
Abstract
Background: Osteolysis after total ankle arthroplasty (TAA) has become a major concern regarding long-term implant survival. The primary goal of this study was to determine whether CT was more sensitive than plain films in detecting the presence and extent of periprosthetic lucency. A secondary goal was to determine whether lack of syndesmotic fusion was associated with more extensive lucency. Methods: Seventeen patients (19 ankles) who had TAA between 2001 and 2003 were consecutively recruited and evaluated as part of a prospective study. Plain radiographs and helical CT with metal-artifact minimization were obtained. Evidence of lucent lesions and syndesmotic fusion was compared using the different imaging techniques. Results: Of the 19 ankles imaged, a total of 29 lesions were detected by CT, whereas plain radiographs detected 18 lesions. CT detected 21 lesions less than 200mm 2 , of which plain radiographs detected only 11. The mean size of the lesions detected on CT was over three times larger than the size on plain radiographs. With the small sample size used, there were no statistically significant differences between ankles with and without fusion of the syndesmosis and the extent (p = 0.84) and location (p = 0.377) of lucency. Conclusion: CT is a more accurate method for early detection and quantification of periprosthetic lucency than plain radiographs. Accurate evaluation of lucent lesions may identify patients at high risk for lack of syndesmotic fusion with subsequent loosening and implant failure.
Introduction
Disabling tibiotalar arthritis is most often a sequela of trauma, rheumatoid arthritis, or degenerative disease. Ankle arthrodesis has been the standard operative procedure for pain relief in patients with advanced tibiotalar arthritis refractory to all other treatment modalities such as analgesics, physical therapy, or brace management. Although arthrodesis has been successfully performed to alleviate pain and restore stability, this treatment continues to be associated with a high complication rate and functional impairment. 1,8,14,16,21 Postoperatively, patients may experience a considerable alteration in their gait with respect to a shortened stride length and decreased cadence. In addition, compensatory motion at adjacent joints may result in increased degenerative wear to these joint surfaces. 8 Total ankle arthroplasty (TAA) was developed as an alternative to arthrodesis for end-stage arthritis.
New TAA implant designs are continually being developed to improve stress distribution while allowing satisfactory ankle stability and range of motion. The implant used in this study, the Agility Ankle prosthesis (DePuy, Warsaw, IN), is the only ankle of the current generation of device systems that is fully approved by the FDA. A tibiofibular syndesmotic arthrodesis is incorporated which provides increased surface area for bone ingrowth as well as improved weight distribution of the prosthesis through load sharing with the fibula. Despite improvements in design, complications continue to threaten the success of these implants.
A number of relevant findings have emerged from studies of total hip implants, and evidence that acetabular component loosening is a manifestation of periprosthetic osteolysis has been reported. 9 In addition, studies on total hip arthroplasty have reported an inverse relationship between the extent of pelvic osteolysis and the success of revision surgery. 6 It also has been found that patients often remain asymptomatic despite massive osteolysis. 11 For these reasons, the significance of periprosthetic lucency has become a leading issue in long-term implant survival.
Traditionally, plain radiographs have been used to assess the extent of periprosthetic lucency after TAA. However, the detection of lucent lesions on radiographs is limited, and more sensitive methods may allow both earlier detection and improved quantification of lucent lesions. The significance of improved characterization is the potential for earlier intervention with both medical and economic benefits.
To our knowledge, there has been no study examining the efficacy of helical CT in identifying lucency after TAA. Thus, the purpose of our study was to determine whether CT was more sensitive than plain radiographs in detecting the presence and extent of periprosthetic lucency. As an exploratory aim, we examined whether lack of fusion (either partial or nonunion) of the syndesmosis was associated with more extensive lesions, and, specifically, lesions in the lateral ankle.
Materials and Methods
Patients
A total of 17 patients (19 ankles) who had TAA during the years 2001 through 2003 were consecutively recruited for this study. Patients were recruited for the purpose of this cross-sectional study in observance with current HIPAA requirements. The institutional review board of Evanston Northwestern Healthcare approved this study, and all patients provided informed consent. The cohort consisted of 10 men and seven women with a mean age of 68 (range 44 to 83) years. The indications for arthroplasty were severe pain in the ankle unrelieved by joint conservative treatment, and degenerative joint changes on plain radiographs. The preoperative diagnosis included post-traumatic osteoarthritis (14 ankles), primary osteoarthritis (four ankles), and rheumatoid arthritis (one ankle). Each patient had one set of images (radiographs and CT) at a single visit after enrolling in the study. The mean time-interval between surgery and imaging was 23 (range 7 to 38) months.
