
Abstract
Background: Traditionally, pediatric patients with symptomatic calcaneonavicular coalitions have been treated with resection of the coalition and interposition of the origin of the extensor digitorum brevis muscle. Despite the success of calcaneonavicular coalition resection in children, many surgeons are reluctant to perform this procedure in adults or in patients with osseous coalitions, and joint sacrificing arthrodesis often is done instead. Methods: Seven adult patients (eight feet) had calcaneonavicular coalition resection with extensor digitorum brevis interposition. The average patient age was 41 years, and all patients displayed isolated, symptomatic calcaneonavicular coalitions without any radiographic evidence of degenerative arthritis. At followup, physical and radiographic evaluations were performed, and an American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot score was recorded. Charts were reviewed for complications and patients were questioned with regards to their overall satisfaction with the surgery. Results: At a mean postoperative followup of 56.5 months, the average AOFAS score was 87. Review of most recent radiographs revealed no degenerative changes or recurrence of the coalition. All patients responded that they would have this surgery again and that they would recommend this procedure to a friend. Complications included one superficial infection and one dysesthesia involving the sural nerve. Conclusions: The results of the present study suggest that resection combined with muscular interposition can be successful in patients over the age of 18 in whom conservative management of their symptomatic coalitions has failed. This procedure offers an excellent alternative to arthrodesis and has a very low complication rate.
Keywords
Introduction
A tarsal coalition represents an abnormal fusion between two adjacent tarsal bones, most likely secondary to a failure of segmentation of the primitive mesenchyme. 3,6,7,15,22 It is estimated that less than 1% to 2% of the general population is affected by this condition, 2,3,6,7,9,13,22 and there does not appear to be a gender 3 or racial 7,13 predisposition. However, an autosomal dominant trait has been suggested. 4,22 Approximately 90% of these coalitions affect either the subtalar joint or the intervening space between the calcaneus and the navicular, with these two areas being affected in roughly equal numbers. 2,7 Although tarsal coalition may be asymptomatic, symptoms typically include hindfoot or midfoot pain, 4 -8 recurrent ankle sprains, 6,18,19 difficulty ambulating on uneven surfaces, 18 and significant disability associated with decreased or absent subtalar motion. 4 -6 Most patients present in childhood or adolescence, at an age that appears to coincide with the ossification of the coalition. 4,7,11,13,21 However, there remains a population of patients who, for reasons that are not clearly understood, become symptomatic in adulthood.
Traditionally, pediatric patients with calcaneonavicular coalition are treated with resection of the coalition and interposition of the origin of the extensor digitorum brevis muscle. 19,22 This procedure has had favorable outcomes in terms of symptomatic relief and a low rate of complications 2,4,8,10,15 -17,20 and has become a standard treatment in young patients with a calcaneonavicular coalition in whom conservative treatment has failed. 19 Contraindications to this procedure have included osseous coalitions, 4,5,11 coalitions in adult patients, 11,13 and radiographic evidence of degenerative arthritic changes elsewhere in the foot. 4 -6 Some authors have suggested that patients meeting any of these criteria should not be considered a candidate for resection and should, therefore, be offered an arthrodesis. 2,6,13 However, in an older patient without significant degenerative changes, an arthrodesis is irreversible and may predispose the patient to arthritis elsewhere in the foot.
Despite the success of calcaneonavicular coalition resection in the pediatric population, many surgeons are reluctant to perform this procedure in adult patients or in patients with an osseous coalition. It is their belief that given the chronicity of these coalitions, these patients may have arthritic changes not yet evident radiographically. 11 There have been few reports in the literature of calcaneonavicular coalition resection in adults, and more specifically, calcaneonavicular coalition resection with extensor digitorum brevis interposition in adult patients. The purpose of our study was to evaluate the objective and subjective results of calcaneonavicular coalition resection with extensor digitorum brevis interposition in a population of patients over the age of 18 years.
Materials and Methods
Patient Demographics
Between June, 1998, and February, 2002, seven adult patients (eight feet) had calcaneonavicular coalition resection with extensor digitorum brevis interposition. The five women and two men had an average age at the time of surgery of 41 (range 31 to 61) years. All patients were diagnosed with an isolated calcaneonavicular coalition, displayed symptoms attributable to this coalition, and had failed to obtain relief of symptoms after a conservative treatment regimen that included anti-inflammatory medications, orthoses, and casting. Inclusion criteria were age older than 18 years, an isolated calcaneonavicular coalition, and excision of this coalition with interposition of the extensor digitorum brevis origin into the defect. Patients were excluded if they had had a previous operative procedure on the affected foot.
