
Abstract
Background
Ankle spanning external fixation has become the initial treatment of choice for complex tibial pilon fractures. Many fixator designs exist, but their biomechanical performance has not been studied extensively for this application. The goal of the present study was to compare the torsional performance of two commercially available frames, the Orthofix XCaliber and the Howmedica Hoffmann® II.
Methods
The XCaliber and the Hoffmann® II were each applied to six fresh cadaver lower extremities and were loaded in a materials testing machine. Strain gauges were attached to the anteromedial cortex of the distal tibia, and each specimen underwent torsional and axial load testing, with and without the external fixator. A simulated pilon fracture was created, and torsional testing was repeated.
Results
Results indicated that the XCaliber was significantly more rigid in internal rotation than the Hoffmann® II, before (49%) and after (41%) creation of the pilon fracture. Despite the XCaliber's increased rigidity relative to the Hoffmann® II (22% to 31%) in external rotation, statistical significance was not attained. Both fixators reduced strain (25% to 85%) at the anteromedial cortex upon torsional testing, but no significant differences between the two frames were noted.
Conclusions
The present study demonstrates that the XCaliber has mechanical advantages over the Hoffmann® II in terms of torsional rigidity for a tibial pilon fracture.
Clinical Relevance
Increased rigidity of the XCaliber could potentially lead to decreased time to union, and a lower incidence of pin loosening and would prove beneficial in a setting in which the external fixator is used as the definitive fixation.
Introduction
Tibial pilon fractures are fractures that involve a significant portion of the weightbearing surface of the distal tibia. Despite technologic advances in fracture fixation, these injuries continue to pose a challenge for even the most experienced traumatologist or foot and ankle specialist. Many of the difficulties in treating these fractures arise from the nature of the fracture itself, as well as the condition of the surrounding soft tissues.1,3 Both closed and open methods have been used in the treatment of complex pilon fractures, but the results have been less than satisfactory because of a myriad of complications, 11 which have included gross malreduction, superficial and deep wound infections, skin sloughing, and post-traumatic arthritis.1,3,11
Ankle spanning external fixation is reserved for tibial pilon fractures with marked comminution and significant soft-tissue injury.3,6,7,9 Other frame constructs, such as nonankle-spanning thin wire ring fixators, ankle spanning thin wire ring fixators, and hybrid ring fixators are occasionally used for tibial pilon fractures, but their use is limited to lower energy injuries with minimal to no comminution. Although the nonspanning frames allow more range of motion of the tibiotalar joint, which may promote healing of the articular surface, placement takes longer, and they do not aid in the reduction of a comminuted articular surface afforded by the ligamentotaxis of an ankle spanning external fixator. Ankle-spanning thin-wire frames also are limited by the amount of time that it takes to apply them and, in the acute setting, do not offer any advantages over other types of ankle spanning frames in terms of fracture reduction.
Numerous clinical studies have shown the benefits of applying a spanning external fixator in the treatment of complex pilon fractures,1,3,4,6 but we were unable to identify any biomechanical studies comparing the various configurations used to span the ankle in this complex injury pattern. Of course, there are numerous biomechanical studies dealing with external fixators in general, but these studies have tended to focus on the treatment of diaphyseal fractures. The treatments for diaphyseal fractures and intra-articular fractures with external fixators are very different, with the former relying on compression and the latter relying on a combination of distraction and ligamentotaxis. 8 Previous animal studies in which diaphyseal fractures have been treated with external fixators have shown that stiffer fixators lead to higher rates of bony union with a lower incidence of pin loosening,13,14 but if a frame becomes too stiff, bone healing may actually be impeded. 5 On the other hand, external fixation of intra-articular fractures relies on distraction. Therefore, when dealing with a comminuted intra-articular fracture, such as a complex pilon fracture, the ideal frame should be as rigid as possible because this will limit gross motion at the fracture site, provide a stable environment for soft-tissue healing, and decrease pin loosening.
