
Abstract
Background: This study compared the effects of lateral column lengthening and medial translational calcaneal osteotomy on pedal realignment and degeneration of adjacent hindfoot joints noted on radiographs. Methods: Forty patients who had either a lateral column lengthening (25 feet) or calcaneal osteotomy (17 feet) to reconstruct a flatfoot were retrospectively reviewed as two groups. Six parameters of foot alignment were measured from weightbearing preoperative, early postoperative, and latest followup radiographs. The magnitude of realignment achieved initially and preserved at latest followup was determined for each group. The talonavicular and subtalar joints were graded for radiographic evidence of arthritis before the reconstruction and at latest followup. Demographic information, complication rate, and reoperation associated with each group also were determined by chart review. Results: The group that received a lateral column lengthening demonstrated a greater initial realignment than the group treated with a calcaneal osteotomy. The lengthening group also demonstrated greater realignment than the osteotomized group when they were compared at their respective latest followup. The lengthening group had a higher number of adjacent joints with progression of arthritis. The rate of nonunion was higher with a lateral column lengthening; however, the rate of reoperation after an osteotomy was more than twice that observed after a lateral column lengthening. Conclusions: The lateral column lengthening group achieved greater realignment initially and maintained correction better over time than the calcaneal osteotomy group while having a lower reoperation rate despite a higher incidence of nonunion and radiographic progression of adjacent joint arthritis.
INTRODUCTION
A medial translational osteotomy (MTO) of the calcaneus, a lateral column lengthening (LCL) or both have been combined with transfer of the flexor digitorum longus to the midfoot to reconstruct a painful acquired adult flatfoot secondary to dysfunction of the posterior tibial tendon. Numerous published studies have documented relief from pain, improved alignment, and increased function with these procedures. 3,7,10,13,18,22,23,27,29,31 These reports of clinical success have made the MTO and LCL prevailing bony procedures for reconstruction of adult acquired flatfoot deformity. However, little comparative evidence exists to guide the choice of which procedure to use. A recent evidence-based review found fair and insufficient evidence in the literature to support the use of a calcaneal osteotomy and lateral column lengthening, respectively. 21 A recent survey of academic orthopaedic foot and ankle surgeons identified a predilection for MTO over LCL; 12 however, the study did not solicit the surgeons’ rationale for their preferences. Some surgeons maintain that realignment is paramount; advocating full restoration of pedal alignment to maximize the longevity of the reconstruction and to eliminate the presence of abnormal contact stress within the ankle and increased strain on the longitudinal arch associated with increased valgus of the hindfoot. 2,8 Others contend that clinical success is not contingent upon the complete static correction of the deformity. They assert that a less invasive and more dynamic correction, achieved through bony procedures that redirect muscle forces, diminishes the morbidity and risk of complications associated with the reconstruction without compromising the outcome. 19,20
No biomechanical study directly compares the effect of these procedures. Three separate biomechanical studies evaluating the effect of a calcaneal osteotomy on tibiotalar contact characteristics have observed that the location of weightbearing forces in the ankle moves in the direction of the translated tuberosity. 4,11,26 CT with simulated weightbearing demonstrated a reduction of the posterolaterally subluxated subtalar joint after LCL of the foot. 6 These results indicate that both procedures alter the kinematics of the ankle and hindfoot but do not justify a partiality for one over the other in the clinical decision-making process.
A comparison of the effects of MTO of the calcaneus and LCL on the alignment and functional outcome of the foot may advance our understanding of their roles in the operative management of adult acquired flatfoot deformity. The purpose of this investigation was to compare the changes in six radiographic parameters of pedal station over time in a series of patients who had reconstruction with either one of the two procedures. The subtalar and talonaviuclar joints were assessed and graded for the presence of osteoarthritis before and after reconstruction to identify radiographic evidence of hindfoot degeneration. This study also compared rates of complications and reoperations for each procedure. The results of these comparisons may reveal differences in the capacity of these two procedures to realign a flexible flatfoot, to preserve the initial correction achieved by the reconstruction, and to avoid postoperative complications and the need for subsequent surgery.
MATERIALS AND METHODS
This investigation was approved by the Institutional Review Board of the University of Chicago Medical Center under an expedited review with a waiver of informed consent.
A consecutive series of 40 patients who had reconstruction for adult acquired flatfoot deformity with either LCL through distraction arthrodesis of the calcaneocuboid joint or MTO of the calcaneus were identified from the database of the senior author (B.C.T). An adult acquired flatfoot deformity was defined as flattening of the medial longitudinal arch with increased valgus alignment of the hindfoot, increased abduction of the midfoot, and increased varus alignment of the forefoot when the foot was inspected with the patient standing. Every flatfoot in this series was considered flexible because it could be corrected to a plantigrade posture with manual manipulation. Nonoperative management failed in all patients in this series. For the purpose of this study, patients were divided into two groups based on which procedure was used to realign the hindfoot. One patient in each group had staged, bilateral reconstructions; thus, a total of 42 feet were included in this retrospective review. The first 25 consecutive reconstructions used LCL to realign the hindfoot. The subsequent 17 reconstructions had MTO. In addition to the procedure chosen for hindfoot correction, every patient had three other procedures on their foot during surgery. The flexor digitorum longus tendon was transferred to the navicular to reconstruct the deficient posterior tibial tendon, the gastrocnemius tendon was recessed to eradicate the equinus contracture, and a plantar translational arthrodesis of the first tarsometatarsal joint was used to correct the varus deformity of the forefoot.
