
Abstract
Background: This study tested the hypothesis that modification of the standard technique of hindfoot arthrodesis with the use of a wedge-shaped tricortical allograft would improve the amount of correction of pes planovalgus deformity. The results were compared to previous reports. Methods: Between 1998 and 2005, the senior author (LBC) performed 13 hindfoot arthrodeses on 12 patients using an allograft to improve correction of the deformity for severe, painful pes planovalgus deformity. The average patient age was 55 (range 27 to 77) years. There were seven women and five men. The indications were posterior tibial tendon dysfunction (seven feet), rheumatoid arthritis (three feet), post-traumatic arthritis and deformity (one foot), congenital pes planovalgus (one foot), and tarsal coalition (one foot). Results: Twelve of 13 feet achieved union by 12 weeks postoperatively. There was one nonunion. The average time to fusion was 12 weeks. All 12 patients were satisfied with the results of the operation. The average postoperative American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot score was 87 points, and the AOFAS Midfoot score was 85 points. Preoperative and postoperative radiographs were compared to evaluate correction of deformity. On lateral weightbearing views, the talo-first metatarsal angle improved from 15 to 6 degrees, and the lateral talocalcaneal angle improved from 48 to 35 degrees. On anteroposterior views, the talo-first metatarsal angle improved from 17 to 7 degrees, the talonavicular coverage decreased from 28 to 13 degrees, and the talocalcaneal angle improved from 23 to 13 degrees. Conclusions: A simple modification of the addition of allograft to a common procedure of hindfoot arthrodesis to treat severe, painful pes planovalgus results is reliable and offers satisfactory correction.
INTRODUCTION
The etiology of pes planovalgus deformity in adults is varied. The most common cause is posterior tibial tendon dysfunction, and other disorders include rheumatoid arthritis, tarsal coalition, idiopathic, and post-traumatic arthritis. Pes planovalgus deformity often involves several biomechanical abnormalities, including lateral column shortening in relation to the medial column, lateral subluxation of the navicular on the talus, hyperpronation from increased eversion of the subtalar joint, and valgus orientation of the calcaneus. 4,8,19 Pes planovalgus may be flexible or rigid, as well as painless or symptomatic. Patients who progress to severe or fixed deformities may have discomfort in one or more of the following areas: medial or lateral midfoot and medial or lateral hindfoot. In symptomatic patients, treatment with analgesic medication, shoe modification with braces or inserts, and activity modification may be helpful. When nonoperative management fails, operative reconstruction may be indicated. Traditionally, subtalar or triple arthrodesis is done in an attempt to correct the hindfoot deformity. Studies by Maenpaa et al. 11 and Pell et al. 15 found that the degree of correction of the pes planus deformity correlates with postoperative outcome both clinically and radiographically.
The purpose of this study was to retrospectively evaluate patients in a consecutive series with severe, painful pes planovalgus who were treated with hindfoot arthrodesis using a tricortical wedge-shaped allograft. The hypothesis was that this modification would improve correction. A corollary purpose in this study was to compare patient satisfaction and degree of correction to previous reports.
MATERIALS AND METHODS
Institutional review board approval was obtained for this retrospective review on 15 feet in 14 consecutive patients who underwent hindfoot arthrodesis for painful severe pes planovalgus deformity between 1998 and 2005. Two patients were excluded because one placed weight on the operated foot immediately and had loss of fixation and correction. The other patient declined followup because she was elderly with multiple medical problems and did not have transportation for the 200-mile travel. The average age of the remaining study group of 13 feet in 12 patients was 55 (range 27 to 77) years. There were seven women and five men. The etiology of the deformity was varied and included posterior tibial tendon dysfunction in seven feet, rheumatoid arthritis in three feet, post-traumatic arthritis and deformity in one foot, congenital pes planovalgus in one foot, and tarsal coalition in one foot. All patients had severe pain in the midfoot or hindfoot or both, which was worse with weightbearing activities. The average duration of symptoms was 43 (range 4 to 180) months. All patients were treated initially with nonoperative modalities, which included oral analgesics (nonsteroidal anti-inflammatory medication), shoe inserts, braces, and activity modification. The average followup from the time of the operation was 34 (range 12 to 70) months.
