
Abstract
Background: A retrospective case review of 65 agility total ankle replacements (64 patients) was done between April, 1998, and March, 2002. The purpose of this study was to more closely identify factors that may be predictive of a favorable outcome, including a comparison of outcome measures between patients who had preoperative corrective procedures and those patients who did not. Methods: The outcomes of this series of patients were examined with post-operative Short Form (SF)-36 scores as well as chart and radiographic review. Endpoints for this study were amputation, arthrodesis, osteochondral allograft, total ankle revision, or revision of either or both components. The Kaplan-Meier survivorship curve also was estimated including the 95% confidence intervals. Results: Patients with rheumatoid arthritis (RA) were found to have a statistically significant lower rate of failure. Use of a size 1 prosthesis was associated with subsidence and the highest rate of subsequent failure, but fell short of statistical significance (because of the limited power of the study). Smoking, diabetes, and methotrexate use were not associated with an adverse outcome either clinically or statistically, but the number of patients in each group was small. The age of the patient was not a factor in predicting failure of the prosthesis in the posttraumatic arthritis group; however it trended toward significance in the osteoarthritis group. The mean time to failure in patients with osteoarthritis was shorter than in the patients with post-traumatic arthritis but fell just short of statistical significance. Conclusions: From this series we concluded that rheumatoid arthritis and use of a prosthesis larger than size 1 are predictive factors for better outcome.
Introduction
Although ankle arthrodesis may provide good early relief of pain, it may be associated with premature deterioration of other joints of the foot and eventual arthritis, pain, and dysfunction. 2,4 Total ankle replacements are available for treatment of end-stage degenerative joint disease as an alternative to fusion. 5,13 The Agility (DePuy, Warsaw, IN) total ankle has been available for general use since 1998 and has been featured in outcome studies. 3,5,10,12,14,15 Although other ankle replacement systems have been studied, 1,9 this retrospective study details our results with the Agility total ankle and examines our clinical and radiographic experience and the possible reasons for the failures.
Materials and Methods
Patient Demographics
Between April, 1998, and March, 2002, 65 primary total ankle replacements using the Agility total ankle were performed in 64 patients at this institution by the senior author (JSG). The average followup was 3.3 (range 2.0 to 5.9) years. One patient died 2 years after the replacement, one patient declined to participate in the study, and one patient was lost to followup. Sixty-two total ankles, therefore, were evaluated in 61 patients (34 right ankles and 28 left ankles in 22 men and 39 women). The mean age at surgery was 54.5 (range 28 to 77) years. We examined seven parameters as they related to patient outcome: (1) patient age, (2) whether the patient had a prior procedure as part of a staged approach to ankle replacement, (3) the cause of arthritis, (4) smoking status, (5) methotrexate use, (6) diabetes, and (7) the size of the prosthesis used. Endpoints for this study were amputation, arthrodesis, osteochondral allograft, total ankle replacement, 8 or revision of either or both components. Each of the patients was contacted and completed the Medical Outcome Study 36-item Short-Form Health Survey (SF-36). 17,18 This generic health measure assesses health-related quality of life outcomes and has been previously shown to be both valid and reliable. 5,6,7,15,16 Radiographic and chart records also were reviewed for each patient. End-stage degenerative joint disease included post-traumatic arthritis (PTA), osteoarthritis (OA), rheumatoid arthritis (RA), post-polio syndrome, and adult clubfoot.
Of the 62 ankle replacements, 22 were the recipients of a prior procedure for an identified hindfoot malalignment or pantalar arthrosis. These patients received one or more of the following procedures: calcaneal osteotomies, subtalar arthrodesis, or triple arthrodesis. Additionally, nine patients were preoperative smokers and four had diabetes. Three of the 10 patients with RA were taking methotrexate that was discontinued 1 week before the procedure.
Operative Technique
The total ankle replacement was performed through an anterior incision between the extensor hallucis longus and anterior tibial tendons. All but the first 20 procedures were done with chamfer cuts on the talus to limit submalleolar impingement. Several methods for fusing the syndesmosis were employed over the series consisting of iliac crest bone graft and later the use of Platelet Concentrate System (DePuy, Warsaw, IN). The lateral cortex of the tibia and the medial cortex of the fibula were debrided to aid in fusion. The method of syndesmotic fixation progressed from two screws to the application of a titanium plate. Refinement of the technique included the early adoption of a lateral fibular plate to enhance syndesmotic fusion.