The medical record of each patient was reviewed to ascertain specific details regarding their preoperative status and postoperative course. Citations regarding age, dates of surgery, the healing of the bony procedures, the nature and prevalence of complications and subsequent additional operations were pulled from the progress notes. The preoperative American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot score, obtained prospectively before surgery, was recorded for each reconstruction. 15,30
Description of Study Groups
The mean followup was 35 (range 12 to 96) months for the LCL group and 26 (range 12 to 48) months for the MTO group. Nineteen women and five men comprised the LCL group, and 15 women and one man comprised the MTO group. The mean age at the time of reconstruction was 49 (range 28 to 68) and 44 (range 16 to 55) years, respectively, for the LCL and the MTO groups. The mean preoperative AOFAS scores were 38 (range 17 to 59) and 44 (range 17 to 65) points for the LCL and MTO groups, respectively. There were no significant differences in the mean ages or preoperative AOFAS scores between the groups. Six patients in the LCL group and seven in the MTO group were treated under Workers’ Compensation. Three patients in the LCL group (13%) and five patients (31%) in the MTO group admitted to smoking during the postoperative period.
Radiographic Evaluation
Six, previously described parameters of pedal alignment were measured from weightbearing anteroposterior and lateral radiographs of each patient at three time points: preoperative, early postoperative (less than 4 months after reconstruction), and latest followup. 29 On the anteroposterior radiographs, the talo-first metatarsal (TMT), talocalcaneal (TC), and talonavicular coverage (TNC) angles were measured. On the lateral radiographs, the TMT, TC, and calcaneal pitch (CP) angles were measured. The mean value and standard deviation were determined for each parameter at each time point for the two groups (Figures 1 through 6).

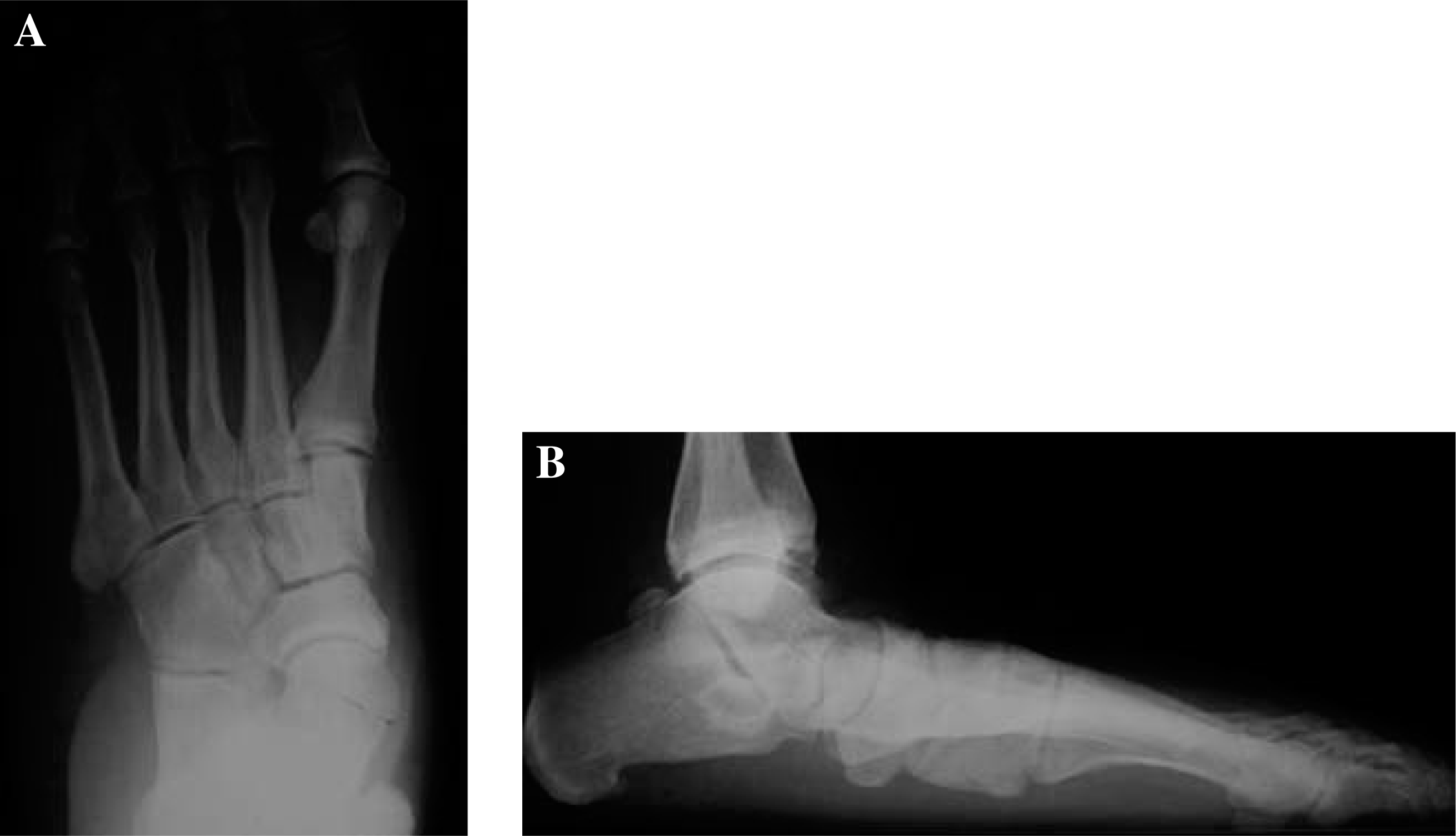
Preoperative, weightbearing radiographs in a 55-year-old woman with symptomatic flatfoot.