Implant
The Agility Ankle® prosthesis (DePuy, Warsaw, Indiana) is a two-component semiconstrained implant allowing for axial rotation and medial and lateral translation of the talar component. The device consists of a titanium tibial component, a cobalt-chromium talar component, and a polyethylene spacer secured within the tibial component. Both the tibial and talar components are porous coated for cementless press-fit fixation by means of bone ingrowth. Unique to this implant is the incorporation of an arthrodesis of the tibiofibular syndesmosis. This feature provides increased surface area for bone ingrowth as well as increased load distribution to the fibula.
For the Agility Ankle, additional postoperative intervention currently is based on radiographic assessment of the syndesmosis along with clinical assessment of pain. A solid fusion mass between the distal tibia and fibula should be radiographically evident 6 months postoperatively. Patients with persistent pain and swelling and inadequate radiographic evidence of union by this time may require revision arthrodesis of the syndesmosis and possibly component revision. Initially, a period of immobilization in a cast or weight-bearing boot is attempted to allow the fusion to mature.
Radiography
Weightbearing radiographs consisted of anteroposterior, lateral, and mortise views. Lesions were defined as well demarcated lucencies larger than 2 mm at the interface between the tibial component and the tibia or fibula. The size of each lesion was determined on the PACS system (GE Healthcare, Barrington, IL) with electronic calipers calibrated in centimeters by measuring the longest diameter and longest width perpendicular to that diameter. The term diameter was used as opposed to length because most lesions are circular. The areas of the lesions were obtained by multiplying these two measurements. Four locations of tibial lesions were classified as anterior, posterior, medial, and lateral. A fifth location was defined at the level of the fibula. The tibiofibular syndesmosis was classified as fused, partially fused, or not united. The films were sequentially reviewed by the senior musculoskeletal radiologist (M.L.).
Helical Computed Tomography
The CT images were made with a GE LightSpeed (General Electric, Milwaukee, Wisconsin) helical scanner. A metal-artifact minimizing protocol was used, consisting of scanning at 140 keV, no image enhancement, a pitch of ± 1.0, as small a field of view as possible, a bone algorithm, and overlapping of images by > 50%. 17 The helical CT scan began from 5 cm proximal to the tibial component to a point distal to the end of the implant. Patients were scanned in the axial plane, and coronal and sagittal images were reformatted from the axial images. The thickness of these sections was 1.25 mm.
Lesions were defined as well-demarcated lucencies between the tibial component and bone without osseous trabeculae. As with the radiographs, the longest diameter of each lesion and the longest width perpendicular to that diameter were measured on the coronal images using the PACS system electronic calipers. The areas of the lesions were obtained by multiplying these two measurements. Location categories for radiographs were applied, with the addition of a central tibial location. The tibiofibular syndesmosis was classified as fused, partially fused, or not united. CT scans were mixed and reviewed randomly at a different time than radiographs by the senior musculoskeletal radiologist who was blinded to prior results (M.L.).
Statistical Analysis
To assess agreement in detecting nonfusion between the two methods (radiograph, CT), McNemar's test was used. Areas and counts of detected lesions were compared using a nonparametric (Wilcoxon) test. A logistic regression model for repeated measures was used to model the probability of detected osteolytic lesions being large (> 200 mm 2 ). A Fisher exact test was used to compare proportions of lateral fusion by area. An unpaired Student t-test was used to compare the mean sizes of the lesions.