Many fixator designs exist, but their biomechanical performance has not been studied for this application. There are two basic types of ankle spanning external fixators. The first type is the articulated uniplanar external fixator that uses one half-pin in the posterior tuberosity of the calcaneus, one half-pin in the talar neck, and two half-pins in the anteromedial face of the tibial diaphysis connected by an articulated carbon fiber column. The Orthofix XCaliber Articulated Ankle Fixator (Orthofix Corp., McKinney, TX) would fall into this general category. The second basic type, the triangulated calcaneal transfixing frame, uses two transfixation pins through the calcaneal tuberosity and two half-pins in the anteromedial face of the tibial shaft connected in a triangulating fashion through the use of carbon rods and pin-to-bar clamps. The Howmedica Hoffmann® II, Ankle Fusion Frame (Howmedica Corp., Geneva, Switzerland) would fall into this second category of fixators. The goal of the present study was to compare these two commercially available frames, hereafter referred to as XCaliber and Hoffmann® II respectively, in terms of torsional resistance and strain reduction at the fracture site.
Materials and Methods
Twelve fresh cadaver lower extremities were disarticulated at the knee (mean age, 65; range, 54 to 82 years). Ten of these consisted of five matched pairs and two unmatched came from donors of similar age, gender, and ethnicity. Differences in data recorded from these two specimens were comparable to those between matched pairs. All soft tissues were removed except for the interosseous membrane, tibiotalar joint capsule, and subtalar joint capsule. The specimens were divided into two groups with six designated for testing with the XCaliber frame, and six with the Hoffmann® II frame. Each external fixator was attached to the intact ankle following the manufacturer's recommendations in a manner that maintained neutral anatomic orientation. Both external fixators required two uniplanar pins (half-pins) placed into the anteromedial face of the tibial diaphysis. The XCaliber frame (Figure 1) used two uniplanar pins, one through the neck of the talus and one through the calcaneus, while the Hoffmann® II frame (Figure 2) used two transfixing pins through the calcaneus. After application of the fixator, the forefoot was removed at the level of the transverse tarsal joint. Specimens were secured in a tapered 2 × 3-in PVC pipe connector by two 1/8-in diameter pins and orthodontic resin, a form of polymethylmethacrylate (PMMA). Before pouring the PMMA, two 1/8-in diameter pins were inserted through the PVC into the calcaneus, one through the center of the calcaneus in an anterior to posterior direction and the other 5 mm superior to this pin in an anteromedial to posterolateral direction. Cutouts were made in the PVC, and modeling clay was strategically placed to prevent contact of PMMA with the external fixator pins.
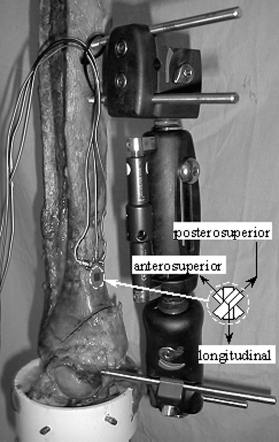
XCaliber frame on a typical specimen. The simulated fracture is clearly evident. Inset shows the orientation of the attached strain gauges on a right limb.
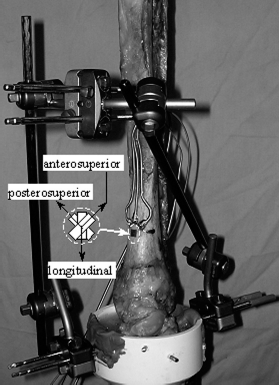
Hoffmann® II frame on a typical intact specimen. Inset shows the orientation of the attached strain gauges on a left limb.
The anteromedial surface of the tibia was prepared for strain gauge attachment using procedures established in the literature 10 with materials from Vishay Micro-Measurements (Raleigh, NC). Briefly, the periosteum was removed and the area sanded using 220-grit and then 320-grit silcon-carbide paper. A catalyst (Catalyst-C) was applied to the region, allowed to air-dry, and then cyanoacrylate (M-Bond 200) was applied. After drying, the surface was sanded again using 320-grit and then 400-grit silicon-carbide paper to smooth the dried glue. A rosette pattern strain gauge (WK-13-060WR-350) was then glued into place so that the center of the gauge pattern was 5.5 cm above the tibial plafond and centered in the anteromedial surface. This location was chosen to place the gauge approximately 2.5 cm superior to the fracture site. The center gauge aligned longitudinally with the tibial diaphysis, and the other two gauges were at 45 degrees to the center gauge, with one in an anterosuperior direction and the other in a posterosuperior direction (Figures 1 and 2). The integrity of each gauge was then confirmed using a Vishay Gauge Installation Tester (Model 1300). Hereafter, these gauges are referred to as the longitudinal, anterosuperior, and posterosuperior gauges.