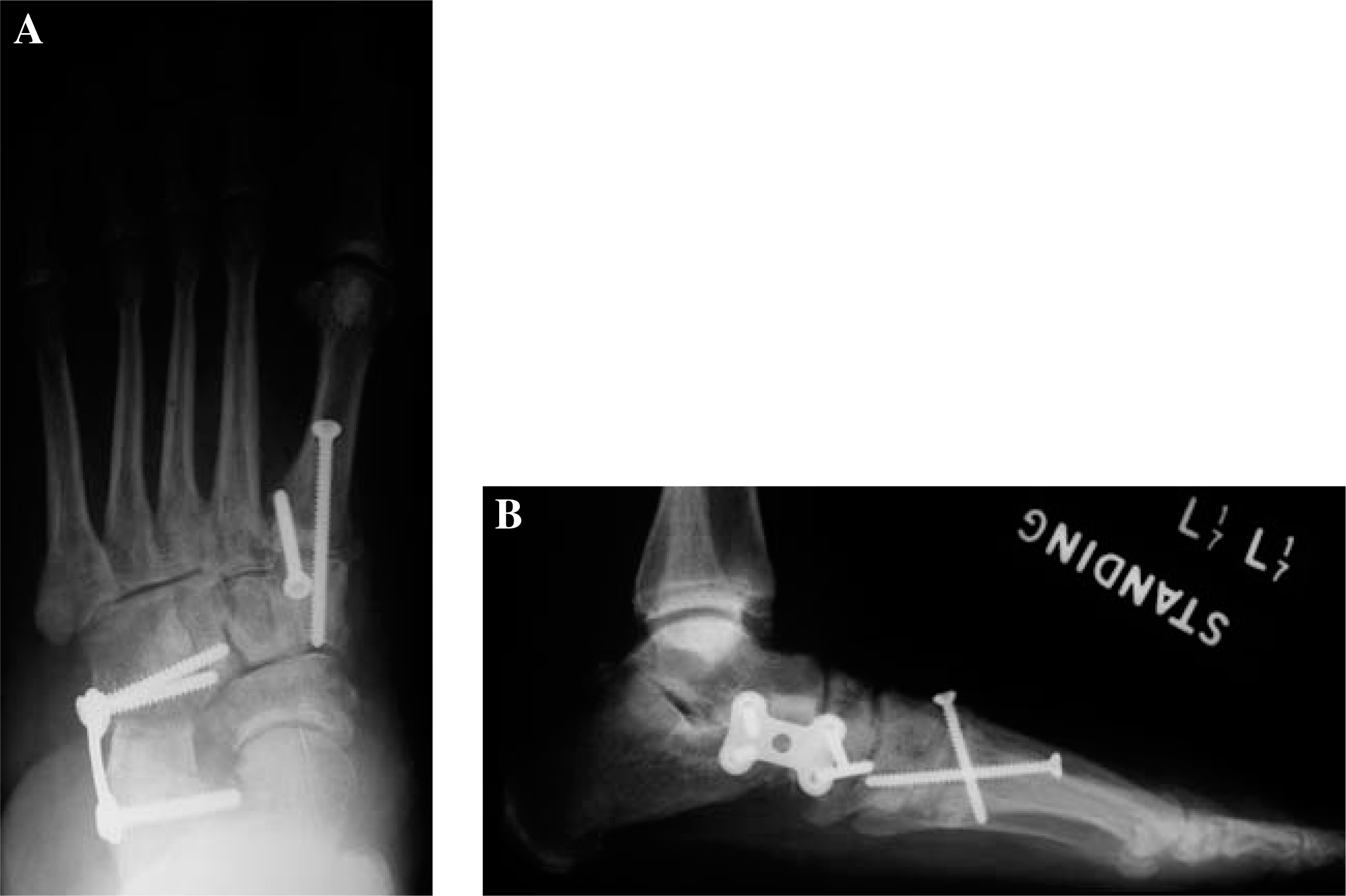
Weightbearing anteroposterior and lateral radiographs of the same patient taken 3 months after reconstruction with a medial translational osteotomy of the calcaneus.
