
Abstract
Background: Few studies exist to guide the best practice in thromboprophylaxis after foot and ankle surgery. A survey of foot and ankle surgeons was performed to assess current trends in thromboprophylaxis. Methods: An email-based survey of American and British foot and ankle surgeons was conducted. Surgeons were questioned as to their use and type(s) of thromboprophylaxis as well as reasons for not using prophylaxis. Surgeons also were asked about their use of thromboprophylaxis in hip and knee arthroplasty, if they did these surgeries. Results: Nearly one-fifth (19%, 27) of surgeons routinely used thromboprophylaxis in both elective and trauma foot and ankle surgery. The most common situation for use was in a postoperative patient who was immobilized and nonweightbearing. A lack of published evidence and a low rate of thromboembolism were the most commonly cited reasons for not using thromboprophylaxis. Conclusions: This survey showed a wide variability in thromboembolic prophylaxis. It suggests that despite the literature indicating to the contrary, a significant proportion of foot and ankle surgeons routinely use thromboprophylaxis. Confusion remains regarding the appropriateness of thromboprophylaxis and what type(s)(if any) should be used. This study has identified a need for more in-depth evaluation of the importance of, and possible prophylaxis against, thromboembolic problems after foot and ankle surgery.
INTRODUCTION
Thromboembolism is a significant cause of morbidity and mortality in orthopaedic surgery. Despite being well recognized in hip and knee arthroplasty, 4,12,13 there currently is little scientific literature to guide best practice with regard to chemical thromboembolic prophylaxis in foot and ankle surgery. Few studies have been performed looking specifically at the incidence of thromboembolic disease after surgery of the foot and ankle. 3,9,10,11 These studies found that the risk for venous thrombosis is low and concluded that routine deep vein thrombosis (DVT) prophylaxis is not indicated in the most patients undergoing foot and ankle surgery. The purpose of this study was to evaluate trends in the use of thromboembolic prophylaxis among American and British foot and ankle surgeons.
MATERIALS AND METHODS
A survey (Table 1) was e-mailed to surgeons involved in the treatment of foot and ankle problems, all of whom were members of the American Orthopaedic Foot and Ankle Society (AOFAS) or the British Orthopaedic Foot Surgery Society (BOFSS). In order to receive a survey, surgeons had to be active society members and have an active e-mail address. Surgeons were identified from their respective society directories. If no reply was received at 12 weeks, a second e-mail survey was sent.
Questionnaire received by American Orthopaedic Foot and Ankle Society and the British Orthopaedic Foot Surgery Society
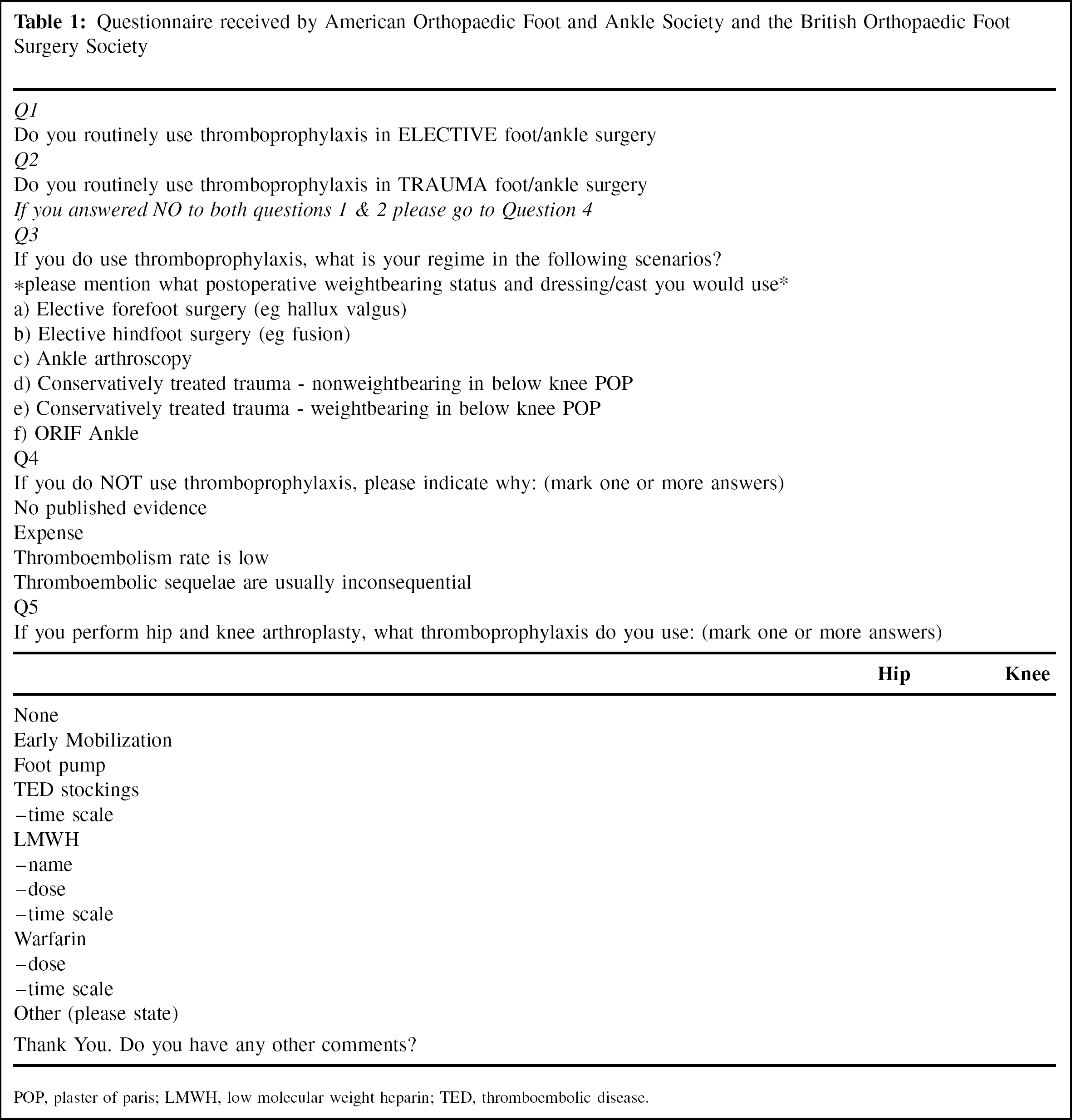
POP, plaster of paris; LMWH, low molecular weight heparin; TED, thromboembolic disease.
RESULTS
One hundred and forty replies were received from 455 questionnaires, a response rate of 31% (Table 2). Similar rates of response were received from American and British surgeons (30% and 33%, respectively). Returned surveys were included if part of each of the questions was answered.