Preoperative Evaluation
Preoperatively, a focused history was obtained from each patient. This was followed by a thorough clinical examination of the patient's bilateral foot and bilateral ankle with specific attention paid to subtalar range of motion. Additionally, all plain radiographs were evaluated for evidence of a calcaneonavicular coalition, a concomitant second tarsal coalition, associated pathology, degenerative changes, and talar beaking, and all coalitions were classified as complete-ossified or incomplete-fibrous based on radiographic appearance (Figure 1). CT scans were obtained on seven feet, and a MRI was obtained on one foot to confirm the diagnosis and to rule out concomitant coalitions. Total preoperative subtalar range of motion (sum of inversion and eversion) was less than 5 degrees in all eight feet. There was no evidence of degenerative changes or talar beaking on preoperative radiographs, CT, or MRI. One ankle displayed an anterior drawer on physical examination before surgery. Review of preoperative records revealed no history of gastroc contracture, abnormal transverse tarsal motion, significant forefoot varus, or hindfoot valgus in any patient.

Preoperative radiograph of 31-year-old man with isolated calcaneonavicular coalition.
Operative Procedure
All surgeries were performed by the senior author (H.R.T). Thirty to 60 minutes before surgery, all patients were administered an appropriate intravenous antibiotic. An Ollier incision was centered over the calcaneonavicular coalition from the most lateral extent of the extensor digitorum longus tendons dorsally to the peroneal tendons plantarly. The sural cutaneous nerve and the dorsal intermediate branch of the superficial peroneal nerve were identified and protected. The origin of the extensor digitorum brevis was identified as well as its dorsal and plantar margins. Using electrocautery and a Cobb elevator, the origin and muscle belly of the extensor digitorum brevis were elevated while protecting the overlying fascia. The origin was retracted distally and grasped with an interlocking suture. The borders of the coalition were identified and with a straight osteotome, a 1 cm rectangular block including the entire coalition was removed. Parallel cuts were made to prevent a convergent, trapezoidal resection. After removal of the coalition, the depths of the resection site were debrided with a rongeur. A free Keith needle was then attached to the limbs of the suture and passed medially through the resection. The tips of the needles exited the soft tissue of the medial arch just dorsal to the weightbearing surface and were subsequently secured over a soft dental bolster (no button was used). This brought the muscle into the depths of the resection. Radiographs were taken to confirm adequate resection, and the wound was closed in layers. A short-leg fiberglass, walking cast was applied. Patients were allowed to bear weight as tolerated the day after surgery. The cast, wound sutures, and bolster stitch were removed at 3 weeks, and all patients were sent to physical therapy for ankle and hindfoot range-of-motion exercises.
Postoperative Evaluation
Average postoperative followup was 56.5 (range 39 to 84.5) months. Each patient was administered a standardized set of subjective questions from the American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Scale. 12 This set included questions regarding current pain levels, postoperative improvement in terms of pain, activity limitations, maximal walking distance, and difficulty with uneven surfaces. In addition to this standard set of questions, patients also were asked about pre- and postoperative orthoses, subsequent foot operations, wound dehiscence, superficial and deep wound infections, and nerve damage. Complications and subsequent treatment of these complications were reviewed in the medical records as well. Finally, patients were asked if they would have this surgery again, and if they would recommend this surgery to a friend given their experience.
After answering all questions adequately, the physical examination portion of the AOFAS Ankle-Hindfoot Scale was performed. This included an examination of the patient's gait, sagittal ankle motion (combined dorsiflexion and plantarflexion), coronal hindfoot motion (combined inversion and eversion), ankle and hindfoot stability, and overall alignment. All postoperative range-of-motion measurements were obtained with the use of a goniometer. Based on the patient's answers to the subjective questioning and the results of the physical examination, an AOFAS score was assigned for each patient.
Finally, plain radiographs were obtained and evaluated for evidence of degenerative changes anywhere in the foot and for recurrence of the calcaneonavicular coalition (Figure 2).
Results
Intraoperatively, three coalitions were found to be complete osseous fusions, and five were fibrous (incomplete). These findings are in concordance with their appearance on preoperative plain radiographs.