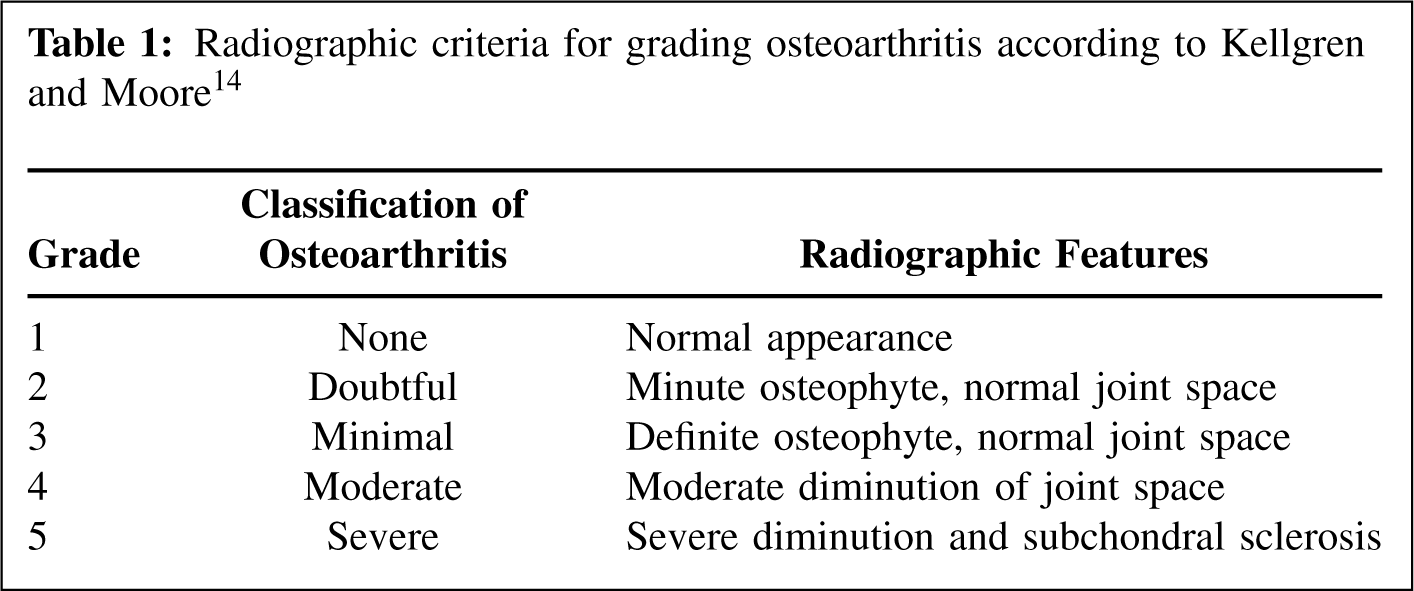
The talonavicular and subtalar joints were graded for osteoarthritis according to the classification system of Kellgren and Moore. 14 Using the preoperative and latest followup radiographs, the appearance of these joints were assigned a grade between one and five based on the presence and magnitude of periarticular osteophyte formation and the diminution of the joint space (Table 1).
Radiographic criteria for grading osteoarthritis according to Kellgren and Moore 14
Statistical Analysis
Multiple t-tests were used to analyze the age, preoperative AOFAS score, and the radiographic data of the two groups. Statistical significance was set at a p ≤ 0.05 for each test.
Operative Techniques
The technique used in this study to perform LCL through a distraction arthrodesis of the calcaneocuboid joint has been previously published in detail elsewhere. 28 The amount of distraction necessary to correct the flatfoot was determined by visual inspection of the position of the medial longitudinal arch and calcaneal tuberosity. A contoured tricortical graft from the anterior iliac crest was inserted into the calcaneocuboid joint with the foot held in this position. A cervical H-plate and four cortical screws (Synthes, Paoli, PA) stabilized the distraction-arthrodesis.
The MTO was performed as originally described by Gleich 9 and subsequently modified by others. 17,22 The osteotomized tuberosity was translated medially 1 cm and fixed with two 6.5-mm partially-threaded cancellous lag screws (Synthes, Paoli, PA) directed parallel to the longitudinal axis of calcaneus and perpendicular to the osteotomy.
The plantar translational arthrodesis of the first tarsometatarsal joint was performed through a dorsal approach. The first metatarsal was translated plantarwards between 2 and 5 mm relative to the medial cuneiform until the varus deformity of the forefoot was resolved. The arthrodesis was stabilized with two, crossed 3.5-mm cortical lag screws (Synthes, Paoli PA).
The flexor digitorum longus was transferred to the navicular through a bone tunnel in its tuberosity. The transferred tendon was tensioned and sutured in place with the foot in slight plantarflexion and inversion after the bony procedures had been performed. The gastrocnemius recession was performed as described by Strayer. 25 It was always the first procedure performed during the surgery to resolve the equinus contracture before reconstructing the foot.