Statistical Methods
The Kaplan-Meier survivorship curve was estimated from the entire series of 65 ankles including the 95% confidence intervals. ANOVA was used to examine the differences in ages between PTA, OA, and RA groups. The remaining category of post-polio and adult clubfoot containing only two patients representing three ankles was omitted because of the small sample size.
Causes of ankle arthritis and endpoint reached
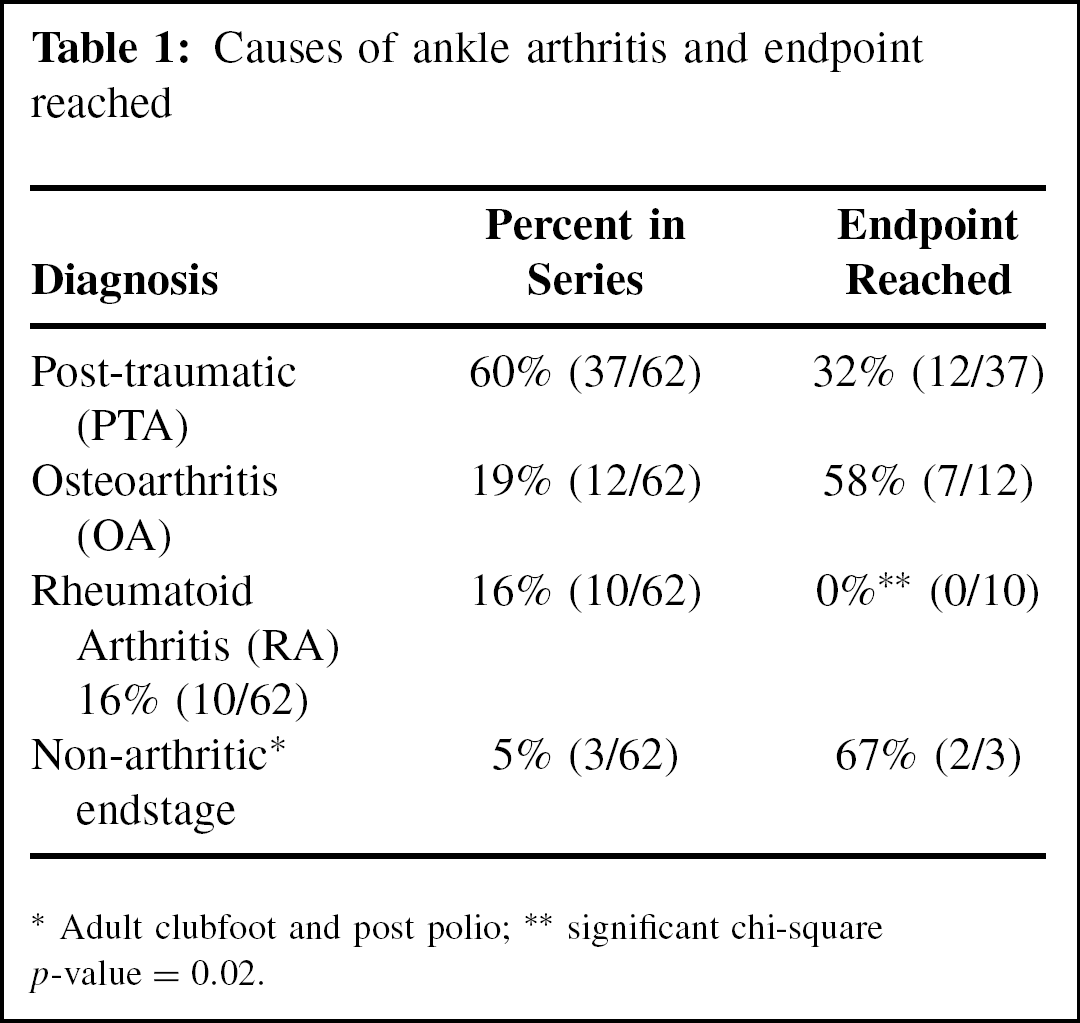
Adult clubfoot and post polio
significant chi-square p-value = 0.02.
A Student's t-test was used to examine whether age was a predictive factor within PTA or OA for predicting failure as well as examining the mean time to failure within a group.