Responses regarding use of thromboprophylaxis in clinical settings
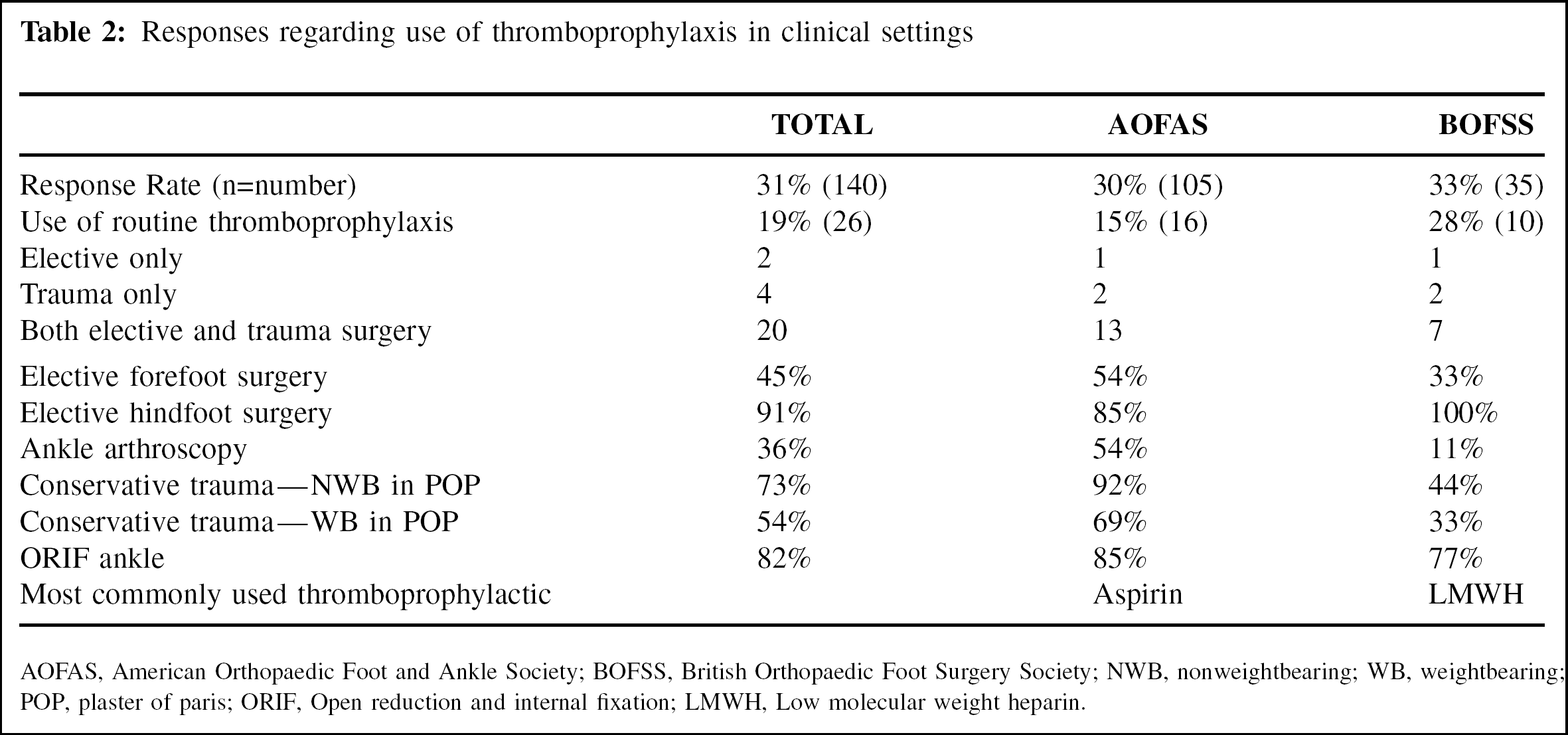
AOFAS, American Orthopaedic Foot and Ankle Society; BOFSS, British Orthopaedic Foot Surgery Society; NWB, nonweightbearing; WB, weightbearing; POP, plaster of paris; ORIF, Open reduction and internal fixation; LMWH, Low molecular weight heparin.
Overall, 19% of surgeons routinely used thromboprophylaxis in either elective or trauma foot and ankle surgery. Of those who used thromboprophylaxis, most used it for both elective and trauma patients. The most common situations in which thromboprophylaxis were used were elective hindfoot surgery, open reduction and internal fixation (ORIF) of the ankle, and trauma treated conservatively with nonweightbearing (NWB) in a plaster cast. These may all be linked by the fact that the patient is likely to be nonweightbearing with immobilization for a period of time.
The most common form of prophylaxis was aspirin by AOFAS members and low-molecular weight heparin (LMWH) by BOFSS. However, there was variability in types of treatment. Aspirin was used with doses varying from 81 mg once a day to 325 mg four times daily. The length of treatments also varied considerably.