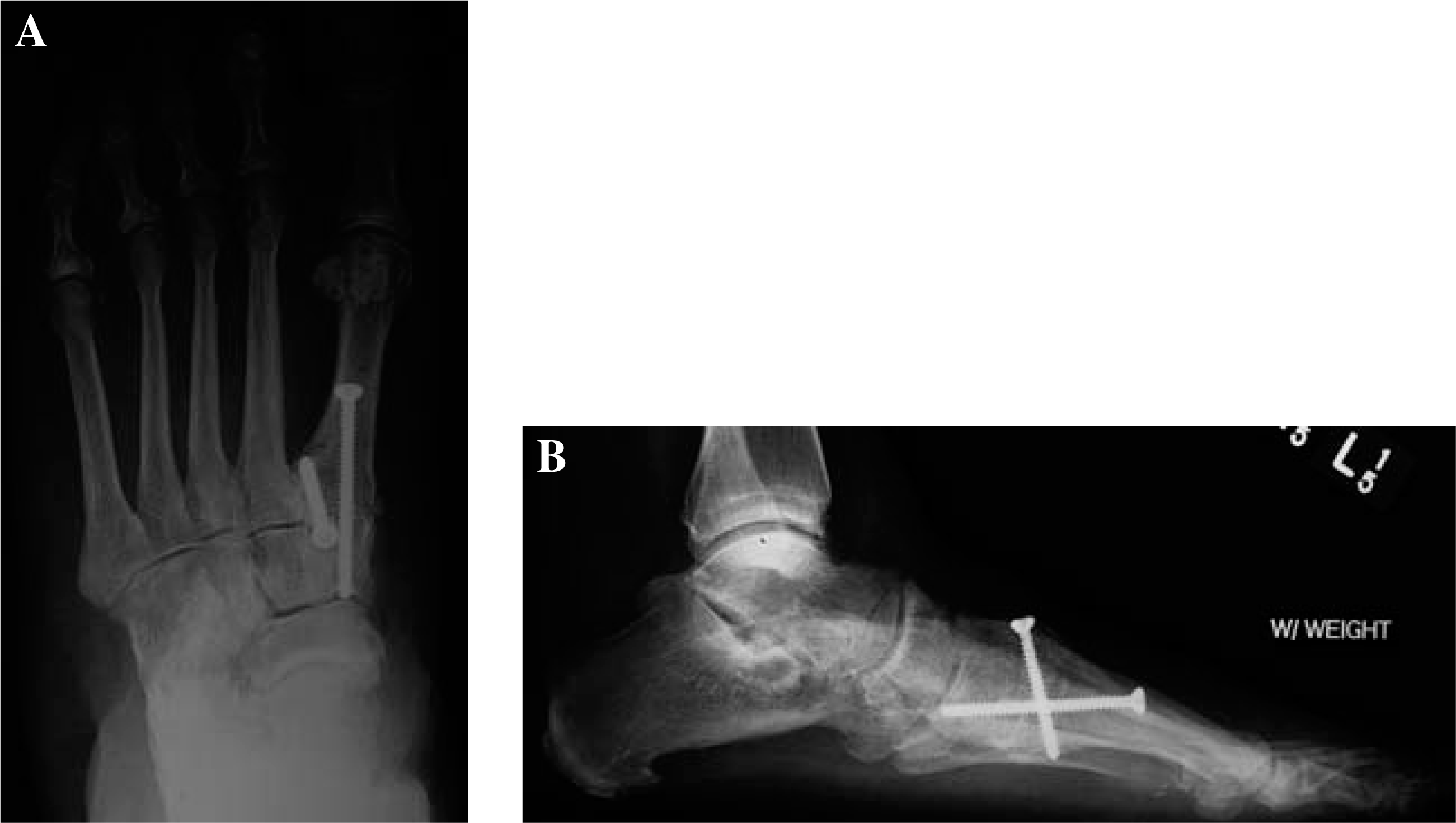
Weightbearing anteroposterior and lateral radiographs of the same patient taken 41 months after reconstruction.
Preoperative, weightbearing radiographs in a 56-year-old woman with symptomatic flatfoot.
Postoperative Care
All feet were immobilized for 6 weeks in a nonweightbearing short-leg cast after surgery. A commercial walkerboot was used after casting as the patient began a standardized protocol of supervised physical therapy to restore strength, range of motion, and full weightbearing function to the reconstructed foot. Within 16 weeks after surgery, all patients demonstrating bony healing wore shoes with a noncustom foot orthosis. Patients with delayed or no healing of the bone received physical therapy but were not progressed to full weightbearing in shoes until healing or additional surgery had occurred.
Weightbearing anteroposterior and lateral radiographs of the same patient taken 4.5 months after a reconstruction with a lateral column lengthening.
Weightbearing anteroposterior and lateral radiographs of the same patient taken 60 months after reconstruction.
RESULTS
Rates of Complications and Additional Surgeries
Three LCL procedures did not unite. All nonunions failed to heal at the interface between the graft and calcaneus. All nonunions subsequently healed with cancellous bone grafting, and revision of the internal fixation. Six patients had removal of painful hardware at the LCL site, with resolution of their symptoms. The first tarsometatarsal arthrodesis did not heal in two patients in this group and required cancellous bone grafting, and revision of internal fixation were required. One of the patients who had a nonunion of the LCL and one who had a nonunion of the tarsometatarsal arthrodesis smoked cigarettes. Overall, nine of the 25 reconstructions with a lengthening required additional surgery.