All surgeries were performed by the same surgeon (LBC) using a single incision technique for subtalar fusion (6 cases), and a two-incision technique for triple arthrodesis (7 cases). Patients were evaluated preoperatively to determine the extent of the arthrodesis to be done. In patients with the deformity primarily involving the subtalar joint, a subtalar arthrodesis was planned. However, if the deformity could not be corrected through the subtalar joint alone, the transverse tarsal joint was included in the arthrodesis. This was determined by placing the subtalar joint in 5 degrees of valgus, and if there was residual forefoot varus, the talonavicular and calcaneocuboid joints were included in the arthrodesis to ensure a plantigrade foot.
All patients were interviewed and examined at the time of the last followup. Questions addressed severity and location of pain, use of analgesic medications, function, shoe issues, need for ambulatory aids, satisfaction, and whether or not the patient would repeat the procedure. In addition, patients were evaluated using the American Orthopaedic Foot and Ankle Society (AOFAS) Hindfoot and Midfoot Scales. 9 The preoperative scores were not determined retrospectively. 18,20 Physical examination evaluated tenderness, edema, erythema, callus, bony prominences, and alignment deformities.
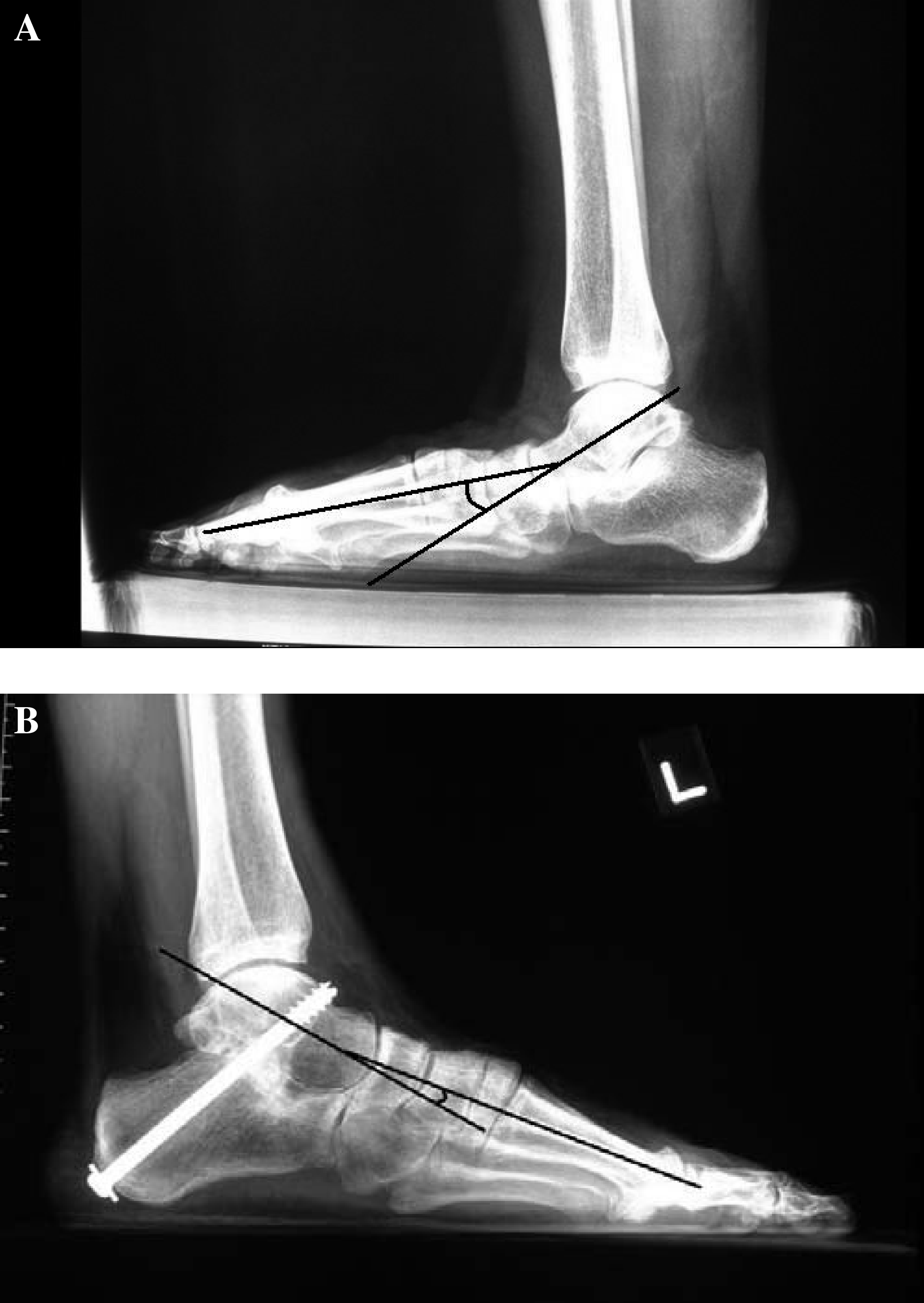
Weightbearing preoperative and postoperative radiographs were obtained of the foot and ankle using standard techniques. A goniometer was used for all angle measurements on anteroposterior and lateral views, as described by Sangeorzan et al. 17 Using the anteroposterior views, the talo-first metatarsal angle, talonavicular coverage, angle and talocalcaneal were measured. The talo-first metatarsal angle was measured by using the long axis of the first metatarsal and the long axis of the