
Abstract
Background: Much has been written about the effects of successful arterial bypass on forefoot surgery for ulceration and gangrene. This study examined the effects of the amputation site and timing on the arterial bypass graft site. Methods: We reviewed the records of all patients who had successful vascular bypass graft surgery and amputation at our institution, between October, 1995 and May, 2002. Thirty-eight procedures in 35 patients fit the criteria and were included in the study. Results: Thirty-five patients had successful vascular bypass graft surgery and forefoot amputation for gangrene or nonhealing ulceration. Three of these patients developed gangrene on the contralateral side and received similar treatment for that side. All of the wounds eventually healed. Healing time, rate of graft infection, and rate of wound dehiscence did not differ noticeably between patients with amputation immediately after arterial bypass and patients with amputation one or more days after arterial bypass. Infection at the bypass site occurred in two patients; their amputation sites were closed primarily. Wound dehiscence developed at the bypass site in one patient whose amputation site was closed by secondary intention. Although not statistically significant, the median healing time in patients treated with primary closure (37 days) was less than that in patients treated with closure by secondary intention (61 days; p = 0.09), and rates of graft infection and wound dehiscence did not differ between these two groups of patients. Conclusions: Amputation site wound closure may adversely affect the bypass graft, but results were not statistically significant. Treatment requires a closely coordinated team approach between the vascular surgeon and the orthopedic surgeon.
Introduction
Forefoot amputation associated with revascularization procedures for peripheral vascular insufficiency has become more commonplace. 22 As the population ages, the number of patients with peripheral vascular disease will increase, and forefoot amputation will continue to pose a challenge to surgeons in terms of timing and level of amputation. The goals of surgery in dysvascular patients with or without gangrene are eradication of infection, wound healing, and rehabilitation to the maximal functional level. Partial foot amputation is performed to maintain walking independence. A study of rehabilitation after lower extremity amputation showed that wounds rarely heal completely in this patient population. 11 Delayed wound healing appears to be the rule rather than the exception. Limiting the level of amputation has improved with the success of revascularization of more peripheral or distal vessels. 2,8,9
The purpose of this study was to evaluate the effect that both the timing and wound closure technique of foot amputation have on healing times and on the likelihood of graft infection and wound dehiscence and to determine if infection rates are higher and wound-healing problems more extensive at the bypass graft site if the foot amputation wound is closed primarily, if the wound is treated by delayed primary closure, or if the incision is allowed to heal by secondary intention.
The need for revascularization and limb salvage has been linked to a number of comorbid conditions: diabetes mellitus, end-stage renal disease requiring dialysis, acute arterial insufficiency as seen in embolization, extensive gangrene, extensive deep infection, severe coronary artery disease, history of stroke, elevated C-reactive protein level, heel gangrene, and multiple skin ulcerations. Patients with these disease processes tend to fare poorly, often requiring major amputation, including transfemoral amputation. 1,3 5,7,12,13,15,–19 21,23 Grafts must remain patent until the wound has healed or collateral blood flow has been established. 10,12,23 In some patients, if patency of the bypass graft is lost, subsequent development of collateral blood flow may prove sufficient to support the limb. There is little in the literature that examines the effect of primary closure, delayed closure, or healing by secondary intention on the vascular bypass operative sites.
A number of tests have been advocated for preoperative evaluation (before both revascularization and amputation) to help predict success for the amputation level. These include Doppler studies, radioisotope studies, ankle-brachial index, nailfold capillary microscopy, and transcutaneous oxygen pressure. 14,21 These have contributed to successful decision making by the surgeon.
Materials and Methods
With institutional review board approval, we reviewed the records of all patients who had successful vascular bypass graft surgery at our institution, between October, 1995, and May, 2002. Records were reviewed for the following characteristics: age, sex of patient, history of diabetes mellitus, serum albumin level, history of peripheral neuropathy, coronary artery disease, history of smoking, renal failure requiring dialysis, dry or wet gangrene or cellulitis, healing time of the amputation site, healing problems at the bypass graft site, infection of the graft, graft material (synthetic compared to autologous vein), the timing of the amputation in relation to the revascularization procedure, and treatment of the amputation site (primary closure, delayed primary closure, or healing by secondary intention).
