
Abstract
Background: The aim of this study was to evaluate the results of a series of subtalar arthrodeses done by a single surgeon using a standard technique. Methods: A retrospective review of 95 primary isolated subtalar arthrodeses in 92 patients was done. Original diagnoses included post-traumatic subtalar arthrosis, primary osteoarthrosis, talocalcaneal coalition, and inflammatory joint disease. In all arthrodeses, a single 7.0-mm partially-threaded cancellous screw was used for fixation, and autogenous bone graft was used. Structural iliac crest autograft was required to restore heel height in three feet with post-traumatic arthrosis. In these three, autograft was harvested from the iliac crest with the remainder receiving morcellized autograft either from the tibia, fibula, or calcaneus. Results: No patients were lost to followup. Ninety-five percent (87) of patients went on to bony union radiographically. Using the Angus and Cowell rating system, 93% (88 feet) of patients had a good or fair outcome. There were seven poor results: four arthrodeses failed to unite, two patients had persistent hindfoot pain in spite of radiographic union, and one developed post-traumatic ankle arthrosis. Conclusions: The results of isolated subtalar arthrodesis using a single screw for fixation are comparable to other fixation methods. Bone graft from local sites obviates the need for iliac crest autograft in most patients.
Keywords
Introduction
Subtalar arthrodesis is the fusion of the talocalcaneal joint. Like triple arthrodesis, subtalar arthrodesis is indicated for treatment of multiple adult hindfoot pathologies. It is a less technically demanding procedure than triple arthrodesis 11 with the added advantage of preserving some hindfoot function. 2
Published series of subtalar arthrodesis are invariably retrospective reviews of small, heterogenous groups of hindfoot pathologies. In addition, successful fusion is consistently determined by clinical examination in conjunction with plain radiographs. As a result and with the failure to followup on every patient, the true rate of fusion remains undefined.
The aim of our study was to determine the rate of fusion and assess the outcome of an accepted method for subtalar arthrodesis done by a single surgeon (TSS).
Materials and Methods
Between January, 1993, and August, 2003, the senior author (TSS) performed 95 primary subtalar arthrodeses in 92 patients. A retrospective chart review was completed for all patients. There were 68 men and 24 women with a mean age of 46 (range 21 to 79) years at the time of surgery. Three patients had staged bilateral procedures: two men had post-traumatic osteoarthrosis following bilateral intra-articular calcaneal fractures, and one woman had rheumatoid arthritis. The primary diagnoses were post-traumatic osteoarthrosis (64 feet), primary osteoarthrosis (no other specific diagnosis was made) (22 feet), tarsal coalition (five feet), and inflammatory joint disease (four feet). The same operative technique was used with either autologous local bone graft (92 feet) or structural graft (three feet).
All 92 patients were evaluated clinically and radiographically until union was achieved or the diagnosis of nonunion was established by CT. The radiographs obtained included anteroposterior and lateral views of the ankle and subtalar views. All radiographs were independently evaluated by a radiologist. All cases of suspected nonunion (nine patients), 10 feet had CT. The criteria for union was more than 50% posterior facet consolidation on CT.
Operative Technique
Under thigh tourniquet control, a 4-cm horizontal incision was made from the tip of the fibula aligned with the fourth metatarsal. With careful protection of the superficial peroneal nerve and the peroneal tendons, the extensor digitorum brevis was elevated to expose the posterior facet.
The sinus tarsi was cleared of soft tissue, allowing lamina spreaders to distract the posterior facet. The articular surface was then denuded of cartilage using a flexible chisel until the tendon of the flexor hallucis longus could be seen across the joint. Joint apposition was then assessed and bone graft used to help achieve apposition or correct hindfoot alignment. Structural graft was harvested from the ipsilateral iliac crest in three patients in which heel height required restoration. Alternatively, the lateral calcaneal wall provided a source of graft after calcaneus fracture (67 feet), otherwise graft (25 feet) was harvested from the tibia or fibula. Once bony apposition was achieved, a guide wire was advanced from the calcaneal tuberosity, across the posterior facet into the talar dome and the position checked fluoroscopically. After appropriate reaming, a single 7-mm partially threaded cancellous screw was advanced along the guide wire to provide compression; the head of the screw was not countersunk. The wounds were closed in anatomical layers and the plantigrade limb placed in a plaster-of-Paris splint.