Postoperatively, two patients reported that they were pain-free, while five patients complained of only mild pain (including both feet in the patient who had bilateral resections). However, all seven patients reported an improvement in terms of pain from preoperative levels. Two patients complained of recreational activity limitations, whereas the remainder denied any activity limitations. All seven patients were able to walk more than six city blocks, and five patients reported no difficulties ambulating on any surface. Two individuals reported some difficulty on uneven terrain, stairs, inclines, or ladders.

Postoperative radiograph of same patient 84.5 months after resection of the coalition. No recurrence of coalition was noted, and no evidence of degenerative changes was present.
Preoperatively, one patient was wearing orthoses. This number increased to two postoperatively (including the original). At final followup, none of the patients had undergone a subsequent operation on the involved foot.
At the postoperative physical examination, no gait abnormalities were noted. Average ankle dorsiflexion was 16 (range 10 to 20) degrees and average plantarflexion was 41 (range 30 to 50) degrees. Average hindfoot inversion was 4 (range 0 to 5) degrees and average hindfoot eversion was also 4 (range 0 to 5) degrees, giving an average total subtalar range of motion of 8 degrees, a slight improvement from preoperative levels. However, a level of significance could not be calculated for these measurements given the fact that all preoperative subtalar ranges of motion were recorded as either 0 degrees or less than 5 degrees. All ankles were stable to anterior-posterior stress and varus-valgus stress. All eight feet were plantigrade with well-aligned hindfeet and ankles. The average AOFAS Score was 87 (range 79 to 97). Review of the most recent radiographs revealed no degenerative changes or recurrence of the calcaneonavicular coalition.
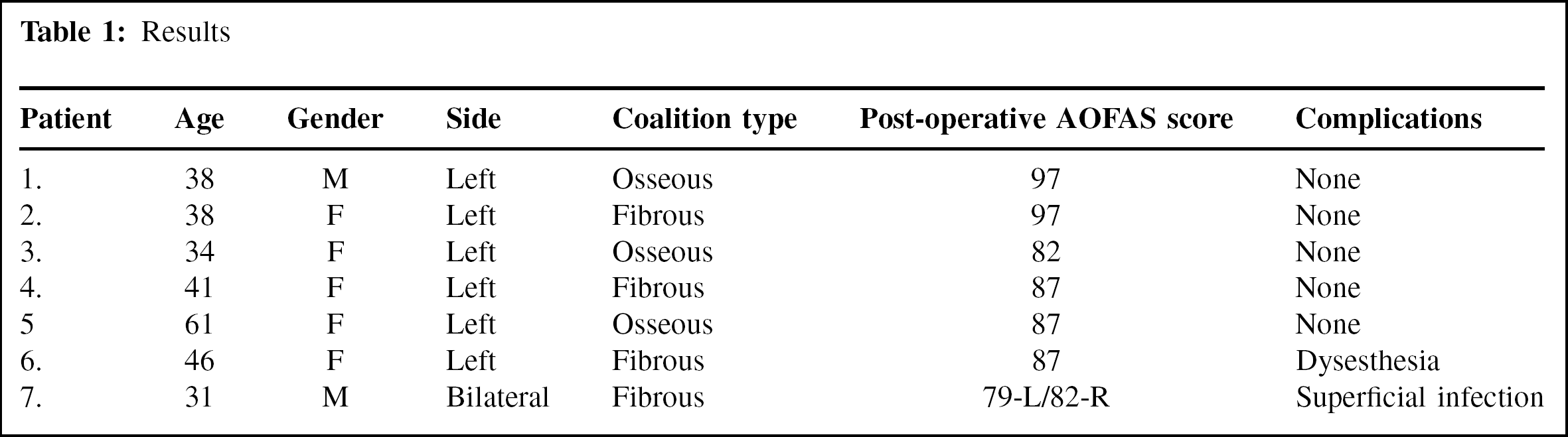
Complications were few. There were no deep infections and only one superficial wound infection with mild dehiscence. This wound was treated with oral antibiotics, whirlpool, and local wound care, and healed by secondary intention. One dysesthesia involving the sural nerve resolved at 6 weeks (Table 1). All seven patients responded that they would have this surgery again and would recommend this procedure.