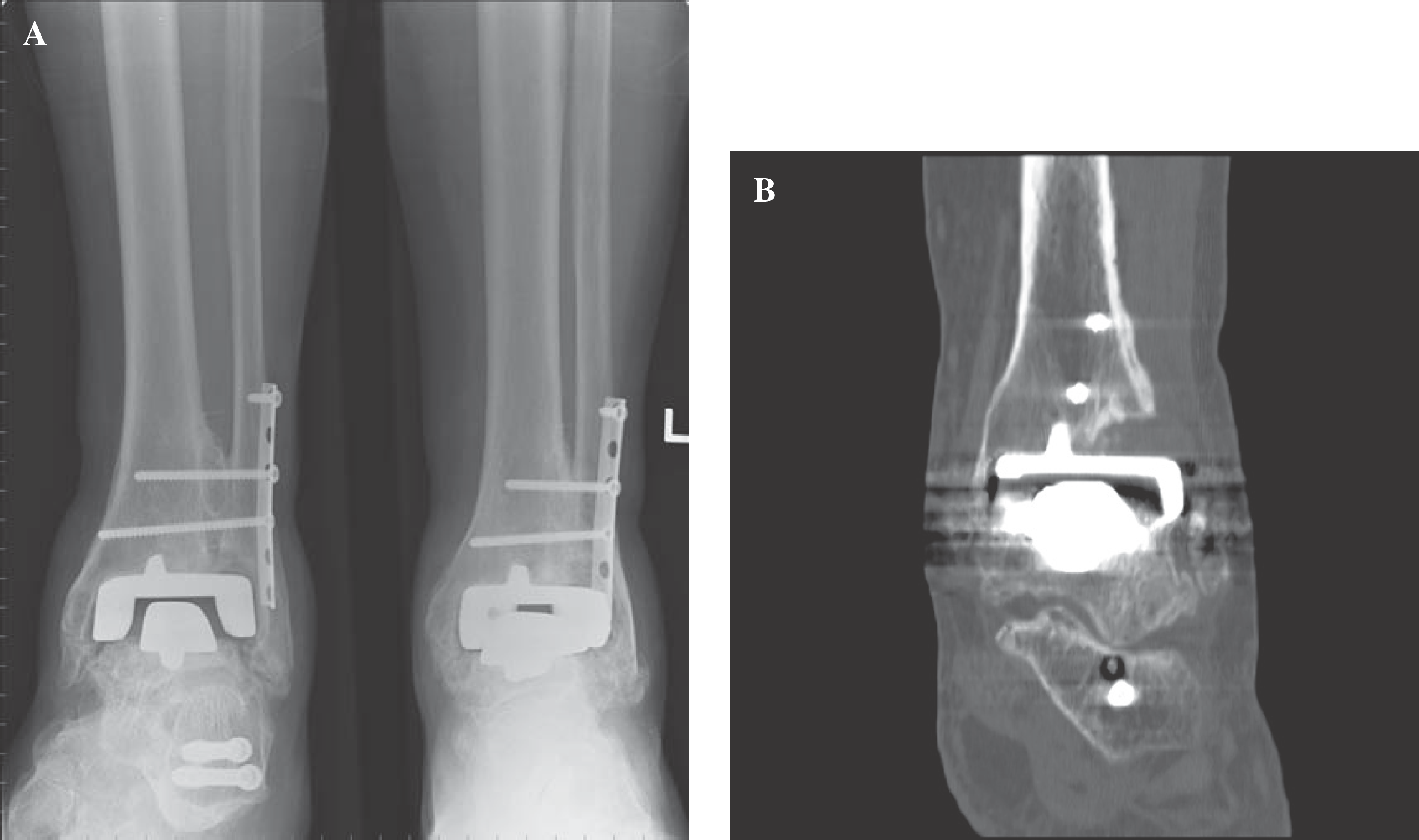
Images of a 57-year-old asymptomatic man.
All significance tests were done with an alpha of 0.05.
Results
Of the 19 imaged ankles, 18 demonstrated lesions on CT, and 13 on radiographs. In total, 29 lesions were identified on CT and 18 on radiographs. CT detected 21 lesions less than 200 mm 2 ; radiographs detected 11 such lesions. CT was more sensitive than radiographs for the detection of lesions less than 200 mm 2 . Based on these data, the sensitivity of radiographs for the identification of lesions less than 200 mm 2 was 52%, with a 95% confidence interval of 33% to 72%. The average area of a lesion seen on radiographs was 61.7 mm 2 (SD ± 113) and on CT was 187.8 mm 2 (SD ± 177) (p < 0.05) (Figures 1 and 2).