Comparative statistics were calculated for the various clinical outcomes between different groups defined by cause of arthritis, size of the prosthesis, and SF-36 component scores using the chi-square test. SF-36 has component scores for Physical Functioning, Role Physical, Bodily Pain, General Health, Vitality, Social Functioning, Role Emotional, Mental Health, Physical Summary and Mental Summary.
Component scores of the SF-36 were used by grouping normal and high responses together and then comparing them to patients who scored low.
Results
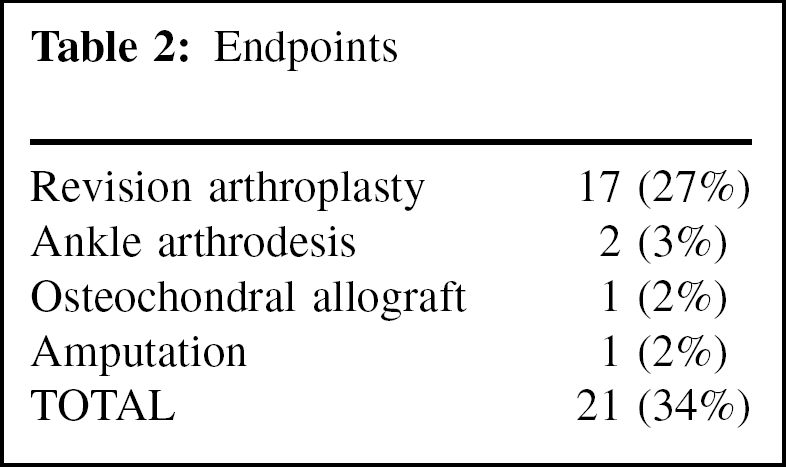
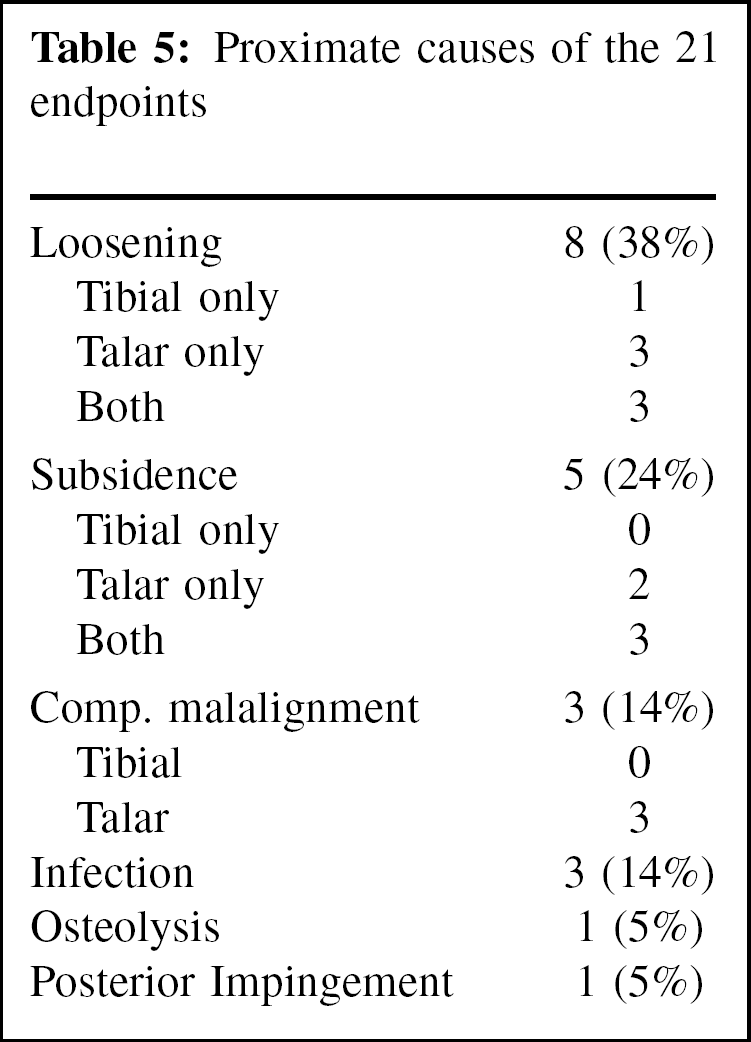
The endpoint rate is summarized in Table 1 and shows that none of the patients with RA reached an endpoint. This finding was statistically significant (p = 0.02). The 21 failures or endpoints reached are summarized in Table 2.