talus. The talonavicular coverage angle was measured using one line perpendicular to the proximal edges of the navicular and another line drawn between the medial and lateral margins of the talar head articular surface. The talocalcaneal angle was measured using the longitudinal axis of the talus and the longitudinal axis of the calcaneus. Using the lateral view, the talo-first metatarsal angle and lateral talocalcaneal angles were measured. The talo-first metatarsal angle was measured using the longitudinal axis of the first metatarsal and the long axis of the talus. The lateral talocalcaneal angle was measured using the long axis of the talus and the inferior margin of the calcaneus.
Radiographs also were used to determine fusion or nonunion. Evidence of bridging trabeculae was indicative of fusion, whereas persistent lucency was considered to be a nonunion.
Operative Technique
For a subtalar arthrodesis, the technique follows the description by Haskell et al. 6 After general or regional anesthesia, with the patient supine, a padded bump was placed under the ipsilateral hip and a tourniquet on the upper thigh. An incision was made over the lateral aspect of the hindfoot from the distal tip of the fibula to the base of the fourth metatarsal. The sural nerve was identified and protected for the entire procedure. The extensor digitorum brevis was elevated from its origin to expose the sinus tarsi and subtalar joint. The contents of the sinus tarsi and articular cartilage were removed using small curets and osteotomes. A lamina spreader was placed in the sinus tarsi to improve exposure of the posterior, middle, and anterior facets of the subtalar joint. The subchondral bone was feathered with an osteotome. This was done by angling the osteotome about 45 degrees and fracturing the subchondral surface to make a fish scale or roof tile appearance.