To determine if ankles that had not fused at the syndesmosis had significantly more extensive lesions than ankles with fusion, the number and mean area of lesions in ankles with and without fusion were compared on CT. Comparisons on radiographs could not be done because of the small number of ankles without fusion. The mean area of lesions was 165.1 mm 2 (SD ± 134.5) in ankles with fusion and 196.4 mm 2 (SD ± 227) in ankles without fusion. Although ankles with lack of fusion demonstrated greater mean areas on CT, these findings were not significantly different (p = 0.84). There were 12 lesions in ankles with fusion and 17 lesions in ankles without fusion. Similarly, although ankles that had not fused demonstrated a greater number of lesions on CT, the data were not significantly different (p = 0.167).
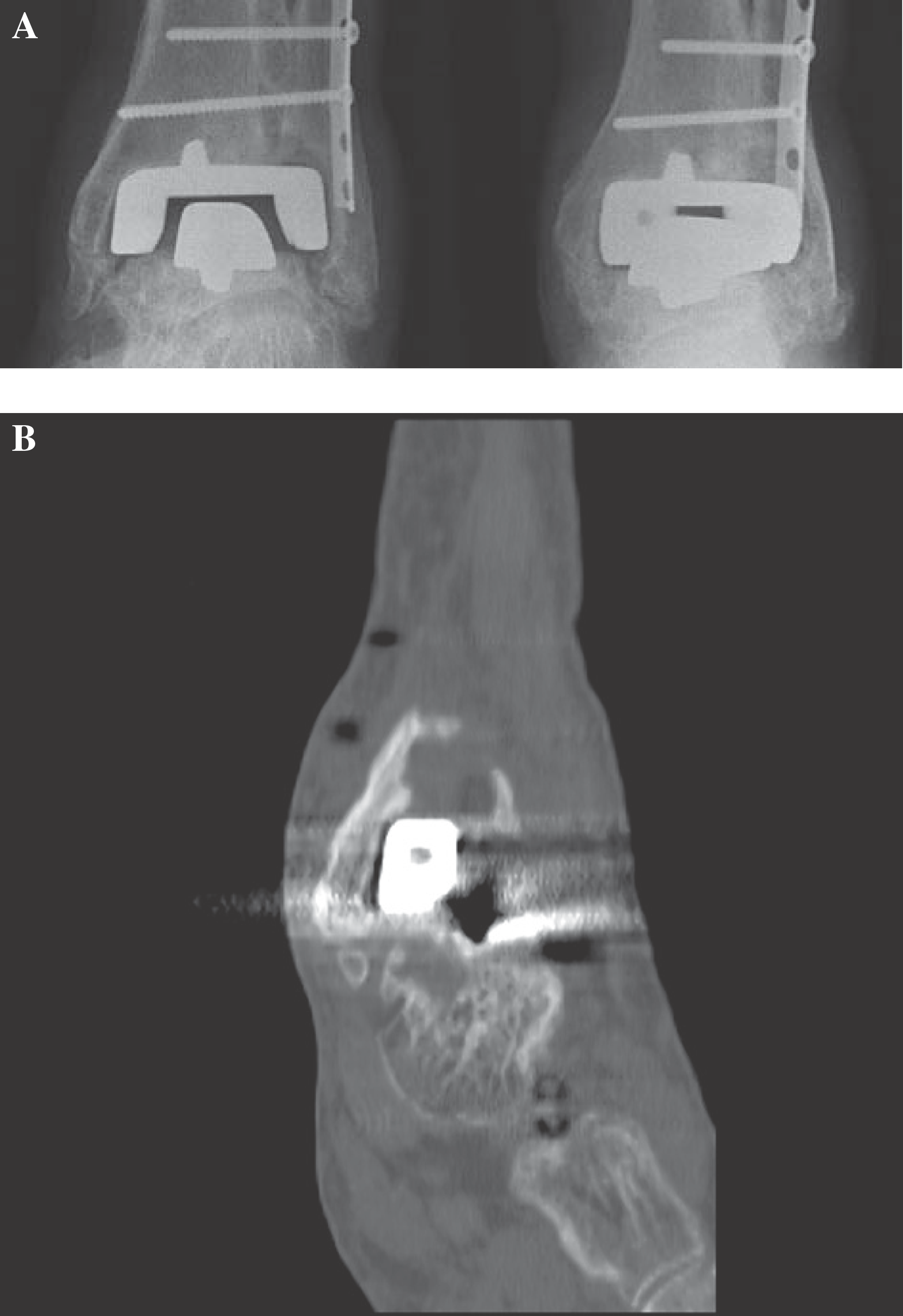
Images of a 78-year-old man.