A Kaplan-Meier survivorship curve (Figure 1) was estimated using all 65 ankles by censoring the patients after they were lost to followup. At the end of the first year, 91% of total ankles remained with a 95% confidence interval between 98% and 83%. At the end of the 3 years the survivorship percentage dropped to 70% and then at the end of the 6 years the survivorship was 67%.
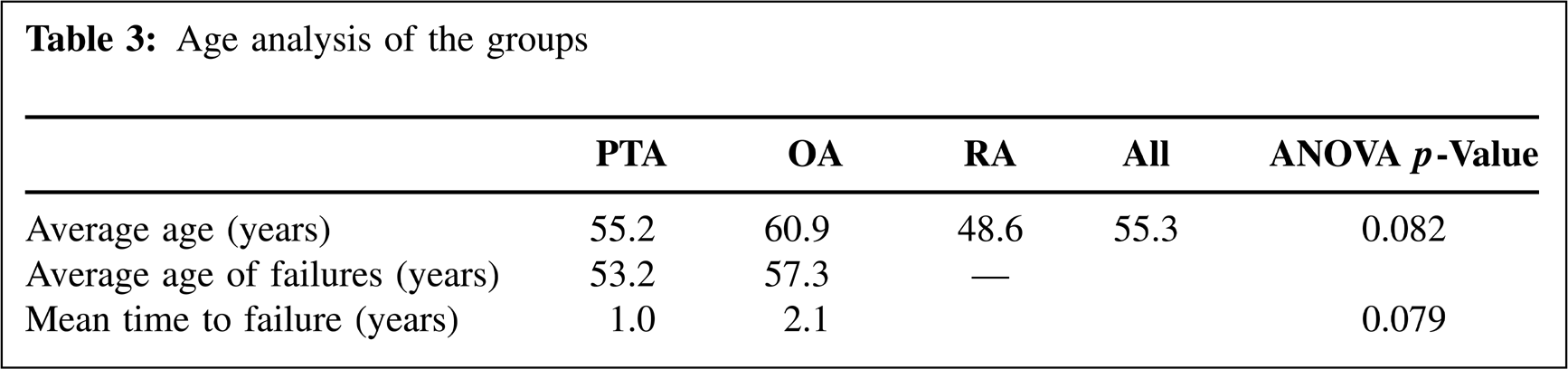
The average age of the patients at the time of ankle replacement was 54.5 years, and the average age of the patients with total ankles that failed was 53.4 years. An analysis of the age of patients revealed that the RA group was composed of younger patients. The average age of the entire group is 54.4 years, but when the two patients with post-polio and adult clubfoot were excluded, the average age of the group was 55.3 years. ANOVA demonstrated differences in the mean age between the remaining three groups and approached significance with a p-value of 0.082. The averages of the ages of the groups are summarized in Table 3.