Those surgeons who did not routinely use thromboprophylaxis were then questioned regarding their reasons for not using it (Table 3). Surgeons could give more than one answer to this question. The most frequently cited reasons for not using medical thromboprophylaxis were lack of published evidence for its use and the fact that the rate of thromboembolism was believed to be low. When asked if the sequelae of thromboembolism are inconsequential or if clots are nonprogressive, only 8% agreed. No British surgeon was concerned about the cost of using parenteral prophylaxis.
Reasons given for not using routine thromboprophylaxis
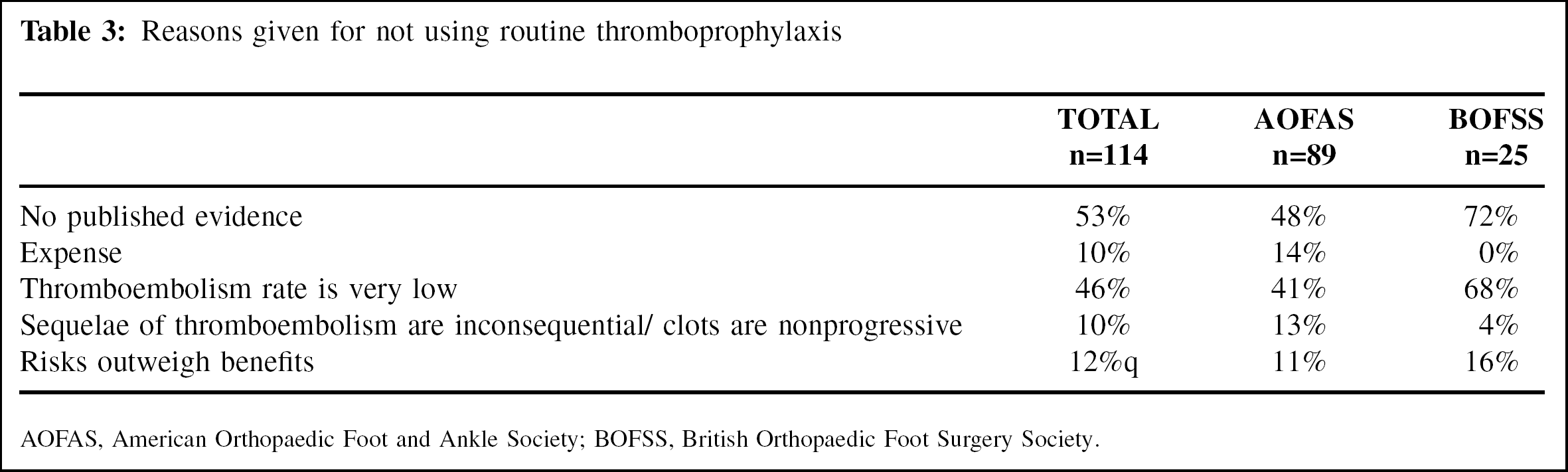
AOFAS, American Orthopaedic Foot and Ankle Society; BOFSS, British Orthopaedic Foot Surgery Society.
Despite being members of their national foot and ankle societies, a high proportion of surgeons also performed other lower limb arthroplasty procedures (Table 4). Only one surgeon used no parenteral prophylaxis for hip, knee, or foot and ankle surgery; 77% of surgeons used thromboprophylaxis for hip and knee surgery but not for foot surgery.