Discussion
Most calcaneonavicular coalitions are diagnosed and treated in children and adolescents. Initial treatment usually consists of nonoperative measures such as anti-inflammatory medications, orthoses, casting, and occasionally localized steroid injections. Although a small percentage of patients respond to nonoperative management, most remain symptomatic and require operative intervention. 10,15,17 Bagdley, 1 in 1927, was the first surgeon to describe the resection of a bony bridge between the calcaneus and the navicular in a 13-year-old patient with a painful, peroneal spastic flatfoot. Since 1927, this procedure has undergone a number of modifications, the most significant of which was the interposition of the origin of the extensor digitorum brevis muscle into the defect created by the resection.
Given its success, calcaneonavicular coalition resection with extensor digitorum brevis interposition has become the standard operative procedure in pediatric patients whose radiographs reveal no advanced degenerative changes elsewhere in the foot. 19,22 Its success in the pediatric population has been well documented. Gonzalez and Kumar 10 reported the results of calcaneonavicular coalition resection and interposition of the extensor digitorum brevis in 75 feet (48 patients) with 77% good to excellent results. The best outcomes were in patients under the age of 16 with cartilaginous coalitions. Of the patients followed for more than 10 years, the results did not deteriorate with time. Similarly, Swiontkowski et al. 20 reported the results of 39 calcaneonavicular coalition resections, 38 of which included interpositional material (extensor digitorum brevis or fat). At a mean followup of 4.6 years, there were 29 asymptomatic feet, six feet with a mild ache during strenuous activity, and four feet with moderate to severe pain. The average patient age was 12 years. Other authors have reported comparable success rates in the pediatric population. Moyes et al. 16 reported 10 patients (average age 12 years) who had resection with extensor digitorum brevis interposition. At a mean followup of 3.4 years, nine were symptom-free. The one patient who was not pain-free had developed secondary degenerative changes. Following resection with interposition, 23 of 26 patients treated by Jayakumar and Cowell 11 were symptom-free. They stated that these patients were able to ambulate without any difficulty and were able to participate in sports. The three failures had occurred in two patients who displayed degenerative changes elsewhere in the foot prior to surgery and in one patient who had an unrecognized concomitant talocalcaneal coalition. O'Neill and Micheli, 17 in a retrospective review, evaluated 15 feet in adolescent athletes with osseous calcaneonavicular coalitions. Fourteen had good or excellent ratings on an objective foot and ankle scale at an average follow-up of 5.1 years. Similarly, Morgan and Crawford 15 also looked at adolescent athletes with symptomatic tarsal coalitions. Of the six patients (nine feet) there was only one unsatisfactory result which was attributed to an inadequate resection of the coalition.
Results
In contrast to the numerous studies that have described calcaneonavicular coalition resections in pediatric patients, there have been few studies that have examined the results of this procedure in adults. It has been recommended that adult patients with symptomatic calcaneonavicular coalitions should be treated with a triple arthrodesis 14 and that resection should be confined to patients under the age of 14 years. 13 However, others have suggested that there is no upper age limit and that resection is warranted if there is no radiographic evidence of advanced degenerative changes. 22 Another topic of concern is the complete osseous coalition. With advancing age, coalitions tend to ossify, meaning that an adult patient would be more likely to present with an osseous coalition. Jayakumar and Cowell 11 suggested that an osseous coalition was a relative contra-indication to resection because it was likely that progressive degenerative changes paralleled the ossification process. On the other hand, Davis 6 stated that an initial attempt at resection should be made whether the coalition is fibrous, cartilaginous, or osseous. However, he did note that adult patients tend to have more favorable results when the coalition is not ossified.
Cohen et al. 2 evaluated the results of calcaneonavicular coalition resection in 12 adult patients (13 feet). The average patient age was 33 years and the average followup was 36 months. Preoperatively, 75% of the patients displayed radiographic evidence of degenerative changes. Of these 13 resections, six had interposition of the extensor digitorum brevis and seven had bone wax with gelfoam. Ten patients reported subjective relief of their symptoms and the average improvement in subtalar motion was 10 degrees. In the two patients with unsuccessful outcomes, progressive degenerative changes were noted at follow-up and both patients eventually required a hindfoot arthrodesis.