The ages of the patients who had a failed implant in the OA and PTA groups were averaged to see if age was predictive of outcome. When compared with the group average, the OA subgroup that failed was nearly statistically significant (p = 0.079). The failed subgroup of the PTA category had no significance, and this is also summarized in Table 3.
Endpoints
Age analysis of the groups
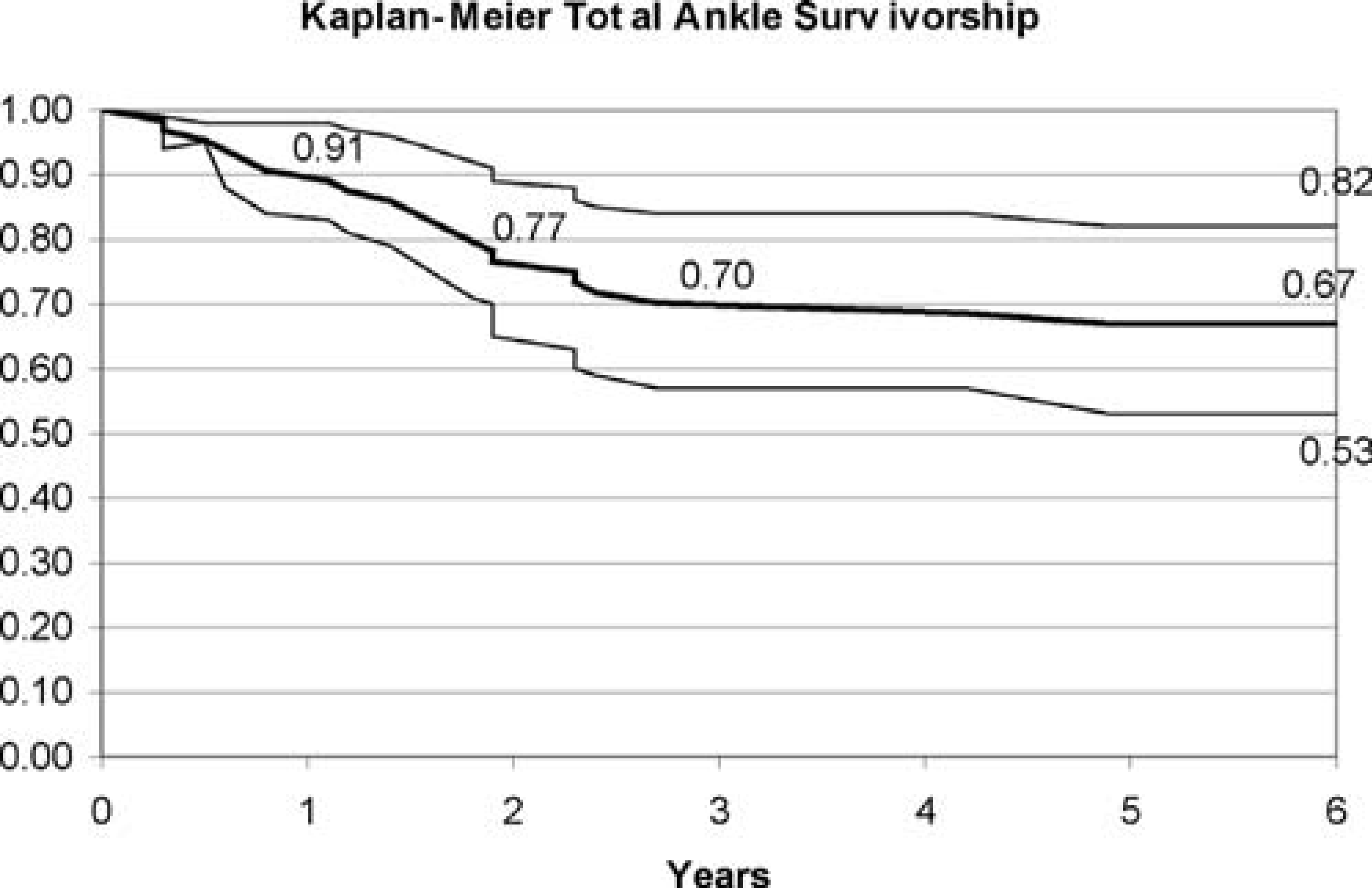
Kaplan-Meier survivorship curve for Agility total ankle replacement.
We examined the outcome with relation to prior procedures as part of a staged approach to ankle replacement surgery. Patients with hindfoot malalignment or pantalar arthritis who received calcaneal osteotomies or subtalar or triple arthrodesis were compared with patients who had not received any of those procedures. The question studied was whether premature failure of total ankle replacement is related to hindfoot alignment or arthritic pain generators.
The time to first revision of each patient whose total ankle failed revealed that the mean time to failure in the PTA group was 2.1 years while the mean time to failure in the OA group was 1 year. A Student t-test analysis revealed a near significant p-value of 0.079.