The criteria for revascularization included critical lower extremity ischemia with the limb at risk, chronic symptomatic ischemia, and nonhealing wounds in the presence of ischemia. The ankle-brachial index, transcutaneous oximetry, and arteriography were used to evaluate the severity and location of disease and the potential ability to reestablish vascular perfusion to the extremity. Peripheral neuropathy was identified by Semmes-Weinstein 5.07 monofilament testing, electromyography, or both. Patient age, sex, history of diabetes mellitus, history of peripheral neuropathy, coronary artery disease, history of smoking, and chronic renal failure were considered important but not absolute contraindications for revascularization.
The level of amputation was based on a number of criteria. In patients who had amputation immediately after revascularization, the level was determined on the basis of viable tissue with no evidence of infection and bleeding at the time of surgery after all necrotic material had been removed. Wounds were routinely closed unless purulence or cellulitis was present. If infection was present in the form of cellulitis or purulence, the wounds were left open and later treated with delayed primary closure or healing by secondary intention. In patients whose amputation was done later, those with an ankle-brachial index of less than 0.5 or uncontrolled infection had transtibial or transfemoral amputation.
Statistical Analysis
Numerical data were summarized with the sample median and range. The Fisher exact test and Wilcoxon rank sum test were used to compare patient demographics and outcomes between groups. A Kruskal-Wallis rank sum test was used to compare healing time according to history of smoking. Kendall τ was used to examine the correlation between serum albumin levels at the time of amputation and healing time. For patients with a bilateral procedure, only the first was considered in statistical analysis. Statistical significance was determined at the 5% level.
Results
Between October, 1995, and May, 2002, a total of 144 peripheral vascular bypass procedures were performed. Of these, 38 procedures in 35 patients fit the criteria established for this study. Three patients had the same procedure on the contralateral side at a different time. These 35 patients presented with gangrene, ulceration, and sometimes accompanying cellulitis of one or more toes, resulting in amputation of involved digits, ray resection, or transmetatarsal amputation.
Table 1 shows patient demographics and outcomes according to wound treatment. Twenty-six of 35 patients were diabetic, 12 (46%) of whom had peripheral neuropathy. The three patients who underwent bilateral surgery were diabetic, and two had diabetic neuropathy. Twenty-one patients (60%) had severe coronary artery disease, and all three patients who underwent bilateral procedures had coronary artery disease. Only 10 patients never smoked; 18 were former smokers who quit smoking 4 months to 35 years before surgery; and seven patients were active smokers at the time of surgery. There was mild evidence of an imbalance in the distribution of smoking history between patients treated with primary closure and patients treated with secondary intention (p = 0.049). No other baseline characteristics differed noticeably between these two groups of patients.