Varner and Michelson 21 retrospectively reviewed 32 feet in 27 adult patients with tarsal coalitions, including 18 subtalar coalitions, 14 calcaneonavicular coalitions, and one naviculocuneiform coalition. One patient had both a subtalar and a calcaneonavicular coalition in the same foot. The average patient age was 40 (range 16 to 81) years. Eleven coalitions were asymptomatic and 14 feet were successfully treated nonoperatively. Of the seven symptomatic feet in which conservative treatment had failed, one had calcaneonavicular resection, four had subtalar arthrodesis, and two were scheduled for subtalar arthrodesis at the time of publication. All five of the operatively treated feet were pain-free at the most recent follow-up. No mention was made as to whether or not the extensor digitorum brevis was interposed or whether any of the four subtalar fusions were done in patients with calcaneonavicular coalitions.
In the podiatric literature, Fuson and Barrett 8 reported their experience with resectional arthroplasty for the treatment of calcaneonavicular coalitions in 24 adults. Results were rated as good in 21 feet, fair in one, and poor in two. An explanation of their rating system was not offered, and the length of followup was not given.
Considerable controversy exists regarding the interposition of the extensor digitorum brevis after resection of the calcaneonavicular coalition. Advocates of muscular interposition cite lower recurrence rates when the newly created void is filled. At a mean followup of 3.4 years, Moyes et al. 16 found no recurrences of the coalition on oblique radiographs in 10 patients who had resection with extensor digitorum brevis interposition. In contrast, three of the seven patients who had resection without interposition displayed radiographic evidence of calcaneonavicular bar recurrence. This difference was shown to be statistically significant. Swiontkowski et al. 20 used interpositional material (fat or muscle) in 38 of 39 feet without a single radiographic recurrence. Gonzalez and Kumar 10 examined the results of calcaneonavicular coalition resections with interposition of the extensor digitorum brevis in 75 adolescents with followup ranging from 2 to 22 years. They noted partial reformation in 22% of patients with no complete coalition reformations. Similarly, Cowell 4 reported no total reformations in 26 feet undergoing resection with muscular interposition at 5-year followup. Lending further support to interposition of the extensor digitorum brevis origin is a study by Mitchell and Gibson, 14 which examined the results of simple excision of 41 calcaneonavicular coalitions without the insertion of muscle or fat into the intervening space. At a mean followup of 6 years, there was a recurrence of the coalition “to a large extent” in one-third and “to a slight extent” in an additional one-third of feet.
Those surgeons who do not favor the interposition of the extensor digitorum brevis in conjunction with a calcaneonavicular coalition resection believe that the complication rate may be increased by the interposition. In the series of Cohen et al., 2 an extensor digitorum brevis interposition was performed in the first six feet. Three of these feet developed a lateral wound dehiscence, so the interposition was subsequently abandoned. In the last seven feet, bone wax was applied to the osteotomized bone surface, the void was filled with gelfoam, and the extensor digitorum brevis was reattached to its origin. There were no new wound dehiscences noted, leading the authors to surmise that these dehiscences may be caused by the creation of a dead space deep to the lateral wound. Fuson and Barrett 8 interposed the extensor digitorum brevis in one of their 24 resections. This patient developed pain in the sinus tarsi and was subsequently taken back to the operating room where the extensor digitorum brevis was re-attached to its origin. She later developed reflex sympathetic dystrophy. These authors suggested that the extensor digitorum brevis may function as an “extensor capsularis” and that its interposition may lead to a painful pinching of the subtalar joint capsule during dorsiflexion of the ankle. Ehrlich and Elmer 7 recommended against the interposition of the extensor digitorum brevis origin, because most surgeons are overly cautious about protecting the medial pull-out suture. They believed that this necessitated a period of cast immobilization at the expense of range of motion.
The results of our study lead us to believe that resection of a calcaneonavicular coalition in combination with extensor digitorum brevis interposition can be a successful procedure in adult patients who have not developed degenerative arthritis in the hindfoot or midfoot. This procedure is associated with a low rate of complications and may delay or prevent a future arthrodesis without hindering the ability to perform such a fusion. Our study is limited by low patient numbers and a mean followup of only 56.5 months. The relative scarcity of adult patients with symptomatic tarsal coalitions requiring operative intervention makes amassing a large number of patients or constructing a randomized, prospective trial very difficult. However, we believe that a larger series conducted in a randomized, prospective manner is indicated. Finally, our study is limited by its lack of a preoperative AOFAS score. Although a postoperative score allows some comparison between studies, a preoperative score would have allowed us to evaluate outcomes using a validated rating system.