Torsional and axial load testing was accomplished using a biaxial servo-hydraulic materials testing machine (Instron Model 1321, Instron Corporation, Canton, MA), retrofitted with an MTS TestStarII digital controller (MTS Corporation, Eden Prairie, MN). Data was acquired at a 100 Hz frequency while torsional rotation tests were performed for five cycles from 8 degrees internal to 8 degrees external tibial rotation. A 15-lb preload was maintained throughout torsional testing. Strain gauge signals were processed through Vishay Bridge Completion Modules (MR1-350-127).
After a specimen was mounted in the materials testing machine, the external fixation device was removed and torsional testing, as described above, was performed to obtain data for the intact specimen without fixation. The external fixation device was then reattached, while maintaining a 30-lb distractive force. The 15-lb compressive preload was reapplied, and torsional loading was repeated. Without removing the external fixator, an AO type B2 tibial pilon fracture was simulated by an osteotomy. To maintain uniformity of the osteotomy, the center of the plafond along the anterior edge of the articular surface was marked with an indelible marker, and a protractor was then used to create a line 45 degrees to the plafond beginning at the center-mark and exiting through the medial tibial cortex. At this point, an oscillating saw was used to make the osteotomy perpendicular to the anterior face of the distal tibia in an anterior-to-posterior fashion. The 15-lb preload was reapplied, and torsional loading was repeated. The specimen was then axially loaded for 100 cycles from 15 to 100 lb of compressive load. After axial loading, the 15-lb preload was reapplied, and torsional loading was repeated with the external fixator still attached to assess stability of the device. Finally, the external fixator was removed, the 15-lb preload reapplied and torsional loading repeated.
Data from the fifth cycle of torsion was analyzed using a mixed model ANOVA followed by Tukey-Kramer pair-wise comparison (SAS® for Windows v9.1, SAS Institute Inc., Cary, NC).
Results
Torsion Measurements
Typical torsional resistance of the tibia demonstrated substantial differences among the various states of fixation and fracture (Figure 3). When an external fixator was attached to a specimen, whether intact or fractured, the amount of torque required to achieve 8 degrees of tibial rotation increased significantly (more than three times) relative to the intact state without external fixation, for either internal or external rotation (p < 0.001) (Figure 4). Also, fractured specimens without external fixators required significantly less torque (at least 82%) to achieve 8 degrees of tibial rotation than did any of the states with external fixators (p < 0.001). Fractured specimens without external fixators appeared to require at least 42% less torsion at 8 degrees of tibial rotation than did intact specimens without external fixators, but significance was not shown (p > 0.5).
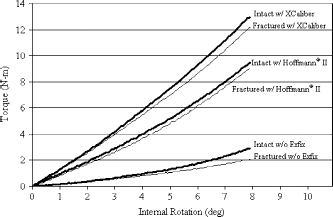
Typical torque versus rotation response of the tibia for the different states of fracture and fixation.
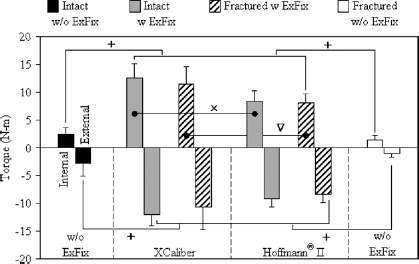
Torque achieved at 8 degrees of tibial rotation. Paired bars represent internal rotation (left) and external rotation (right). Statistically significant differences denoted by: + = p < 0.001, x = p < 0.01, ▿ = p < 0.05. Statistical comparisons among fixation states were made separately within internal and external rotation.