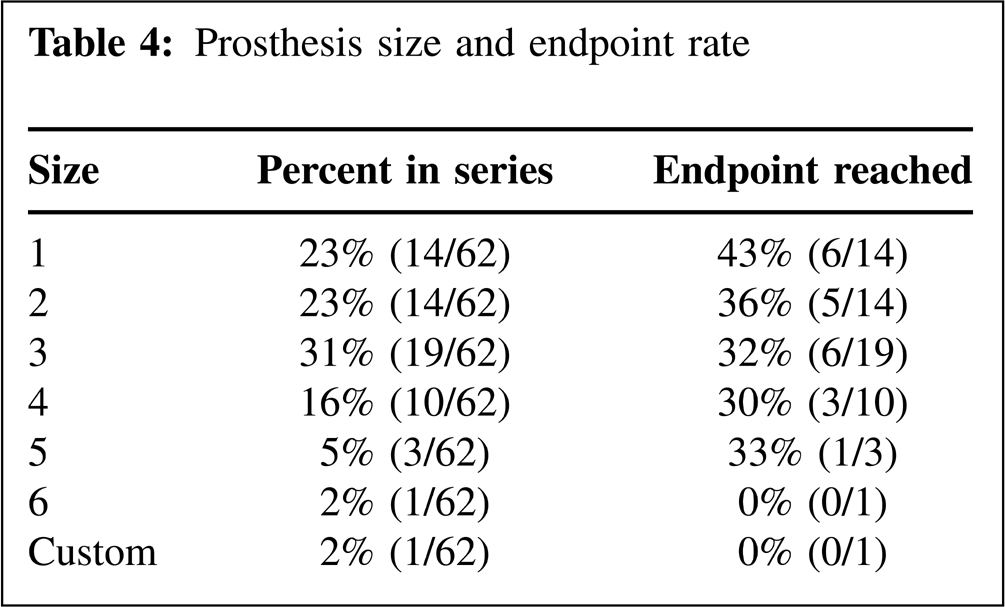
Prosthesis size and endpoint rate
The outcome for patients who had prior procedures revealed that there was no statistical difference in the outcome between the two groups of patients and that 41% (9/22) of patients with prior procedures reached an endpoint versus 30% (12/40) of those without.
There were nine superficial wound complications and three deep infections in 11 of 64 patients (17%) as one patient had both a superficial and deep infection that required amputation. Of the nine superficial wound complications, one was at the site of the lateral incision, six at the site of anterior incision, and two at both incisions.
Of the three deep infections, two resolved after a two-stage revision consisting of an antibiotic spacer. Two of the 11 patients with wound complications were patients who smoked; however, the other seven who smoked did not have wound complications. Additionally, of nine patients who smoked, three had implant failure. This was equivalent to the overall rate of reaching an endpoint for the entire series of patients.
Three of the RA patients had been taking methotrexate. Only one of these patients experienced a superficial wound infection of the lateral incision, and this patient had also been taking prednisone. Owing to the small sample size, little significance can be attributed to this occurrence.
Of the four patients with diabetes in the series, two had implant failure. Three of the four patients with diabetes were in the PTA group and one patient was in the OA group. Both of the diabetic patients with failed implants were in the PTA group, were in their early 40s, and had size 3 implants. The causes were loosening and failure of ingrowth of both components. Again little significance can be attributed to this finding because of the small sample size. No patients with diabetes had any wound complications.
The sizes of the prostheses are summarized in Table 4, which includes the rate of failure for each size prosthesis. The rate of failure as a function of the size of the component demonstrated no statistical significance with chi-square analysis.
The causes for revisions as noted on the charts from intraoperative findings or from radiographic reviews are summarized in Table 5. Five revisions were for subsidence, and all five were size 1 prostheses. When examining the outcome with regard to the SF-36, it was apparent that the patients with RA scored low compared to PTA and OA diagnosis in the category of Bodily Pain. A high score in this category means no pain. So patients with RA reported higher limitations because of pain than patients in the PTA or OA groups;, however, the chi-square p-value was 0.095 and was limited by the power of the study. The RA group also scored consistently lower in categories of General Health, Vitality, and Physical Summary when compared with the other causes of arthritis. There were no trends for differences in Role Physical, Social Functioning, Role Emotional, Mental Health or Mental Summary Score.
Proximate causes of the 21 endpoints
The outcome of the comparison of component SF-36 scores between patients with prior procedures and those without showed that the only area where there was a significant difference was in the Role Physical component score with a p-value of 0.014. No other component scores approached significance when comparing patients with prior procedures with those who had not received a prior procedures.
Discussion
The concept of a prior procedure was reported by Spirt et al. 15 who coined a category, “complex total ankle arthroplasty,” that consisted of patients who had adjuvant surgical procedures for treatment of axial malalignment or instability at the same time or occasionally just before total ankle replacement. 15 In that study, the group requiring adjuvant procedures encompassed 58% of their patients, and their conclusion was that the adjuvant procedures did not increase (or decrease) the risk of failure. Our findings were similar and our conclusion was the same.
Two of four patients with diabetes who were in the PTA group had similar circumstances of failure despite the fact that none of the diabetic patients had wound complications or infection. One patient required a revision for talar loosening and one because of talar subsidence. As was noted, the small sample size precluded assigning any significance to this finding. Perhaps other published series of the Agility total ankle implant might contain information concerning failure of ingrowth that may shed light on this situation.
