
Abstract

Introduction
Management of displaced calcaneal fractures is controversial, and multiple factors, including fracture pattern and severity, soft-tissue integrity, medical comorbidities, and lifestyle issues, influence the decision-making process. Although calcaneal fractures with an underlying tarsal coalition are uncommon, 9,14 the presence of a tarsal coalition should be considered in a patient with an intra-articular calcaneal fracture. We describe a patient who had a displaced intraarticular calcaneal fracture with an occult talocalcaneal coalition. Because of previous hindfoot symptoms related to his coalition and evidence of posterior facet subtalar joint arthritis, this patient was treated with open reduction, internal fixation, and primary subtalar joint arthrodesis. This option treated both hindfoot problems with one operation.
Case Report
A 50-year-old man presented to the emergency room immediately after falling 5 feet off a wall and landing on his left heel. Physical examination showed isolated left heel tenderness, moderate swelling, and ecchymosis, but no skin lacerations. His history was notable for a contralateral calcaneal fracture treated with percutaneous screw fixation 7 years previously. The patient, who had a history of smoking a pack per day for 30 years, was employed as a carpet installer. The patient reported a history of mild hindfoot pain and stiffness for many years before his current injury, but he had never sought medical care for this problem.
Plain radiographs showed a Sanders type-2 intra-articular calcaneal fracture with tongue-type pattern 15 (Figure 1, A) and a bony talocalcaneal coalition that was visible on an axial view (Figure 1, B). The CT scan confirmed the middle facet coalition and showed sclerosis and osteophyte formation, consistent with early degenerative changes of the left subtalar joint (Figure 2).
Initially, the patient was immobilized in a compressive dressing with a plaster splint. Eighteen days after injury, the patient's soft-tissue edema had resolved, and he was taken to the operating room. A lateral extensile incision was made, and a full-thickness flap was elevated. After opening the lateral wall, the depressed segment was disimpacted, and the posterior facet was inspected, showing chronic chondral erosions. Additional areas of acute chondral loss from the fracture also were noted. Based on these findings, a decision was made to proceed with primary fusion of the subtalar joint. The subtalar joint was debrided of cartilage, and cancellous iliac crest bone graft was packed into the subtalar joint and bony defect in the body of the calcaneus. The lateral fracture fragment then was reduced and stabilized with a 4.5-mm partially threaded cannulated screw. A 7.3-mm cannulated screw with a washer was passed percutaneously from the apex of the heel into the body of the talus. The lateral wall fragments were reduced, and a locking calcaneal plate (Synthes, Paoli, PA) was applied to stabilize the fracture (Figure 3). The incision then was closed in layers over a drain.