Of the 29 lesions seen on CT, 22 involved the lateral locations (lateral tibia and fibula) and seven involved the medial locations. Of the 14 lateral tibial lesions, five ankles had not fused. Of the eight fibular lesions, five ankles had not fused. Overall, 57% (four of seven) of ankles that had not fused at the syndesmosis had exclusively lateral lesions, whereas 33% (four of 12) of ankles with fusion of the syndesmosis had exclusively lateral lesions. Similarly, only 14% (one of seven) of patients without fusion of the syndesmosis had exclusively medial or central lesions, whereas 33% (four of 12) ankles with fusion had exclusively medial or central lesions. Although almost all ankles without syndesmotic fusion had lateral lesions, these data do not demonstrate a significant difference in lesion location in ankles compared to those without fusion (p = 0.377).
In comparing CT to radiography for the detection of fusion and partial fusion of the syndesmosis, the following was observed. Seventeen of 19 (89%) ankles were fused at the syndesmosis on radiographs, one was not united and one was partially fused. Twelve of 19 (63%) ankles were fused at the syndesmosis on CT, five were not fused, and two were partially fused. Although CT was able to detect more ankles without syndesmotic fusion, these results were not statistically significant (p = 0.074) (Figure 3).
Discussion
First generation TAA implants were based on constrained and cemented designs that incorrectly treated the ankle as a single-axis dorsiflexion-plantarflexion hinge joint. Despite their inherent stability, the constrained designs transmitted most forces directly to the bone-cement interface leading to a high rate of failure through subsidence, wear, and loosening. 3,5,10,12,21 -24 Experience with these early TAA designs also demonstrated that cementless prostheses obtained better results than cemented devices. 2,4,18,22 These factors led investigators to newer designs based on uncemented and semiconstrained models that take into account the ankle's multi-axial biomechanics that maintain a normal distribution of stresses.
The implant used in this study, the Agility Ankle®, is a second-generation model with the unique incorporation of an arthrodesis of the tibiofibular syndesmosis. While this model represents significant advancement in design, complications continue to threaten long-term implant survival. Besides loosening, subsidence, and polyethylene wear, other complications include malleolar fractures, delayed wound healing, and infection. Despite the gaining popularity of this procedure, relatively little has been done in regards to the analysis of TAA complications. Relatively little is known about the onset and appearance of periprosthetic lucency as a contributing factor to loosening after TAA.