The technique described by Mann 12 was used for the triple arthrodesis. Through the distal aspect of the lateral incision the calcaneocuboid joint and the joint surface were prepared in a similar manner. Next, a medial incision was made over the talonavicular joint between the anterior tibial and posterior tibial tendons. The joint was exposed through a capsulotomy, the articular cartilage was removed, and the subchondral surface was feathered with an osteotome. A lamina spreader or Freer elevator may be used to wedge open the joint to improve exposure of the lateral aspect. The allograft was prepared on the back table (Figure 1) using an oscillating saw. The allograft was tricortical from the iliac crest and cut into a wedge shape, with the lateral side approximately 1 cm in height. The graft was placed at the sinus tarsi and posterior facet with the assistance of a lamina spreader (Figure 2). The effect was an opening wedge to correct the hindfoot valgus deformity to the desired position of 5 degrees of valgus. Because the tricortical structure of the graft, compression was obtained with a subtalar lag screw without risk of collapse or extrusion of the graft.

The tricortical iliac crest allograft is cut into a wedge using a sagittal saw, with the lateral side measuring approximately 1 cm. The effect is an “opening wedge” laterally to correct the hindfoot deformity to 5 degrees of valgus.

Intraoperative photograph shows a lamina spreader used to facilitate placement of the tricortical wedge shaped allograft in the posterior facet of the subtalar joint and sinus tarsi.
The foot was maintained in 5 degrees of valgus and 0 degrees of plantarflexion as rigid internal fixation was placed. Using a guide wire and intraoperative fluoroscan imaging, a single 6.5-mm or 7.3-mm cannulated screw with washer was placed in the calcaneus just posterior to the plantar weightbearing surface. The screw exited at the talar neck, distal to the tibiotalar joint (Figure 4). With the triple arthrodesis, the talonavicular and calcaneocuboid joints were included in the arthrodesis. The foot was held in a plantigrade position, correcting any forefoot supination and abduction. The amount of supination was 0 degrees so the foot was plantigrade, and the amount of external rotation matched the contralateral foot, usually 10 degrees. Two 4.0-mm or 4.5-mm cannulated screws were placed from the distal