The incision healed fully with no infection or dehiscence. The patient was maintained nonweightbearing in a cast for 7 weeks, followed by progressive weightbearing in a fracture boot for another month. Subsequently, the patient moved out of state and did not return for followup. However, he was located and contacted by telephone 34 months after surgery, and he stated that he had resumed work as a self-employed handyman. The patient described only mild discomfort from his calcaneal fracture and stated that he had more limitations from other lower extremity fractures sustained subsequently. He reported a pain level of 3/10, based on a scale of 0 to 10, with 0 representing no pain and 10 representing pain so great the patient would prefer amputation of the affected limb.
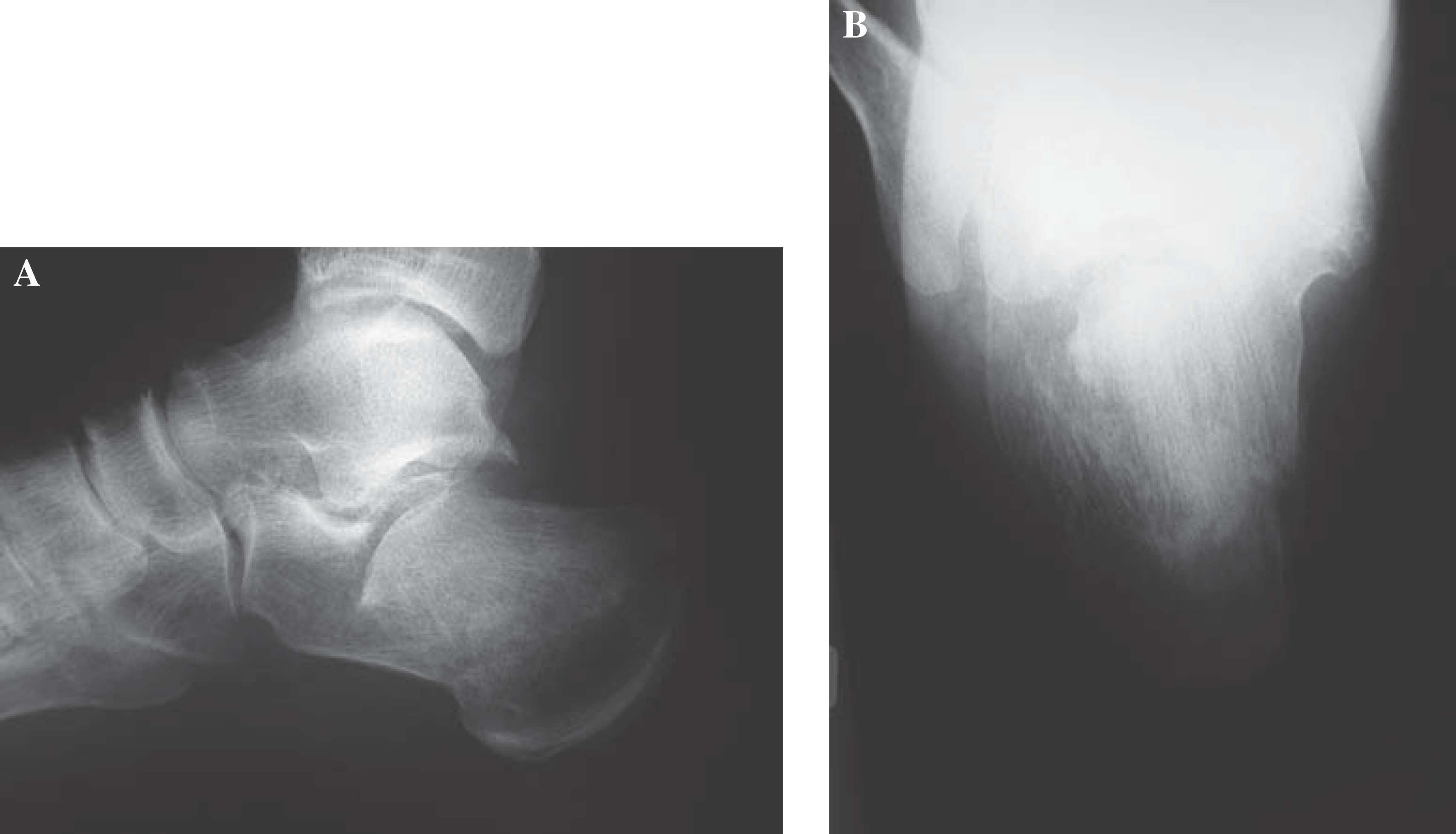
Preoperative radiographs of the left foot after injury. The lateral view
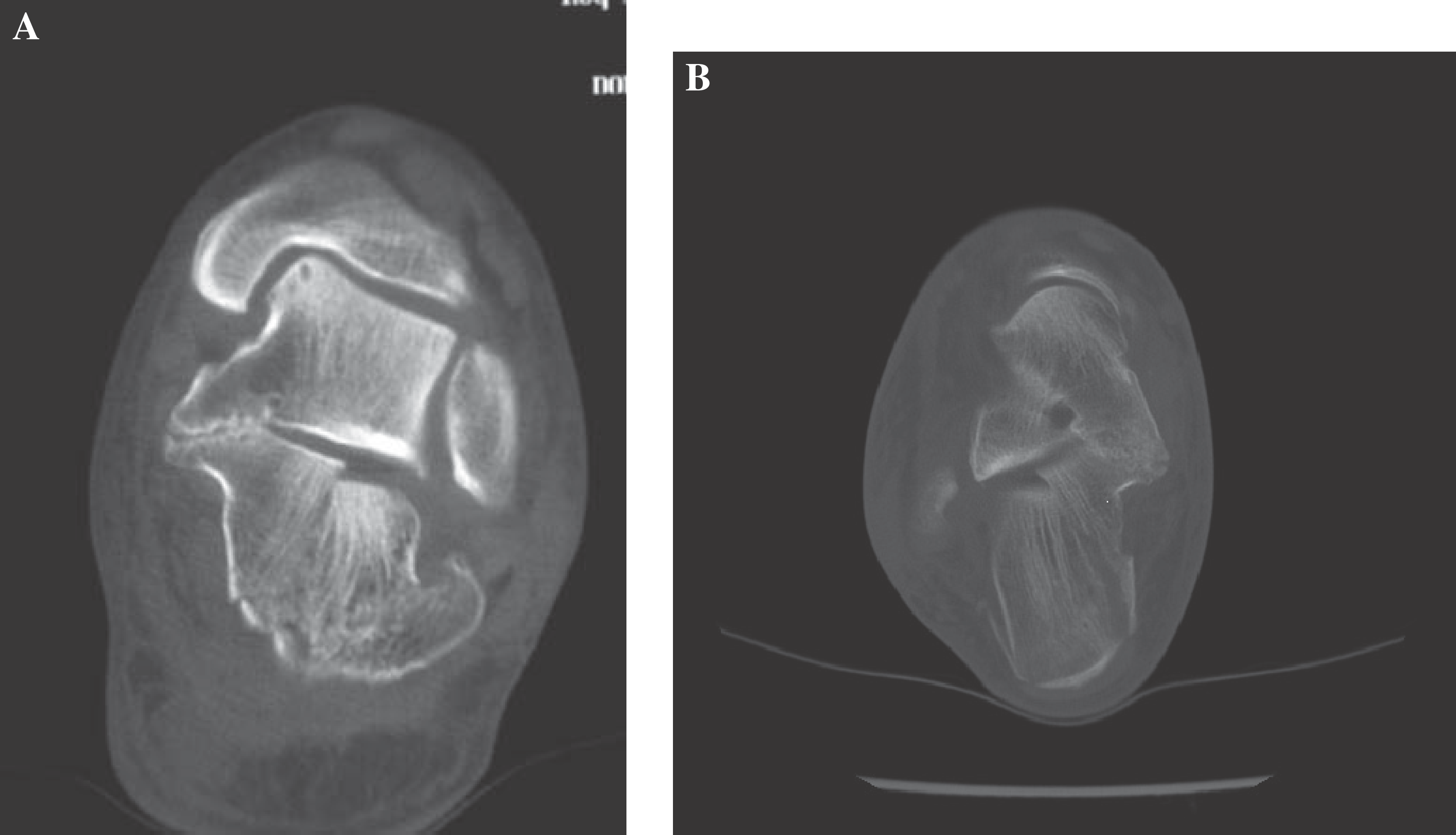
Preoperative coronal (
Discussion
Long-term morbidity is common after fracture of the calcaneus. 3,5 Risk factors for a poor outcome include fragment displacement, high degrees of comminution, lateral impingement, and injuries associated with workers'compensation. 1,5 Open reduction and primary subtalar joint arthrodesis have been recommended for comminuted fractures with extensive cartilage destruction and those in which joint congruency is difficult to obtain. 2,6 -8 Compared with delayed subtalar arthrodesis after calcaneal fracture, early reduction and fusion allow better restoration of anatomic alignment and possibly better clinical results.
Tarsal coalition, the congenital bridging of two or more tarsal bones, frequently is recognized in adolescence when the fibrous or cartilaginous bridge begins to ossify and stiffen the hindfoot, producing pain. Yet, many coalitions remain asymptomatic, and the true incidence of tarsal coalition is unknown. The most common forms of tarsal coalition are talocalcaneal and calcaneonavicular. 16 For symptomatic talocalcaneal coalitions, initial management usually includes activity modification, orthoses, or immobilization in a below-the-knee walking cast for up to 6 weeks. Surgical options depend on the size of the coalition and the degree of associated degenerative arthrosis. For coalitions that involve less than 50% of the joint without evidence of arthritis, coalition resection with interposition of fat or muscle may be attempted. If the coalition is more than 50% of the joint or is associated with degenerative joint changes, then primary arthrodesis is the treatment of choice. 10,18