Responses regarding thromboprophylaxis use in hip and knee arthroplasty
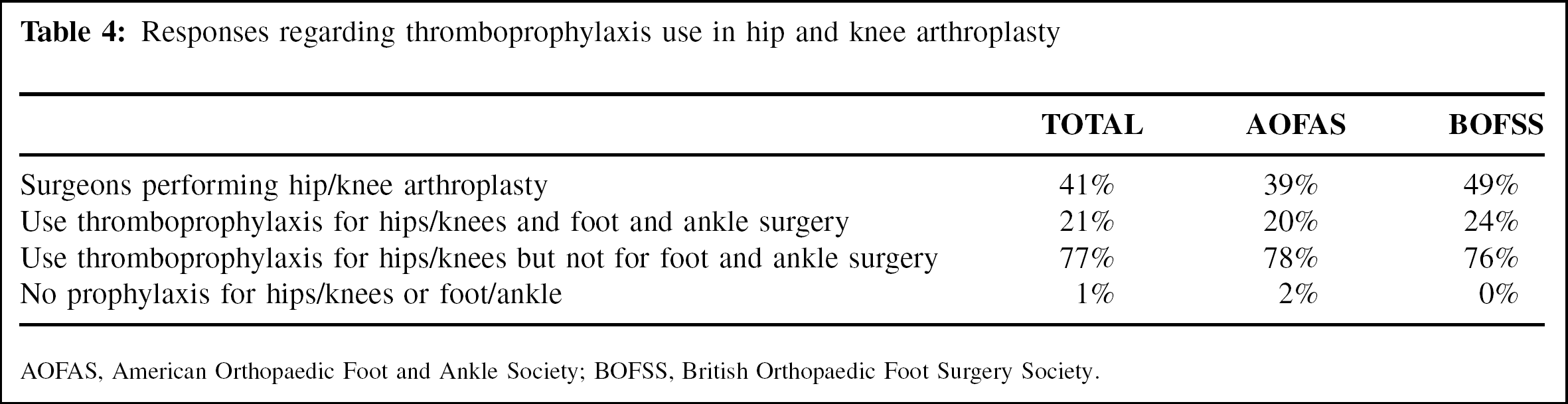
AOFAS, American Orthopaedic Foot and Ankle Society; BOFSS, British Orthopaedic Foot Surgery Society.
DISCUSSION
In comparison to the extensive literature regarding thromboembolism and its prophylaxis in hip and knee surgery, there is a paucity of information regarding this subject in the foot and ankle literature. Only a few studies have tried to calculate the frequency of thromboembolic disease and its associated risk factors. 3,9,10,11 Apart from these studies other literature on the subject consists mainly of case reports 14 or studies in trauma patients with cast immobilization. 7,8
The largest study involved multiple surgeons. 9 Over 2,700 patients undergoing foot and ankle procedures were observed for clinically detectable thromboembolic disease. The use and type of thromboprophylaxis for each patient was determined by the treating surgeon, as well as the type, if any, of radiographic investigation. Six patients (0.22%) had clinical DVT confirmed by Doppler ultrasound or venogram. Four DVTs were associated with nonfatal pulmonary emboli (0.15%) including both the above knee DVTs. The low thrombosis rate may have been an under-estimation because clinical diagnosis alone has been shown to be an inaccurate method of detection and many thrombi are asymptomatic. 1 The DVT rate in those not receiving routine medical prophylaxis was 0.16%.
Solis and Saxby 11 evaluated 201 consecutive patients undergoing a variety of procedures. All were investigated for calf thrombus using bilateral duplex ultrasound at the first postoperative visit. If a DVT was diagnosed, a second scan was performed a week later to evaluate clot progression. Thirteen patients were found to have positive scans. Of these, six were in superficial veins and muscular plexuses.
This left a true DVT rate of 3.5%, with 2.5% of all patients having occlusive clots. As no clot was found to be proximal to the calf no treatment was implemented. At further ultrasound investigation, no clot was found to have progressed. No patient with a duplex proven venous thrombosis was clinically symptomatic.
Radl et al. 10 looked at the occurrence of thromboembolism after chevron osteotomy of the hallux in 100 patients. No patient received medical thromboprophylaxis, but high-risk patients were excluded from the study. Using unilateral phlebography at 4 weeks postoperatively, they found four patients with distal DVT. No patient was clinically symptomatic for either DVT or pulmonary embolism.