and medial navicular into the talar head and neck with the assistance of the guide wires and fluoroscopy. The calcaneocuboid joint was fixed with two 4.0-mm or 4.5-mm cannulated screws or several 16-mm by 25-mm bone staples placed laterally. A small drain was placed in the lateral incision. The extremity was placed in a bulky Jones dressing and plaster splint with the foot and ankle maintained at neutral dorsiflexion and plantarflexion.
Postoperative Treatment
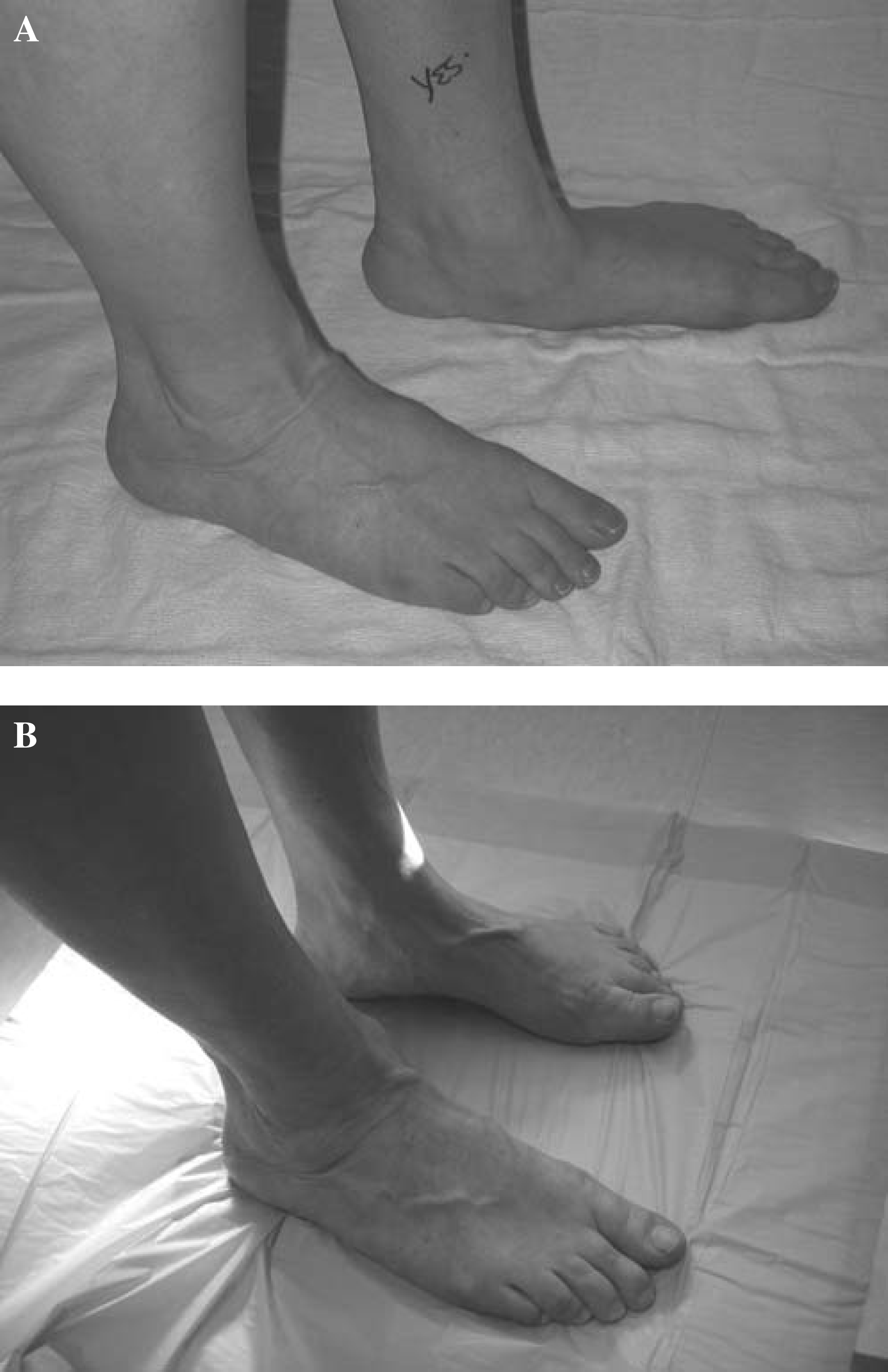
The drain was removed after 24 hours, and the splint and dressings removed after 10 to 14 days. The sutures were removed, and the patient was placed in a short-leg fiberglass cast. The patient continued nonweightbearing until 6 weeks postoperatively, whereupon radiographs were obtained. With adequate evidence of radiographic healing, the patient was placed in a short-leg fiberglass cast and allowed to bear weight. At 12 weeks postoperatively, repeat radiographs of the foot were obtained to determine healing. The patient could then be permitted to bear weight as tolerated in a comfortable, well-cushioned wide shoe (Figures 3 and 4).
RESULTS
Eleven of the 13 feet had no pain; two had mild pain. No patient used pain medication. Seven patients had no limitations with activity, five patients had minimal limitations, and one patient had difficulty with activities of daily living. The latter patient used a cane for ambulation. Four patients walked with a mild limp. All patients wore ordinary store bought shoes. None of the patients used an insert or brace. Six patients had mild residual swelling. The hindfoot valgus was measured with a goniometer with the patient standing; the average was 6 degrees. One patient had a bony prominence at the cuboid that led to callus formation, but it was not painful or tender to palpation. Two patients had a residual pes planus deformity, and one patient had a rocker bottom pes planovalgus deformity. These patients had unlimited activity levels and no pain from their deformities. All 12 patients were satisfied with the results of the operation. One patient stated she would not repeat the procedure because of the long postoperative course. A second patient stated he would repeat the procedure with reservations but was satisfied with the result. The average postoperative AOFAS Ankle-Hindfoot score was 87 points, and the Midfoot score was 85 points.