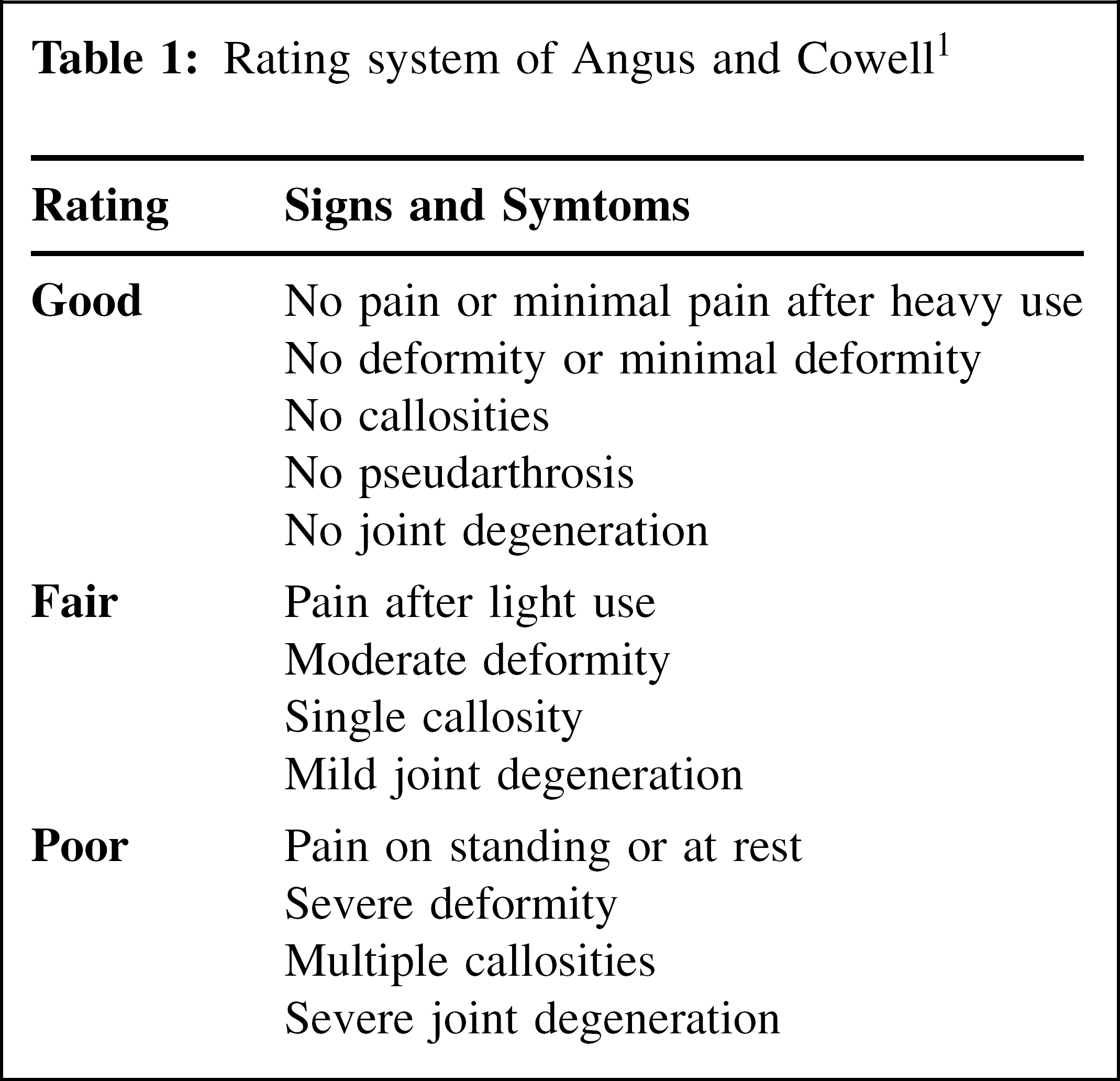
After wound inspection 10 to 14 days postoperatively, a complete cast was applied with the patient remaining nonweightbearing. Weightbearing commenced at 6 weeks within a cast. Twelve weeks postoperatively, the cast was removed to permit clinical and radiographic assessment. This was repeated at 6-week intervals until union occurred (Figures 1 and 2). Patients with persistent pain and poor radiographic evidence of progression to union had CT scans to assess union. Outcomes were graded according to the Angus and Cowell 1 scoring system (Table 1).