Demographics and healing time according to wound treatment*
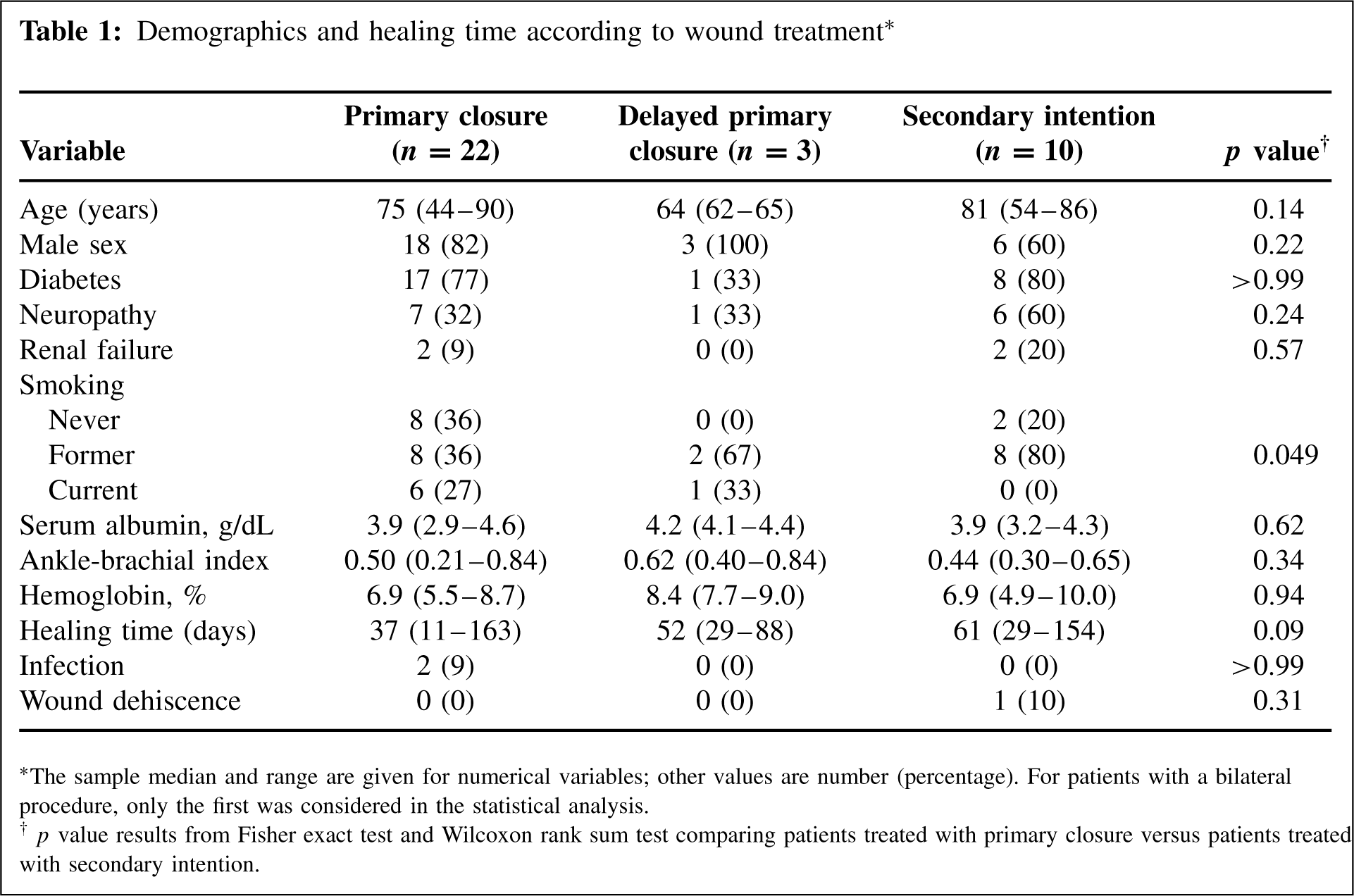
The sample median and range are given for numerical variables; other values are number (percentage). For patients with a bilateral procedure, only the first was considered in the statistical analysis.
p value results from Fisher exact test and Wilcoxon rank sum test comparing patients treated with primary closure versus patients treated with secondary intention.
Autologous saphenous veins were used in 25 graft procedures, and synthetic graft material was used in 13 procedures. The vascular bypass grafts consisted of 19 femoral-popliteal, six femoral-posterior tibial, four femoral-peroneal, three femoral-anterior tibial, three popliteal-tibial, two above-knee to below-knee popliteal, and one femoral-femoral artery bypass. All 35 patients had ankle-brachial index and arteriography studies performed, and oximetry testing was used in 11 patients. The ankle-brachial index at the ankle ranged from 0.21 to 0.84, with a median of 0.50.
The amputated digits were 15 great toes, eight second toes, four third toes, six fourth toes, and six fifth toes, and two were transmetatarsal amputations. The median healing time after amputation was 45 (range 11 to 163) days for all 38 limbs. Two limbs required revision of a toe amputation to a ray resection. One patient required revision of a two-toe amputation to a transmetatarsal amputation before successful healing.
Twenty-four amputations in 22 patients were treated by primary closure of the wound. Two patients in this group developed bypass graft infections believed to be from colonization of the foot gangrene or ulcer bacteria. These infections led to debridement of the bypass graft site followed by 6 weeks of parenteral antibiotics. The median healing time within this group was 37 (range 11 to 163) days.
Three patients’ amputation sites were treated by delayed primary closure 3 days after the primary amputation. None of these patients had cellulitis, and none had bypass graft site problems. Median healing time for this group was 52 (range 29 to 88) days.
Eleven amputation sites in 10 patients were left open to heal by secondary intention. One patient had wound dehiscence, requiring debridement, and the wound then healed by secondary intention. Median healing time in these patients was 61 (range 29 to 154) days, which is higher than the median healing time of 37 days in patients treated with primary closure, although the difference was not statistically significant (p = 0.09).