Hanslow et al. 3 evaluated 602 elective and trauma patients for thromboembolic disease and detected a postoperative DVT in 4%. Pulmonary emboli occurred in 1.3%.
Possible factors associated with an increased risk of a thromboembolic event also have been studied. 3,9,10,11 Mizel et al. 9 found that an increased incidence of deep vein thrombosis correlated with nonweightbearing status and immobilization after surgery. Solis and Saxby 11 found associations with hindfoot surgery (with or without immobilization); increasing age and tourniquet time. Occlusive DVT was associated with hindfoot surgery and an increased body mass index. The only correlating factor found after hallux valgus surgery was age older than 60 years. 10 Hanslow et al. 3 identified a history of rheumatoid arthritis, recent air travel, previous thromboembolic disease, and limb immobilization as being risk factors. Patients deemed to be at risk (history of DVT or malignancy, oral contraceptive use, obese) were given low-molecular weight heparin. The authors noted an interesting inverse relationship between thromboembolic disease and prophylaxis with low-molecular-weight heparin, postulating that this may be due to the fact that the at-risk group for DVT was correctly identified but that the types of prophylaxis were suboptimal.
Current literature has therefore recommended that routine DVT prophylaxis is not indicated in patients undergoing foot and ankle surgery. 9,11 Radl et al. 10 suggested that patients over 60 years of age may benefit from medical prophylaxis against thromboembolism. Hanslow et al. 3 suggested that those identified as at risk may benefit from a home course of low-molecular-weight heparin.
Patients who had a previous history of thromboembolism were excluded from two recent studies. 10,11 Solis and Saxby 11 excluded such patients because it was their routine policy to place these patients on prophylactic anticoagulants. Radl et al. 10 also excluded such patients, as well as those over 75 years or over 100 kg and patients with medical conditions that might place them at increased risk of a thrombotic event. Therefore, it seems reasonable to conclude that such patients could be appropriately treated with some form of thromboprophylaxis.
This survey showed a wide variability in thromboembolic prophylaxis, suggesting that, despite the literature indicating its sparse use (19%), many foot and ankle surgeons routinely use thromboprophylaxis. Confusion remains regarding the appropriateness and type(s) of thromboprophylaxis.
A recent study surveying the use of thromboprophylaxis in foot and ankle trauma 15 reported similar confusion. The study was aimed at a group of patients believed to be at increased risk of thromboembolism. Such patients had received an acute traumatic injury, were immobilized, and were released for delayed definitive management. It was found that fewer than 50% of surgeons treating such a population used prophylaxis, but 70% believed that it was sometimes necessary.
While having a number of weaknesses, this questionnaire-based survey was designed to assess surgeons' attitudes about thromboembolic prophylaxis in foot and ankle surgery and to assess whether further information on this subject was necessary. The response rate of the study was low but was similar to that found in other studies. 15 The fact that the study was voluntary may give rise to selection bias. An e-mail questionnaire allows individual identification that may account for a low response rate. Some surgeons may have changed their e-mail address since publication of the directory.
A number of questions remain unanswered. The literature suggests that the rate of thromboembolism is low, although high rates have been reported, particularly after an injury. 8 While proximal thrombosis is an established cause of pulmonary embolism, the consequences of below-knee DVT are uncertain in both the short and long-term. 5,6 The fact that most DVTs appear at a sub-clinical level 9,10,11 also questions their importance.
A few surgeons in this study quoted medicolegal issues as being a cause of their using thromboprophylaxis, and one surgeon indicated that it was standard hospital policy. Such factors may develop more importance with the publication of new guidelines for venous thromboembolism and its treatment in operative patients. 2
This study identified a need for a more in-depth evaluation of the importance of, and possible prophylaxis against, thromboembolic problems after foot and ankle surgery.