Based on the assessment of lucent lesions after total hip arthroplasty, CT was initially found to be of limited value because of the high amount of metal-produced artifact. 7 However, the use of metal-artifact minimization protocols has generated renewed interest in the use of CT scans for assessment of bone adjacent to metal joint implants. 17,19 Puri et al. 17 examined the use of helical CT for the assessment of acetabular osteolysis after total hip joint arthroplasty. This study demonstrated that helical CT with metal-artifact minimization is more sensitive for identifying and characterizing osteolysis after total hip arthroplasty than are radiographs. Studies by Leung et al. 15 also have examined CT assessment of periacetabular osteolysis. A recent study using an autopsy model demonstrated CT to be more accurate than radiographs for detecting and measuring periacetabular osteolytic lesions. 15
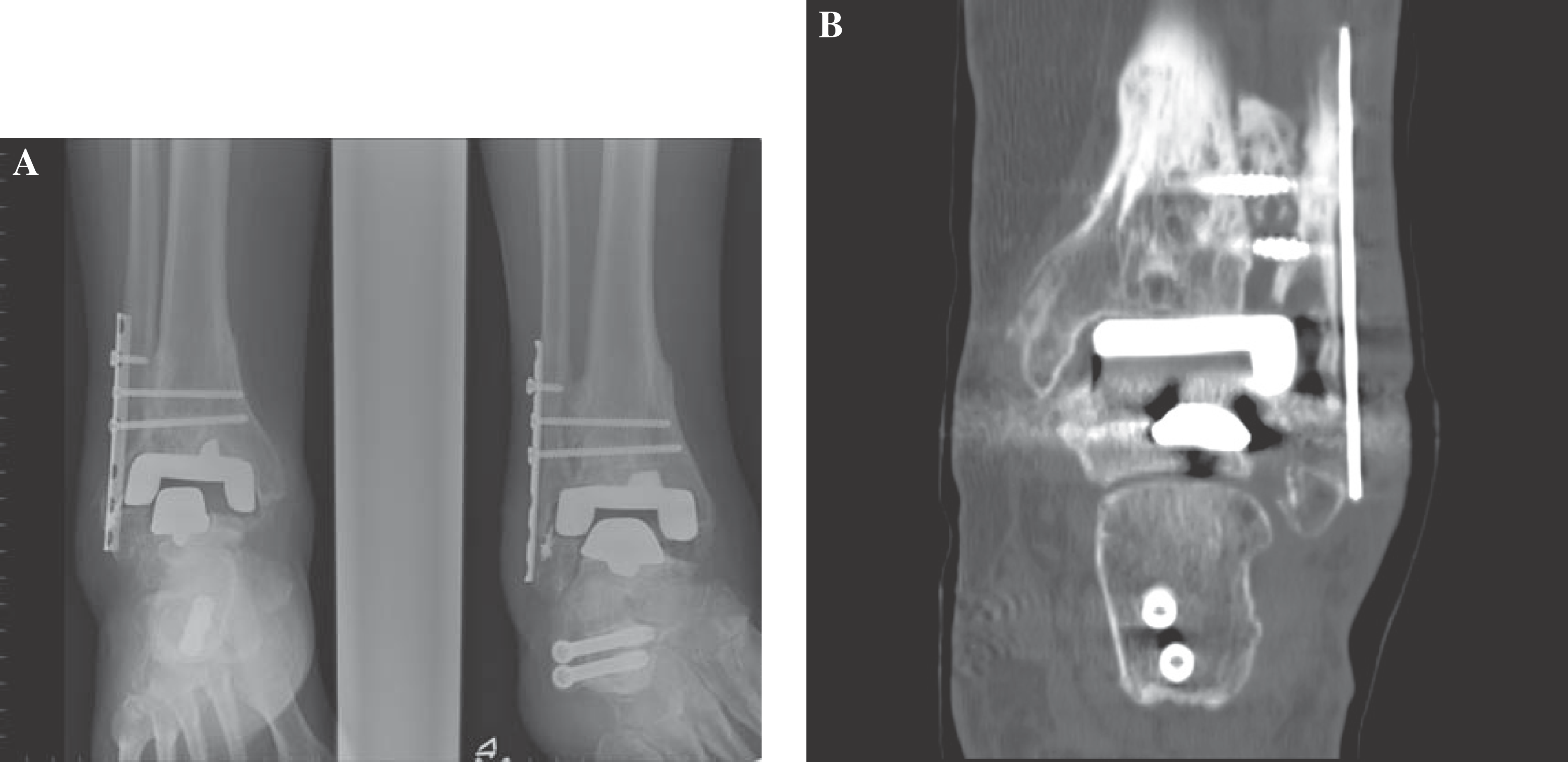
Evaluation of tibiofibular syndesmotic fusion.
The significance of periprosthetic lucency as it relates to tibiofibular syndesmotic fusion incorporated into the Ankle Agility implant technique was first examined by Pyevich et al. 18 The authors determined that fusion of the tibiofibular syndesmosis was inversely related to lateral bone lesions and had the greatest influence on tibial stability and TAA outcome. This type of lucency, referred to as “ballooning lysis,” typically occurred in the first 6 to 12 months after arthroplasty and was concurrent with delayed distal tibiofibular syndesmotic fusion. These lesions generally were nonprogressive and stabilized after syndesmotic fusion. They concluded that the early appearance and of this ‘ballooning lysis’ was a separate phenomenon from the more recognized version of osteolysis from particulate debris. “Ballooning lysis'was thought to occur from high interfascial shear stresses between the tibial prosthetic component and the residual lateral malleolus from persistent fibular rotation from lack of syndesmotic union (Figure 4). This nonunion and subsequent “ballooning lysis,” in turn, may predict impending component subsidence, migration, and loosening with an increased likelihood of prosthesis failure.