Intact specimens with the XCaliber required greater torsion than intact specimens with the Hoffmann® II, but this significance was only established for internal tibial rotation (49%, p < 0.01, internal; 31%, p > 0.4, external). After fracture, the XCaliber continued to require significantly greater torsion than Hoffmann® II for internal rotation (41%, p < 0.05) but not for external rotation (22%, p > 0.7). Finally, the torque achieved at 8 degrees of tibial rotation did not change (virtually the same magnitude and standard deviation) after axial cyclic loading for the XCaliber or Hoffmann® II fixators (p = 1.0).
Strain Measurements
The addition of external fixators generated tensile strains in unloaded intact specimens, which were statistically different from all other unloaded states as measured by longitudinal gauges (p < 0.001), with similar patterns in the anterosuperior and posterosuperior gauges (Table 1). The generation of tensile strains is reasonable given that a distractive force is induced across the joint to apply the fixator. Tensile strains in longitudinal gauges for unloaded intact specimens with the XCaliber external fixator appeared to be higher than with the Hoffmann® II, although statistical significance was not established (p > 0.07). After fracture, these tensile strains disappeared in unloaded specimens, with external fixators bringing strain measurements to levels comparable to unloaded unfixed fractured specimens.
Unloaded strain measurements relative to unloaded unfixed intact state
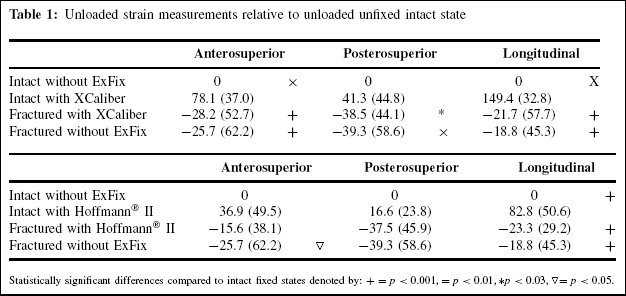
Statistically significant differences compared to intact fixed states denoted by: + = p < 0.001, = p < 0.01, *p < 0.03, ▿ = p < 0.05.
When loaded to 8 degrees of internal or external tibial rotation, strains relative to the start of each test were reduced compared to the intact unfixed state in the anterosuperior (50% to 85%) and posterosuperior (25% to 71%) gauges, but not all reductions were statistically significant (Figure 5). Longitudinal strain gauge measurements were reduced or reversed at 8 degrees of internal rotation, but were unchanged for 8 degrees external rotation.
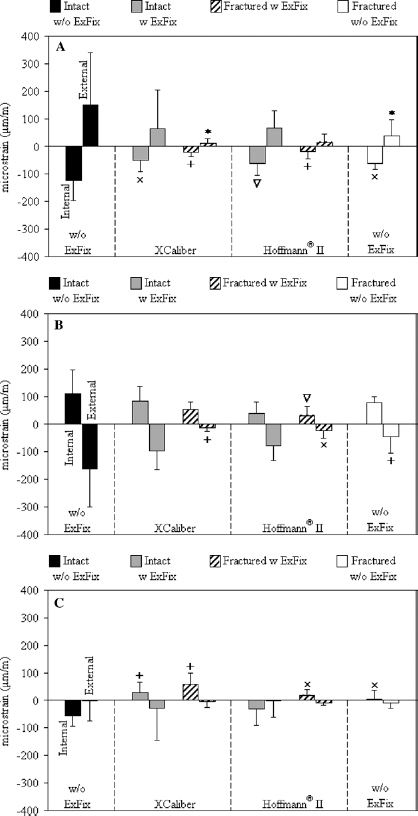
Strain achieved at 8 degrees of tibial rotation relative to the start of each test for:
Fractured strain states for both external fixators were comparable and were not statistically different for unloaded (p > 0.9) and loaded (p > 0.5) conditions. Additionally, strain states at 8 degrees of tibial rotation did not change (with virtually the same magnitude and standard deviation), after axial cyclic loading, for the XCaliber or Hoffmann® II fixators (p > 0.9). Similarly, fractured strain states for both external fixators were comparable to unfixed, fractured specimens in their unloaded state (p > 0.9) and at 8 degrees of external tibial rotation (p > 0.9).