Results
Of the 95 arthrodeses, there were 67 “good” results as determined by the Angus and Cowell 1 criteria. There were 21 “fair” and seven “poor” results. The mean time to union was (range 3 to 12) months. Six arthrodeses failed to achieve union (6.3%), which was diagnosed at average of 7 (range 6 to 8) months with the aid of a CT scan. In each of these cases, the primary diagnosis had been osteoarthrosis secondary to calcaneal fracture. Two of the nonunions occurred in one patient (a heavy smoker) with previous bilateral calcaneal fractures. Despite this, the patient had a “fair” outcome and elected for further nonoperative management. The remaining four nonunions accounted for four of the seven “poor” results. All proceeded to successful union after revision surgery. Chronic regional pain syndrome (one foot) and persistent hindfoot pain of indeterminate cause despite CT confirmation of union (two feet) accounted for the other three “poor” results.

Lateral radiograph demonstrating a single lag screw across the fusion mass.

Anteroposterior radiograph showing the lag screw in situ.
Rating system of Angus and Cowell 1
Six patients developed a superficial wound infection that required oral antibiotics and two patients had a deep venous thrombosis. Eight patients required removal of a prominent screw at an average of 8.5 months after the index surgery (range 3 to 12 months).
Discussion
Isolated subtalar arthrodesis is an accepted treatment for many adult hindfoot pathologies. Most surgeons perform an open procedure, but arthroscopic approaches also have been described. 13 In addition, many methods of stabilizing the arthodesis have been used including staples, 3 dowels, 4 and variable numbers of lag screws introduced either through the talus or the calcaneus. 6,7,10,15 Regardless of the fixation technique, the results have been uniformly successful, with rates of union ranging from 86% to 100% for primary procedures. 3,4,5,6,7,9,10,11,12,13,15 In this study, all 95 arthrodeses were done using the same established operative technique 7,9,11,12 by the senior author (TSS). No revision procedures were included in the chart review for this study, eliminating the potential detrimental effects of revision data on the outcome of primary procedures.
Regardless of the operative techniques or method of fixation used, high rates of bony union have been reported. Studies with large patient numbers suggest lower union rates of 86% to 98%. 5,7,12 In several studies, each with fewer than 45 patients, 100% rates of union have been reported; 3,9,10,11,12 however, three of these studies 3,10,12 had significant loss of patients to followup, giving a potentially misleading rate of union. 3,10,12 Moreover, the high rates of bony union may bring into doubt the clinical and radiographic methods of assessing union or may reflect the small numbers within a series. As our experiences in this study showed, one patient with bilateral post-traumatic degeneration of the posterior facet had sequential bilateral subtalar arthrodeses. After the first procedure, the patient was free of pain with plain radiographic appearances to suggest bony union. On this basis, it was deemed appropriate to proceed with the contralateral arthrodesis. After this procedure, it became apparent that neither attempt to arthrodese the subtalar joints had been successful, because the patient had continued bilateral hindfoot pain. CT scans demonstrated nonunion of the posterior facet. As a consequence, the senior author (TSS) assumed nonunion regardless of the normal radiographic appearance. This is supported by a recent study by Jones et al. 8 who developed a quantitative method for measuring the fusion mass in hindfoot arthrodeses with a postoperative CT scan. They found that plain radiographs may be misleading and believed that CT provided a much more accurate assessment of union. In the two patients with persistent pain and poor clinical outcomes, the CT results excluded nonunion as the cause of pain. In all assumed cases of nonunion, a CT scan should be obtained to clearly image the site of the arthrodesis without metalwork artifact. It would be ideal to obtain a CT scan to confirm union in all patients; however, this would expose a large number of patients to unnecessary expense and radiation. We believe that it is more practical to recommend CT only in patients with significant persistent pain.
An explanation for the variation of union rates among studies 3,7,9,10,11,12 is the retrospective nature; results from each of these studies could be skewed because of loss of patients to followup. Although this study also is retrospective in nature, all patients were followed until union was certain. As a consequence, the union rate of 95% of patients in this study is likely to be a more accurate figure for primary subtalar arthrodesis.
The results of this study demonstrate an accurate and favorable rate of fusion for subtalar arthrodesis using a standard technique. We recommend the use of CT to accurately determine fusion in patients with persistent hindfoot pain.