Subsidence was the attributed cause of revision in five and all were size 1 prostheses. Of the 14 patients who received a size 1 prosthesis, six required revision. Five of the six had subsidence. The sixth patient required revision secondary to infection. Overall the size 1 prostheses had an increased rate of failure representing six of the 21 endpoints reached in the study. Although the size 1 failed at a rate of 43%, it was not statistically significant when compared to failure rates associated with the other sizes as detailed in Table 4. However, a trend was noted, but the significance was limited by the power of the study. Spirt et al. 15 did not review the sizes of prostheses that failed in their study. Pyevitch et al. 12 also did not indicate the sizes of the failed prostheses. 12 Knecht et al. 5 indicated that of the 14 major revisions in their 132 ankles, five failed because of impaction or settling, but no sizes were noted. Earlier versions of the prosthesis had a narrower posterior dimension of the talar component, giving it a trapezoidal shape when viewed from below. In 2001, the talar component was modified and offered as a revision component by increasing the posterior dimension, creating a more rectangular shape and a larger surface area for bone ingrowth. This modification should be considered as the primary component in small ankles requiring size 1 prostheses.
Using regression analysis, an age of younger than 54 years was previously identified as a predictive factor for a poor outcome with a greater likelihood of reoperation and ultimate failure. 13 Our results agree only in the patients with OA. Patients who had implant failure were almost statistically younger (p = 0.067) than those without failure. However, there was no association noted in the average age of the subgroup of failed ankles within the PTA group. Additionally, the RA group with an average age of 49 years was the youngest group (p = 0.082) used in the analysis, and no failures occurred in that group. Our results suggest that age alone is not a reliable predictor, but when combined with a specific diagnosis may offer some predictive value.
With regard to interpreting the results of the SF-36 component scores, it is apparent that RA patients were more apt to be pleased solely with the reduction in pain that the total ankle replacement might bring because their physical health already limits their function. Nishiskawa et al. 11 upheld this finding with AOFAS scores and noted that although clinical results were poor, patient satisfaction was not. Additionally, Unger et. Al. 16 also found 83% satisfactory results in 21 patients with cemented total ankles with a minimum of 2-year followup.
The SF-36 component scores were more mixed in PTA and OA patients who were more apt to be disappointed with limitations that the total ankle imposed on them, because these patients tended to be healthier and more active. Although pain may have been the primary indication for the ankle replacement, this study was limited because there was no preoperative pain score for comparison. However, the patients with PTA generally noted that the pain postoperatively was still higher than they expected.
The only component SF-36 score with a significant difference between patients with a prior procedure and those without was the Role Physical component score. In this component, most patients with a prior fusion scored low, indicating that they had more difficulty with work or other daily activities as a result of physical health. However, the Physical Function component, which asks about specific functions such as bathing, dressing, walking, climbing stairs, bending, lifting weights, and moderate or intense activities, was not significantly different. So despite nearly equivalent scores on individual functions, the patients with prior procedures had more difficulty with work and other daily activities.
The survivorship in the current study was similar to that of Spirt et al. 15 whose 5-year survivorship was 80% and ultimate failure rate (defined as revision or removal of components) was 11%. 15 The Kaplan-Meier survivorship curve of Figure 1 shows two discrete survivorship slopes in the current study. The first 2 years reflect early failures. About one in four ankle replacements failed in this series by the end of the second year. After the initial slope, the rate of failure decreased. The overall revision rate of 34% represents the challenges that accompany this procedure and includes all revisions, arthrodeses and an amputation secondary to infection. Had the early cases been excluded, our overall outcome would certainly have been better in terms of failure rate. We believe that outcomes improve with surgeon experience and that patient selection for this procedure is crucial in bringing total ankle outcomes closer to that of total hip or knee replacement statistics. While data by Spirt et al. 15 was similar, Saltzman and Alvine had a flatter slope initially and overall had better survival even up to 9 years out. 5,13,15
Perioperative complications with this device have been described in other articles and are generally considered to be related to the experience of the surgeon. 3,10,14,15 However, the effect of improvements in the learning curve may apply only within the first 50 cases, and subsequent improvement was never demonstrated. 15 In this study, none of the earliest cases was excluded, and all but four (6%) of the total ankles are still implanted. Modifications in the device and instrumentation, experience in the technique, and refinements in the patient selection all work to increase the survivorship, function, and satisfaction of the procedure.