In a continuation of this study, Knecht et al. 13 went on to describe a second set of lesions referred to as “expansile lysis” that appear anywhere around the implant at a longer time interval from prosthetic implantation. They concluded that this late onset lysis, in contrast to early postoperative lysis, was consistent with true inflammatory bone loss from particulate debris. This osteolysis occurs from polyethylene wear particles inciting macrophage phagocytoses, cell death, cytokine release, and bone loss.
Although true osteolysis after TAA has not been microscopically identified to date, a number of factors suggest why this phenomenon may exist in the ankle much earlier than expected. First, the polyethylene insert used in the Ankle Agility is between 3.7 and 4.7 mm thick, compared to the standard polyethylene liner for hip (6 mm) and knee (8 mm) implants. Also, unlike mechanically assisted component alignment in hip and knee replacement surgery, ankle component placement is more surgeon-dependent and subject to iatrogenic malalignment. Thus, it is hypothesized that both the relatively thin polyethylene component and relatively imprecise operative technique creating component mismatch, can lead to loss of component conformity and increased polyethylene wear through shear stresses.
Our data demonstrated a total of 29 lesions detected on CT scans, whereas plain radiography detected only 18 such lesions. CT demonstrated a greater sensitivity than radiography for detecting lesions smaller than 200 mm 2 . In addition, radiography consistently underestimated the size of the lesions. On average, a lesion detected on CT was over three times larger than that seen on radiographs. In 14 of the 18 radiographically evident lesions, the extent of osteolysis was underestimated. Considering these findings, approximately 87% (25 of 29) of the lesions detected on CT had inaccurate radiographic interpretation. This finding is in agreement with that reported by Puri et al. 17 who found that 88% of plain radiographs inaccurately characterized lesions around hip arthroplasty components.

Coronal reformatted image demonstrates two lucent lesions within the distal fibula. The more proximal lesion represents ‘ballooning lysis,’ distinct from the more distal periprosthetic lucency. Note the lack of syndesmotic fusion.
Our limited sample size precluded significant results for our exploratory aims regarding the syndesmotic fusion. However, definite trends were observed. Lesions in ankles with lack of syndesmotic fusion had greater mean areas than ankles with successful syndesmotic fusion. Overall, most lesions were located along the lateral tibial component (14 of 29 lesions) and the fibula (eight of 29 lesions) in agreement with what has been previously reported. 19,20 Also, ankles without syndesmotic fusion demonstrated lateral lesions more exclusively than ankles with fusion, suggesting a relationship between the two. CT was able to detect a greater number of syndesmotic nonunions than plain radiographs. It is thought that fusion can be misinterpreted with radiographs, as the suspected fusion is actually tibiofibular overlap.
The major limitations of this study were the small sample size and lack of pathological correlation. With a limited number of ankles without syndesmotic union, the data did not show a statistically significant effect from this lack of fusion. Although we noticed a definite trend towards this hypothesis, the question remains whether syndesmotic nonunion leads to more extensive lateral periprosthetic lucency, which subsequently creates or contributes to implant loosening and failure. Further studies with larger sample sizes need to be done to confirm this. Another weakness of the study was the lack of an imaging gold standard with which to compare both modalities (CT and plain radiography). Without pathological correlation, it is unknown to what extent these lesions represent true inflammatory osteolysis secondary to polyethylene wear. Therefore, CT imaging, which detected more extensive and an increased number of lesions, could become the standard to which plain radiography is compared.
In conclusion, our data demonstrated a significant underestimation of the presence and extent of bone lucent lesions after ankle arthroplasty detected by plain radiographs as compared to CT scans. CT is more sensitive for early detection and more accurate for quantification of periprosthetic lucency than is plain radiography. CT findings indicate that lucent lesions, including true osteolysis, may occur much earlier and to a greater extent after TAA than was previously thought. Furthermore, trends in the data suggest that lateral ‘ballooning lysis’ may indicate a lack of fixation, evidenced by syndesmotic nonunion which was more often seen by CT. Therefore, CT may be warranted not only in patients with significant pain, but also in asymptomatic patients with radiographic evidence of lucent lesions, syndesmotic nonunion, or risk factors for the development of osteolysis, because extensive lesions may significantly affect the success of revision surgery and implant survival.