One MTO did not unite and required revision of the internal fixation. Nine patients had removal of the calcaneal screws to eliminate posterior heel pain. The arthrodesis did not heal in one patient who smoked until it was treated with cancellous bone grafting and revision internal fixation. Overall, 10 of the 17 reconstructions with an osteotomy required additional surgery.
Table 2 presents the mean values of the six parameters measured on the anteroposterior and lateral radiographs of the two groups. The preoperative mean values did not vary significantly between the two groups in four of the six comparisons. The TNC angle (p = 0.049) and lateral TMT angle (p = 0.0000.4) were the two measurements that differed significantly on the preoperative comparisons.
Angle measurements
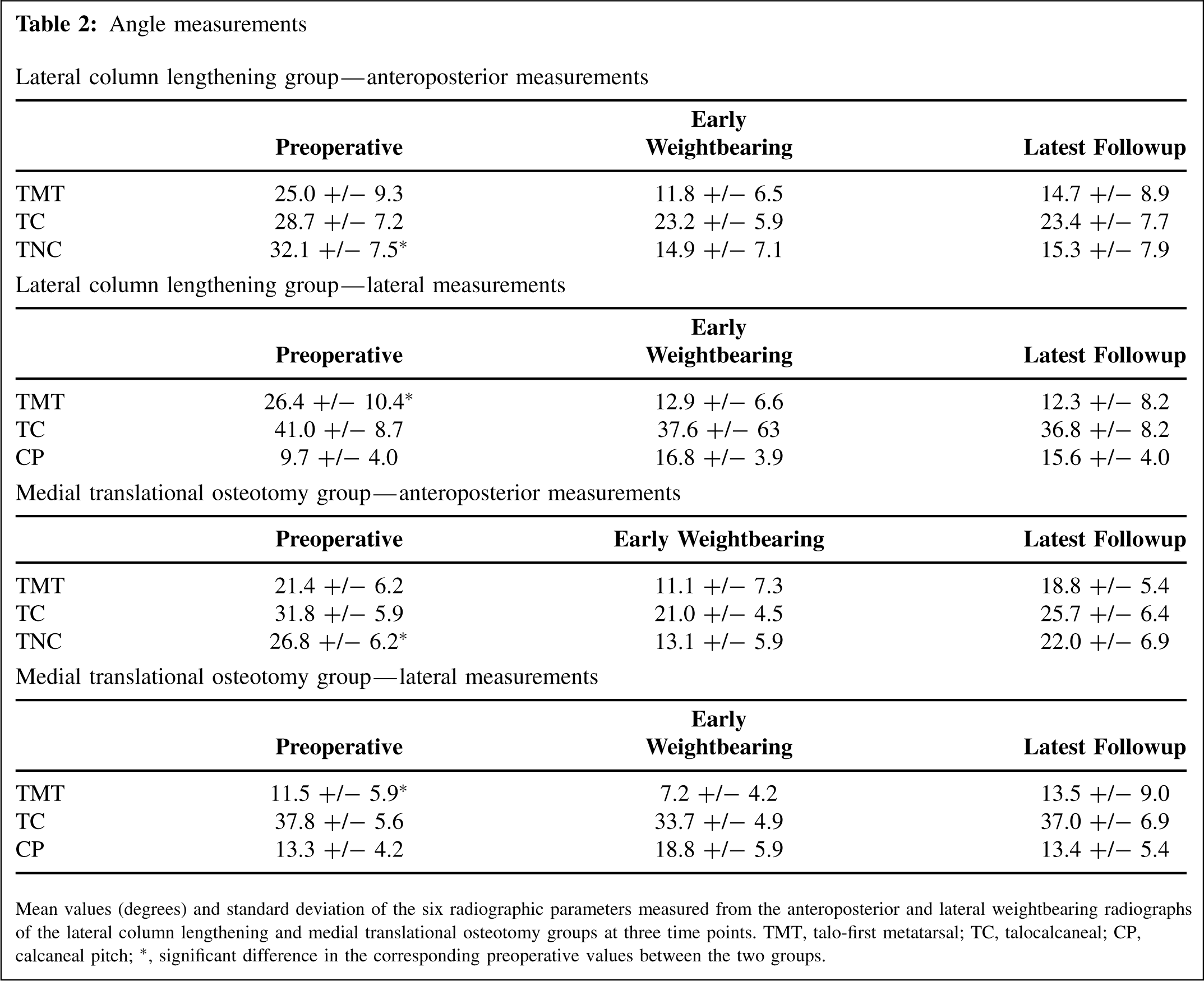
Mean values (degrees) and standard deviation of the six radiographic parameters measured from the anteroposterior and lateral weightbearing radiographs of the lateral column lengthening and medial translational osteotomy groups at three time points. TMT, talo-first metatarsal; TC, talocalcaneal; CP, calcaneal pitch;∗, significant difference in the corresponding preoperative values between the two groups.