Twelve of 13 feet achieved union by 12 weeks postoperatively. Preoperative and postoperative radiographs were compared to evaluate correction of deformity. On the anteroposterior views, the talo-first metatarsal angle improved from 17 to 7 degrees, the talonavicular coverage decreased from 28 to 13 degrees, and the talocalcaneal angle improved from 23 to 13 degrees. On the lateral weightbearing views, the talo-first metatarsal angle improved from 15 to 6 degrees, and the lateral talocalcaneal angle improved from 48 to 35 degrees.
One patient developed a nonunion of the subtalar joint and was treated with a revision, which successfully fused after the second procedure. Five patients had removal of symptomatic hardware. There were no cases of nerve injury, infections, wound complications, graft collapse, or extrusion.
DISCUSSION
Historically, treatment of severe, painful pes planovalgus deformity with hindfoot arthrodesis has led to successful outcome. 3,4,7,10,19 Soft-tissue procedures alone cannot correct bony deformities. While joint sparing procedures, such as lateral column lengthening, plantarflexion osteotomy of the medial cuneiform, the Evans procedure, and posterior calcaneal osteotomies, have been used, 8 full correction of severe deformities may not be achieved. 10,12,14,17 Limited arthrodeses also have been described, such as isolated talonavicular, calcaneocuboid, and subtalar arthrodesis, and medial column arthrodesis. The procedure of choice will depend on the deformity and the philosophy and experience of the surgeon. 19 Between 1989 and 1996, Fortin and Walling 4 evaluated 29 patients who underwent triple arthrodesis for stage III or IV adult acquired pes planus deformity. With 25 patients available for 2-year followup evaluation, radiographic improvement was found in the talo-first metatarsal angle of 18 degrees, lateral talocalcaneal angle of 13 degrees, and anteroposterior talo-first metatarsal angle of 15 degrees. In addition, they reported an average improvement of 36 points using the AOFAS Ankle-Hindfoot Scale. Twenty-two of the 25 patients considered their procedure a success, two were satisfied but had reservations, and one was dissatisfied.
In another report on the results of triple arthrodesis by Coetzee et al., 3 12 feet in 11 patients with long-standing, rigid deformity from posterior tibial tendon dysfunction were evaluated. 3 Radiographic parameters showed improvements in the lateral talo-first metatarsal angle of 31 degrees, calcaneal pitch of 11 degrees, anteroposterior talo-first metatarsal angle of 35 degrees. The AOFAS Ankle-Hindfoot scores improved from an average of 30 points preoperatively to 74 points postoperatively. In a similar study, Jarde et al. 7 reviewed 20 patients treated with triple arthrodesis for valgus flatfoot deformity secondary to posterior tibial tendon dysfunction. Eighteen of 20 patients had either fair, good, or excellent results.
An important finding is that outcome of fusion is highly dependent on postoperative alignment of the foot. Pell et al. 15 followed 183 patients who had triple arthrodesis for an average of 5.7 years postoperatively. The diagnosis included post-traumatic changes, rheumatoid arthritis, rupture of the posterior tibial tendon, pes planus, and neuromuscular imbalance. They found that there was a high correlation between patient satisfaction and postoperative foot alignment.
Moreover, poor postoperative alignment has been shown to result in poor outcome. Maenpaa et al. 11 reviewed 307 primary triple arthrodeses performed in patients with rheumatoid arthritis. The authors evaluated 21 cases deemed “failures” since reoperation was required. The operative technique, correction of hindfoot deformity, use of bone grafts, and cast immobilization were analyzed. They found that the most common cause of failure (12 of 21 cases) was inadequate correction and repositioning of hindfoot deformity. They concluded that achieving solid union does not seem to be problematic, but malunion is a potential hazard if the operative technique is inadequate.