A postoperative lateral radiograph 7 weeks after open reduction and internal fixation and primary subtalar joint arthrodesis shows early union of the fracture fragments and absence of the subtalar joint.
Tarsal coalition has been reported in association with fractures and dislocations. 11,14,17 Calcaneonavicular coalition was associated with traumatic foot fractures in three reported cases; of those, two patients had fractures of the coalition, one of which was associated with a subtalar dislocation that was managed nonoperatively, and one of which eventually required talonavicular arthrodesis for persistent pain after the fracture healed. 11,14 One navicular fracture near a bony bar was treated with excision of the coalition from the beak of the calcaneus to the fracture line. 17
Talocalcaneal coalitions were reported in association with a fracture in three cases. 9,12,13 In one, the patient sustained bilateral talar beak fractures, which were treated with excision of the fragments. 13 Another patient developed a stress fracture through a medial talocalcaneal coalition at the posterior facet of the subtalar joint. This fracture was treated successfully with restricted weightbearing. 12 The third patient was a 15-year-old boy who had an intra-articular calcaneal fracture with an asymptomatic talocalcaneal coalition. 9 No degenerative changes were present in the subtalar joint. Because the coalition was asymptomatic, the fracture was managed with open reduction and internal fixation, but the coalition was not treated. A good clinical result was obtained at 4-year followup.
Our report differs from the last case in several ways: our patient 1) was a middle-aged adult rather than an adolescent; 2) had a mildly symptomatic coalition, with radiographic and intraoperative evidence of early subtalar arthritis; and 3) had risk factors for a poor clinical outcome with fracture reduction and fixation without fusion, namely male gender, age, and smoking history. 4,5 In this circumstance, open reduction and primary subtalar arthrodesis offered an acceptable option for this complex injury. We believe that fracture reduction and primary subtalar arthrodesis provided this patient a better option than nonoperative management or fracture reduction and fixation without fusion, particularly in view of his risk factors for expected poor outcome with those methods. 3 -5
Conclusion
Intra-articular calcaneal fracture with an underlying tarsal coalition is unusual. Our patient was successfully treated with fracture reduction and primary subtalar arthrodesis, providing satisfactory pain relief, functional recovery, and return to work as a laborer at most recent followup almost 3 years later. Therefore, we believe that fracture reduction and primary subtalar fusion should be considered for patients with displaced calcaneal fractures and pre-existing talocalcaneal coalitions, particularly in the presence of subtalar arthritis.