Table 2 shows patient baseline characteristics and outcomes according to timing of amputation in relation to the arterial bypass. In four limbs, amputation was done 1 to 275 days before revascularization. In 16 limbs, revascularization was followed immediately by amputation during the same anesthetic period. In 18 limbs, amputation occurred 1 to 65 days after revascularization. Bypass graft infection occurred in one patient who had amputation 24 days after revascularization and in one patient who had amputation 46 days after revascularization. The timing of the amputation demonstrated no remarkable difference in healing times (p = 0.91), graft infection rates (p = 0.49), or wound dehiscence rates (p = 0.45).
Demographics and outcomes according to amputation timing*
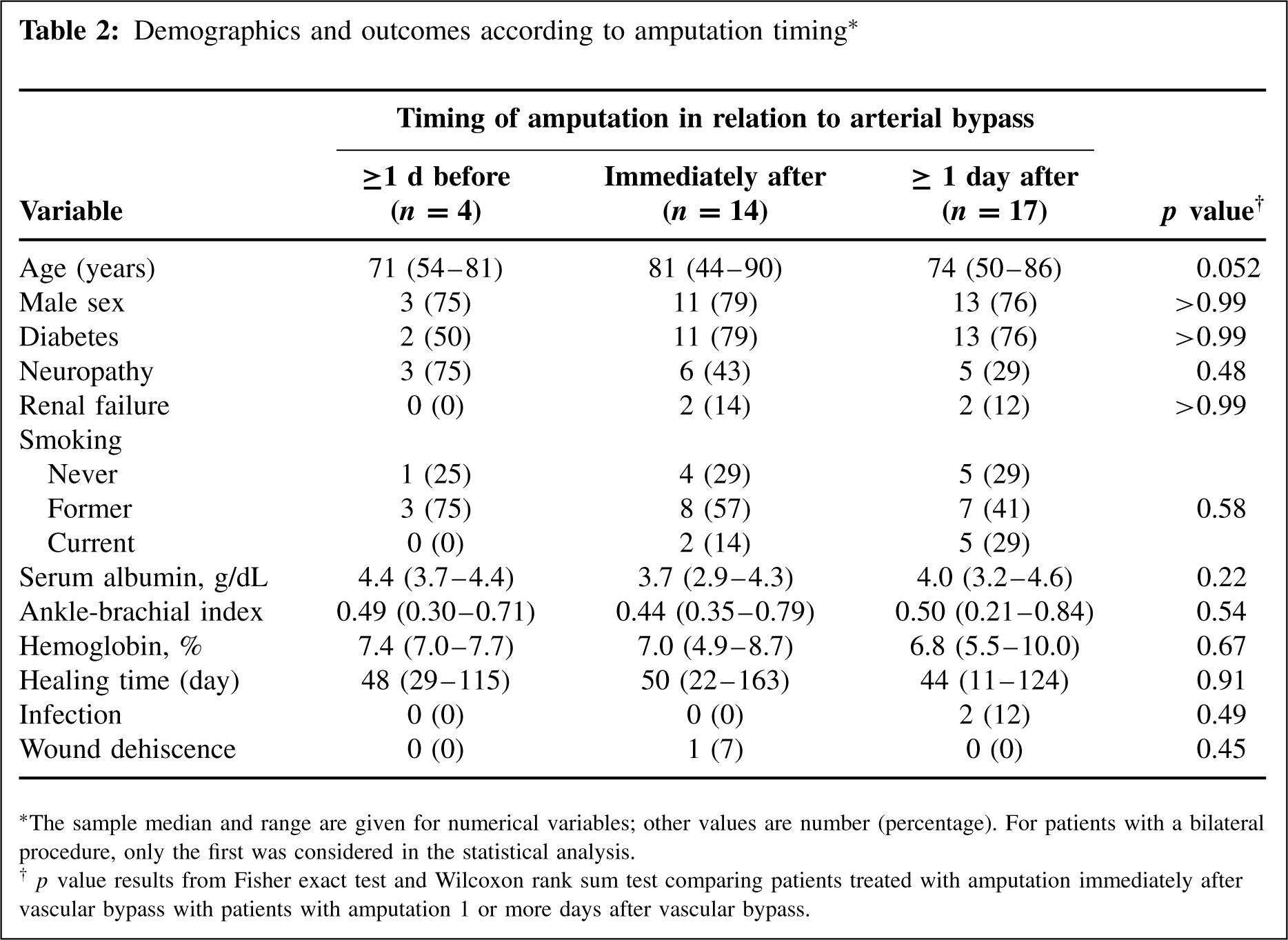
The sample median and range are given for numerical variables; other values are number (percentage). For patients with a bilateral procedure, only the first was considered in the statistical analysis.
p value results from Fisher exact test and Wilcoxon rank sum test comparing patients treated with amputation immediately after vascular bypass with patients with amputation 1 or more days after vascular bypass.