The literature reveals that there is substantial data regarding subtalar and triple arthrodesis in general, but the method of evaluation of alignment after arthrodesis varies widely. This is in part due to different radiographic measurement techniques as well as a variety of angles available for analysis of alignment. Additionally, some studies report the level of correction as the number of degrees of correction as opposed to the actual postoperative measured angle. Because of these factors, comparison of our data with historical data was difficult.
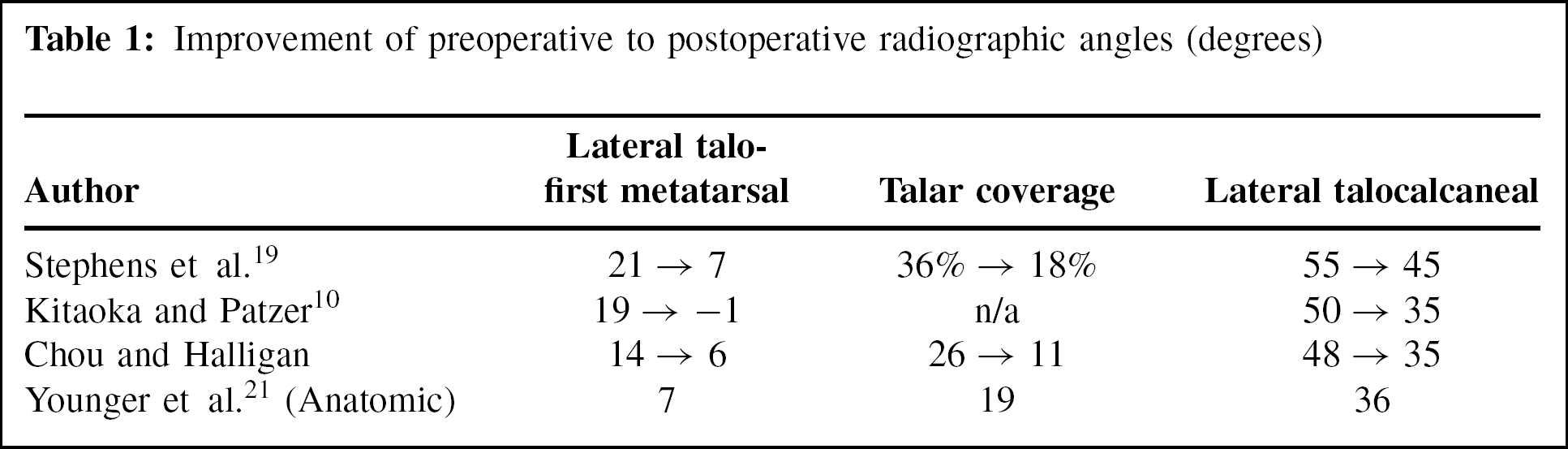
Nevertheless, two studies were found that included data that could be compared to ours. Stephens et al. 19 performed 25 subtalar arthrodeses in 24 patients for acquired pes planus. All patients had middle to late stage II deformity. The AOFAS scores improved an average of 38.3 points to 77.3. All patients elected to undergo the procedure again. Radiographic improvements included lateral talo-first metatarsal angle from 21 to 7 degrees, lateral talocalcaneal angle from 55 to 45 degrees, and percent of talar uncoverage from 36% to 18%. Five feet still had slight residual valgus postoperatively.
Kitaoka and Patzer 10 performed 21 subtalar arthrodeses in 21 consecutive patients for posterior tibial tendon dysfunction and flexible pes planus. All patients had successful union. Radiographic improvement was seen in the lateral talometatarsal angle from 19 to −1 degrees, the lateral talocalcaneal angle from 50 to 35 degrees, and the lateral tibiotalar angle from 121 to 107 degrees. No patient required rigid ankle braces, but 11 of the 21 patients had residual pain postoperatively.
These results are similar to those obtained in this study and are summarized in Table 1. As a result, we think that this technique offers an effective and reliable method of correction in even the most advanced cases of pes planovalgus.