At 8 degrees of internal tibial rotation, anterosuperior and posterosuperior strain measurements for both external fixators on fractured specimens were not statistically different from unfixed, fractured specimens (p > 0.2). Also, longitudinal strain measurements at 8 degrees of internal tibial rotation for fractured specimens with the Hoffmann® II fixator were not statistically different from unfixed, fractured specimens (p > 0.9). In contrast, longitudinal strain measurements for fractured specimens with the XCaliber appeared to be higher than unfixed fractured specimens at 8 degrees of internal rotation, but statistical significance was not established (p > 0.05). Calculation of principal strains and direction from the rosette data (Figure 6) demonstrated that these were very similar in magnitude to that measured by the strain gauges themselves with small values for the principal direction, particularly for external rotation. Thus, the directions of the perpendicular arms of the strain rosette (anterosuperior and posterosuperior) were close to the principal strain directions.
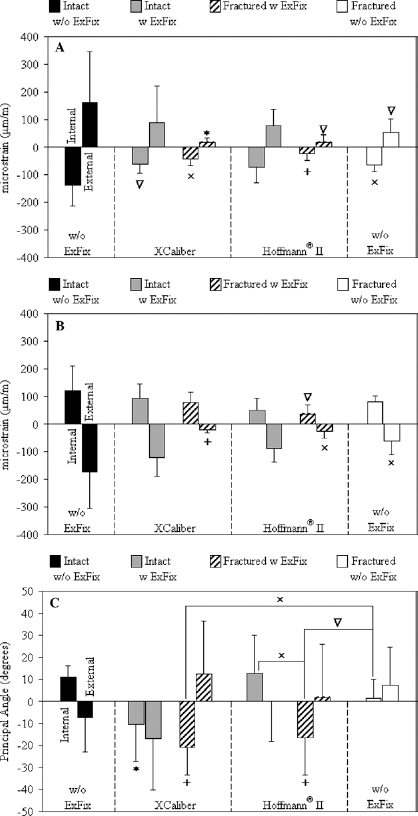
Principal strains and directions achieved at 8 degrees of tibial rotation relative to the start of each test for:
Discussion
Complex tibial pilon fractures continue to pose a clinical challenge. They usually are high-energy injuries sustained during motor vehicle collisions or falls from a height, and they often have a significant soft-tissue component.1,3,6,11 The therapeutic goals are maximization of function and minimization of soft-tissue complications. 11 Treatment modalities have included closed reduction and casting and immediate open reduction with internal fixation.1,3 Results at both extremes have been satisfactory for low-energy, simple injuries, but disappointing when used in the treatment of high-energy, complex tibial pilon fractures.1,3 Casting is limited by its inability to hold a stable reduction, 1 and open reduction and internal fixation affords an excellent reduction, but jeopardizes the soft-tissue envelope.1,3,4 On the other hand, external fixation, either alone or in combination with limited internal fixation, offers a superb alternative for these high-energy injuries.3,4,9 External fixation can be used as definitive fixation or as a temporizing measure before definitive open reduction and internal fixation. 9 In either scenario, the ideal fixator should be as rigid as possible to reduce gross motion at the fracture site and within the soft-tissue envelope and reduce the incidence of pin loosening and pin track infection.
No biomechanical studies to date have compared the articulated uniplanar external fixator and the triangulated calcaneal transfixing frame in the distraction mode commonly used for tibial pilon fractures. To date, the overwhelming majority of biomechanical studies dealing with external fixation and fracture healing have focused on the treatment of diaphyseal fractures. Most of these studies have examined the effects of frame stiffness on fracture healing. In a canine study, Wu et al. 14 treated tibial osteotomies using either a four half-pin unilateral external fixator or a more rigid six half-pin frame. Although all tibiae healed successfully, those treated with the more rigid six half-pin frame showed earlier clinical union and a lower incidence of pin loosening. Similarly, Williams et al. 13 compared a one-plane external fixator with a more rigid two-plane fixator. This study also used a canine tibial osteotomy model and was able to demonstrate that, at 13 weeks, the healed osteotomy sites in those tibiae treated with the more rigid frame exhibited greater torsional stiffness. In contrast, Goodship et al. 5 found a reduction in the healing rate of sheep tibiae when a stiffer frame was employed, a finding that they attributed to the decreased mechanical stimulus at the osteotomy site treated with the stiffer fixator. However, tibial pilon fractures rely on distraction and ligamentotaxis and not on compression or gap healing of an osteotomy site for alignment.