Median healing time in diabetic patients after amputation was 52 (range 11 to 163) days compared with 44 (range 25 to 88) days in nondiabetic patients (p = 0.36). The median diabetic patients’ glycosylated hemoglobin level at the time of surgery was 7.2%, with a range of 4.9% to 10.0% (reference range, 3.5% to 5.0%), indicating poor control of serum glucose levels. Both patients with bypass graft site infections and the patient with wound dehiscence were diabetic.
For all patients, the median serum albumin level was 3.9 g/dL, with a range of 2.9 to 4.6 g/dL (reference range 3.5 to 5.0 g/dL). There was no evidence of a correlation between albumin levels at the time of amputation and healing rate (p = 0.19). Median healing time was 71 (range 11 to 163) days in patients with a serum albumin level less than 3.9 g/dL compared with a median of 56 (range 11 to 163) days for patients with a serum albumin level of 3.9 g/dL or higher. The value of 3.9 g/dL was used as the threshold because, as the median albumin level, it statistically did not make a difference in outcome. However, lower albumin values used in other studies have been more predictive of healing rates.
The general surgery and nutrition literature uses a wound-healing threshold of 3.5 g/dL, 6 and Pinzur et al 16,17 used a threshold of 3.0 g/dL. 3 The serum albumin levels returned to normal values in all but two patients postoperatively.
Median healing time in active smokers after amputation was 36 days compared with 53 (range 24 to 124) days for patients who were former smokers and 34 (range 17 to 102) days for patients who never smoked (p = 0.34). Smoking cessation was required before revascularization; however, compliance data were not obtained. The patient with graft site wound dehiscence was a former smoker. The other two patients with graft site infection had never smoked.
Median healing time for the four patients with end-stage renal disease was 48 days, and these patients had no bypass site problems. This outcome was better than that reported previously 13,15 but was similar to the experience of Yeager et al. 23
Discussion
Healing rates of patients with gangrene or intractable skin ulcerations and severe peripheral vascular occlusive disease are improving as operative bypass techniques and preoperative testing evolve. It is important to evaluate what effects both the timing of amputation and the wound closure treatment of the amputation site have on the bypass graft site. Numerous studies have emphasized the requirement of a patent bypass graft for successful healing. This study included only patients with patent bypass grafts.
A large number of patients in this study were diabetic (26 of 35; 74%) and an equally large number were active or former smokers (25 of 35; 71%). Arterial occlusive disease and gangrene were found in patients who had quit smoking 20 to 30 years before their surgery. Apparently the risks of vascular occlusive disease remain well after quitting smoking. This is consistent with the findings of Suh et al. 18 showing greater nonunion rates in arthrodesis patients who smoked, regardless of when they stopped smoking.
The distribution of gangrene or ulceration of the toes was recorded. The great and second toes were most commonly involved (23 of 38; 61%). This may reflect the mechanical effects of shoe pressure, anatomic deformity, and neuropathy and does not follow any particular vascular supply patterns.
Albrektsen et al. 2 demonstrated that the increase in peripheral perfusion after revascularization was delayed and recommended a delay in definitive foot surgery for up to 1 week after bypass surgery. Unfortunately, gangrene with infection progression and unstable vital signs often require immediate action. No definite advantage in delaying the amputation was found in our study, albeit this study was limited by its retrospective nature as well as its limited sample size, resulting in lack of power to detect what may be real differences between groups.
Little has been written about criteria for primary wound closure versus delayed primary closure and closure by secondary intention in the context of forefoot or toe amputation. Primary closure rates varied from 100% to 46%. 19 With a patent vascular bypass graft, foot amputation wounds healed successfully in all patients in our study.
Although the number of vascular bypass site infections was small, patients with infections had in common primary wound closure of the amputation site. The three patients whose amputations were treated by delayed primary closure had no demonstrable wound healing delays or complications at the vascular bypass site.
Amputation site wound closure may adversely affect the bypass graft, but in this study no definite advantage in delaying the amputation was found.