series of 19 patients over 20 years who had open resection of the calcaneal prominence and did not have the retrocalcaneal bursa removed. Fifteen of the 19 patients had good results. The two fair and two poor outcomes resulted from insufficient bone removal. Better results occurred in those patients who had enough resection to prevent impingement when the foot was maximally dorsiflexed.
Methods to determine how much bone should be removed have been described. Leitze et al. 11 used preoperative radiographic measurements and intraoperative fluoroscopy to determine the angle of resection of the posterior prominence of the calcaneus. These measurements were done for patients who had an open or endoscopic procedure. The postoperative angle of resection averaged 51 degrees for both groups. There was no association with improved outcome and angle of resection. Within our series of patients, resection was carried out until there were no areas of impingement of the Achilles tendon as seen with the endoscope. Preoperative and postoperative radiographs were completed on all patients. There was no attempt made to correlate the amount of radiographic bone resection and patient outcome.
One complication of posterior prominence resection of the calcaneus is Achilles tendon rupture. Based on anatomical dissections and biomechanical testing, it has been shown that when performing partial resections of the Achilles tendon as much as 50% of the tendon may be resected safely superiorly to inferiorly. 9 To date there have not been any reported ruptures of the Achilles tendon with the endoscopic technique. The one Achilles tendon rupture in this series occurred after endoscopic resection while the patient was ambulating without a prescribed protective walker boot. The patient had evidence of Achilles tendinopathy endoscopically. One might argue that when the tendon is debrided endoscopically that it is difficult to judge the depth of the debridement, thus favoring an open debridement. This patient may have benefited from a longer period of immobilization to allow further protected healing and better compliance. Patients need a longer period of cast immobilization after debridement of the Achilles tendon or Achilles tendinopathy.
Endoscopic decompression has been shown to be an effective method of treating Haglund deformity and retrocalcaneal bursitis. Van Dijk et al. 19 had 19 good to excellent results in their series of 20 patients. There were no operative complications or postoperative infections. More recently, Leitze et al. 11 compared endoscopic decompression with the standard open technique. Patient outcomes and recovery times were similar, but there were fewer complications and a better cosmetic appearance with the endoscopic technique. 11 In this current study of 30 heels, there were 28 good to excellent results. There were no postoperative infections or skin complications.
These results must be qualified by the limitations associated with this study. This was a prospective evaluation of a small cohort. Not all AOFAS scores were collected prospectively. Retrospectively acquired scores are subjected to bias. There also are limitations in the AOFAS scoring system, and the AOFAS scores must be interpreted carefully. 3 The results demonstrate the capacity for the technique to relieve pain but not to accurately distinguish between tendinopathy and retrocalcaneal bursitis. There were variations in the techniques used to treat associated tendinopathy found during the endoscopic procedure. It was not possible to determine the exact number of patients who had significant tendon debridement during the endoscopic procedure.
In summary, Haglund deformity and retrocalcaneal bursitis can be treated operatively after conservative measures have failed to relieve symptoms. An open or an endoscopic technique can be used. The endoscopic technique can be done outpatient and has low morbidity, high patient satisfaction, and a short recovery time.