Other authors have examined the use of external fixation for ankle arthrodesis. Thordarson et al. 12 tested three configurations of the Calandruccio clamp and an Orthofix unilateral external fixator using fresh-frozen cadaver specimens. In that study, the frames were placed across an arthrodesis site which was subsequently subjected to an internal-external tibial torsion, as well as a plantarflexion-dorsiflexion bending moment. The Orthofix fixator showed the least amount of motion in terms of plantarflexion and dorsiflexion, and there were no differences in tibial torque between any of the four constructs. In a combined biomechanical and clinical study, Berman et al. 2 modified the classic Charnley frame by adding a transfixation pin through the first metatarsal, thus increasing its torsional and anterior-posterior bending stiffness. This modified Charnley frame was then used in 23 ankle fusions. The 91.3% fusion rate at an average of 11 weeks after arthrodesis was attributed to decreased micromotion at the site secondary to increased rigidity.
Despite studies that have examined external fixation in the treatment of diaphyseal fractures or in ankle arthrodeses, there remains a paucity of biomechanical data to support the use of one spanning ankle external fixator over another. Our goal was to compare two commercially available frames in terms of their ability to resist torsional loading and to reduce strain or force transmission to permit healing near the fracture site on the anteromedial cortex of the distal tibia. In the present study, we compared the Orthofix X-Caliber Articulated Ankle Fixator with the Howmedica Hoffmann® II Ankle Fusion Frame in terms of torsional resistance and strain reduction. Our results indicate that the Orthofix frame was significantly more rigid in internal rotation than the Hoffmann® II frame both before and after creation of the fracture. Although the Orthofix frame also was more rigid in external rotation, this did not reach a level of significance. The increased rigidity of the Orthofix frame noted during torsional testing appears to be due to two main factors. First, the Orthofix pins are larger in diameter: 5.5-mm compared to the 5-mm half-pins and 4-mm transfixation pins of the Hoffmann® II frame. The carbon fiber column of the Orthofix frame also is much larger in cross-sectional area (~ 38 mm in diameter =~ 1100 mm 2 ) than the combined values of the Hoffmann® II dual carbon rods (8 mm in diameter each = 100 mm 2 total). Second, the configuration of the Orthofix frame with pins in both the talus and calcaneus may provide more stability across both the tibiotalar and subtalar joints. Additionally, the Hoffmann® II construct requires a larger number of clamps for fixation than the Orthofix frame in which the clamps are part of the carbon fiber column. Clinically, this could provide more potential sites of subtle loosening or slippage, which would compromise stability of the fixation.
In terms of strain, fractured specimens with either fixator experienced strains in their unloaded state which were comparable to unfixed fractured specimens. An external fixator on the intact specimen resulted in positive strains as the joint was distracted to apply the fixator, which was resisted by soft tissues in the intact state, and thus strains resulted even for the unloaded (i.e. not under torsion) state. The finding of similar strains between fixed-fractured and unfixed-fractured states in the unloaded specimen means that the fracture eliminates the tension induced by the joint distraction. While not all changes were significant, both fixators tended to reduce added strain experienced at the anteromedial metadiaphyseal cortex when subjected to 8 degrees of tibial rotation. It should be pointed out that both the torsional and strain gauge results were maintained after the axial cyclic loading sequence, a finding that indicates that both frames were able to maintain their overall rigidity even after repeated axial loading.
In summary, the results of the present study demonstrate that the Orthofix XCaliber fixation frame, an articulated uniplanar-type external fixator, has mechanical advantages over the Hoffmann® II fixation frame, a triangulated calcaneal transfixation-type external fixator, in terms of torsional rigidity, for a tibial pilon fracture. This increased rigidity could potentially lead to a decreased time to union and a lower incidence of pin loosening. Furthermore, a stiffer construct would prove beneficial in a setting in which the external fixator is used as the definitive fracture fixation.