Table 3 presents the results of the comparisons made on the radiographic measurements between the two groups. When the LCL and MTO groups were compared for change in each of the six parameters from their preoperative measurements to early weightbearing measurements (Initial Correction), the correction of the lateral TMT angle was significantly greater in LCL group than the MTO group (p = 0.002). When the groups were compared for change from their early weightbearing measurements to the measurements obtained at latest followup (change in correction), four of the six comparisons were significantly different. The TMT and TNC angles on the anteroposterior radiographs and the TMT and TC angles on the lateral radiographs were significantly different (p = 0.049, 0.01, and 0.03 respectively). When the groups were compared for change from the preoperative measurements to the measurements obtained at latest followup (final correction), four of the six comparisons were significantly different. The TMT and TNC angles on the anteroposterior radiographs and the TMT and CP angles on the lateral radiographs were significantly different (p = 0.04, 0.03, 0.0001, and 0.03 respectively).
Mean values (degrees) for the calculated changes over time of six radiographic parameters
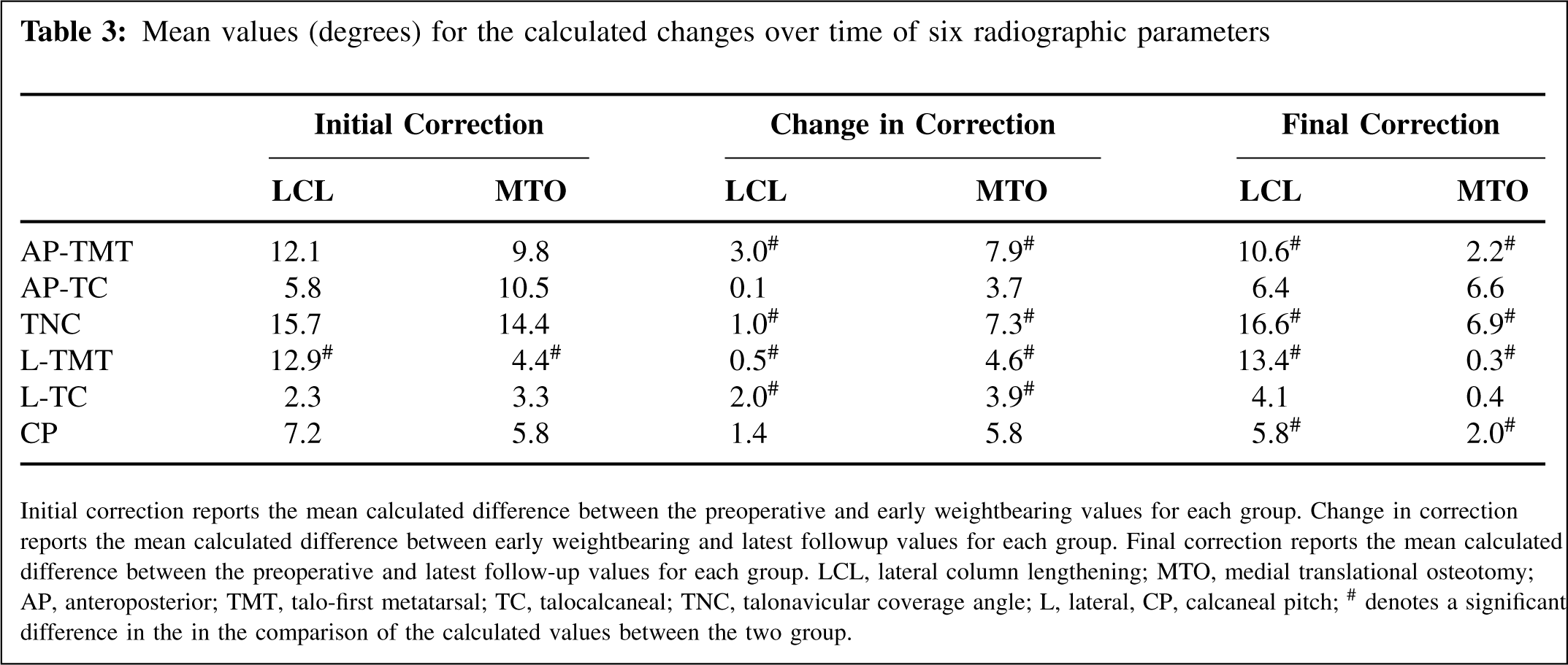
Initial correction reports the mean calculated difference between the preoperative and early weightbearing values for each group. Change in correction reports the mean calculated difference between early weightbearing and latest followup values for each group. Final correction reports the mean calculated difference between the preoperative and latest follow-up values for each group. LCL, lateral column lengthening; MTO, medial translational osteotomy; AP, anteroposterior; TMT, talo-first metatarsal; TC, talocalcaneal; TNC, talonavicular coverage angle; L, lateral, CP, calcaneal pitch;# denotes a significant difference in the in the comparison of the calculated values between the two group.
Degenerative changes in the hindfoot were observed in both groups. Eight joints in four patients from the MTO group exhibited changes in the appearance of the hindfoot joints. Four subtalar joints in four different patients progressed from a grade of 2 to 3 because of an increase in the size of a periarticular osteophyte. Two talonavicular joints in a patient who had staged, bilateral reconstructions progressed from a grade of 2 to 3 because of enlargement of an osteophyte. Two talonavicular joints progressed from a grade of 1 to 2 because a minute osteophyte developed. Fourteen hindfoot joints in nine patients from the LCL group demonstrated arthritic changes. Eight subtalar joints in seven patients showed degeneration over time. Two joints progressed from grade 1 to 2, four joints progressed from grade 2 to 3, and two joints progressed from grade 3 to 4. One of the patients who had narrowing of the joint space had staged, bilateral reconstructions. Six talonavicular joints in six patients exhibited changes. Two joints progressed from grade 1 to 2 and four joints progressed from grade 2 to 3. Five of the 14 joints that degenerated radiographically occurred in three patients with nonunions after LCL.