Improvement of preoperative to postoperative radiographic angles (degrees)
The use of bone graft with hindfoot arthrodesis has been reported previously in the literature. 1,2,5 In 1943, Gallie 5 treated malunited, symptomatic calcaneal fractures with subtalar arthrodesis. He used two segments of bone graft from the anteromedial surface of the tibia into the fusion site to prevent further reduction of the height of the foot. This technique was modified by Carr et al. 2 for treatment of late complications of os calcis fractures. Specifically, the authors treated the decreased calcaneal body height, which results in a shortened Achilles lever arm, limb length discrepancy, and difficulty with the malleoli contacting the shoe counter. The operative procedure uses a femoral distractor to open the subtalar joint to allow placement of a block of tricortical posterior iliac crest graft as high as 2.5 cm. The results were improvement of the lateral talocalcaneal angle from 25 to 36 degrees, and increase in the height of the heel in 6 of the 16 feet of 1 cm. There were 15 complications listed, with 10 feet requiring secondary operations. The most frequent secondary operation was hardware removal (seven of 16 feet).
The use of bone block fusion was further modified by Amendola et al. 1 for treatment of subtalar arthrosis after a calcaneal fracture. The operative technique employed a lamina spreader to increase the opening of the subtalar joint. The bone graft was fashioned as bicortical struts from the posterior superior iliac spine and placed in the subtalar joint to restore foot height and talar inclination. The authors showed that using interposition iliac crest bone graft the heel height was restored with 100% union rate. The procedure described by Amendola et al. 1 was further modified for use in hindfoot arthrodesis for the treatment of severe, painful pes planovalgus deformity as described in this study. In some cases of triple or subtalar arthrodesis without supplemental structural graft, full correction of the deformity may be incomplete or some loss of correction may occur. The addition of a tricortical interposition wedge shaped iliac crest allograft has been shown to improve the deformity and help prevent loss of correction.
Noteworthy is the high rate of removing symptomatic hardware after hindfoot arthrodesis. In the previously mentioned study by Coetzee et al., 3 three of the 12 patients required hardware removal. In the series by Carr et al., 2 implant removal as a second operation occurred in 7 of the 16 feet. Similarly, Sammarco et al. 16 found that seven of 18 patients required hardware removal. Therefore, while five of our 12 patients required a second operation, this is likely more attributable to prominent hardware used in hindfoot fusion as opposed to our specific technique.
There are several limitations to our study. First, the number of subjects in the study was limited; there were only 12 patients over an 8-year study period. Patients with this deformity are initially treated with nonoperative modalities, and only patients who continue to have severe pain and disability were offered operative reconstruction. Second, there was no control group, again because of the small number of patients who had indications for this operation. Thus, we were forced to compare the results with historical data. Third, preoperative AOFAS scores were not collected retrospectively, as this has been shown to be inaccurate. 18,20 Therefore, we could not compare preoperative subjective questions with postoperative ones. Future patients undergoing this procedure will be evaluated preoperatively with the AOFAS scale. Lastly, one could criticize this study for including both triple and subtalar arthrodesis. It is preferable to perform an isolated subtalar arthrodesis to preserve some motion at the transverse tarsal joint while improving the stability and deformity of the arch. In a severe deformity that has residual abnormality, such as forefoot supination malposition when the subtalar joint is reduced, a triple arthrodesis is necessary to obtain full correction. The tricortical wedge shaped allograft is placed in the subtalar joint and sinus tarsi, whether or not the transverse tarsal joint is fused. Hence, patients who underwent either procedure were included in this study.
In conclusion, this simple modification of the common procedure of hindfoot arthrodesis to treat severe, painful pes planovalgus results in reliable and satisfactory correction. The literature reports a high union rate of up to 100% for arthrodesis of the subtalar joint. 1,10,13 The addition of a structural wedge of allograft has not shown to increase morbidity such as nonunion or delayed union.