DISCUSSION
The results of this investigation indicate that a difference exists between these two hindfoot procedures in their capacity to realign a flexible adult acquired flatfoot deformity. The initial correction of the lateral TMT angle achieved with LCL was nearly three-fold greater than the correction obtained with MTO of the calcaneus. Since both groups received a plantar translational arthrodesis of the first tarsometatarsal joint to treat forefoot varus, the effect of either hindfoot procedure on the lateral TMT predominantly occurred at the talonavicular joint. From these results, we concluded that reconstruction LCL provides more correction of the longitudinal arch at the midfoot and overall realignment of the medial column of the foot than a reconstruction with MTO.
The results of this investigation further indicate that these procedures also differ in their capacities to maintain the initial realignment achieved after reconstruction over time. The measurements of four of the six radiographic parameters in the MTO group significantly changed between early weightbearing and latest followup when compared to the LCL group. The changes observed in the anteroposterior TMT, TNC, lateral TMT and lateral TC angles indicate that the reconstructions performed with MTO lost significantly more initial correction than feet reconstructed with an LCL as the patients returned to their activities after surgery. Furthermore, the LCL group demonstrated a significant change compared to the MTO group in four of the six parameters from the preoperative measurements and those obtained at latest followup. This result establishes that the final correction achieved in the LCL group was significantly greater than the one achieved in the MTO group. These findings support the conclusion that reconstructions with LCL lose less of their initial correction and maintain a better correction over time than reconstructions with MTO of the calcaneus.
Inspection of the subtalar and talonavicular joints revealed a higher incidence of degenerative changes in the LCL group. More than twice the number of joints demonstrated degenerative changes in the LCL group compared to the MTO group. Two subtalar joints in the LCL group displayed narrowing of the joint space, progressing from grade 3 to 4 over the course of the investigation. These changes are of concern because they represent a change from minimal to moderate arthritis. However, the cause of these changes observed in the LCL group is not completely known. The LCL group had a greater magnitude of preoperative deformity and a longer duration of postoperative followup. These factors, acting independently or in concert with the decision to use an arthrodesis instead of an osteotomy to reconstruct the flatfoot, may have had a deleterious effect on the remaining joints of the hindfoot.
In this study, patients who had MTO had additional procedures more often than those patients who had LCL. Painful hardware was the predominant indication for additional surgery in both groups. The rate of hardware removal for the MTO group was more than twice that of the LCL group. The rate of nonunion in the LCL group was double the rate in the MTO group. Although the difference in the number of feet requiring additional surgery between the groups was only one, the overall rate of reoperation for problems directly attributable to the hindfoot procedure for the MTO group was nearly twice the rate of the LCL group. Based on these results, we concluded that additional surgery is more likely necessary after MTO from painful hardware; however, the additional surgeries required after reconstruction with LCL are likely to be more invasive because of painful nonunions of the calcaneocuboid distraction-arthrodesis.
The results of this investigation may add to our current knowledge regarding the action by which these two hindfoot procedures realign a flexible flatfoot and maintain correction. In his initial report on flatfoot reconstructions with a medial displacement of the calcaneal tuberosity, Myerson et al. 20 described this procedure as a transfer of the gastrocnemius-soleus complex to produce a more mechanically balanced foot. The osteotomy was intended to reduce the valgus moment of this muscle group acting on the subtalar joint and its antagonistic force on a transferred flexor digitorum longus substituting for a dysfunctional posterior tibial tendon, spring ligament, deltoid ligament, and talonavicular joint capsule. 5,16 Although, he did not observe deterioration in the initial correction, he acknowledged that the longevity of these improvements was unknown. A subsequent study in a larger series of his patients reconstructed for stage II posterior tendon deficiency revealed that 17 of 129 patients lost correction at final followup. 19 In contrast, LCL realigns a flatfoot through biplanar rotation of the talonavicular joint and inversion of the calcaneus through the subtalar joint. 24 CT with simulated weightbearing has demonstrated that subluxation of all three facets of the talocalcaneal joint occurs in patients with flatfeet. DuMontier et al., 6 in a cadaver model, showed that LCL corrects flatfoot by plantarflexion and adduction of the midfoot and forefoot relative to the hindfoot. In our study, the radiographic changes observed in the LCL group agree with this cadaver study. Our results suggest that the effect of LCL on the bony relationships in the foot is more extensive and more durable than transferring the triceps surae through MTO. The greater change observed with the initial correction in the LCL group and the absence of its deterioration back to the preoperative deformity, as seen in the MTO group, may be a result of improved reduction of the subluxated subtalar joint and substitution of the attenuated capsuloligamentous structures surrounding the talonavicular joint.
Several limitations are inherent to the design of this investigation and should be considered during the interpretation of the data. The results of this study were derived from a consecutive series of patients treated by a single surgeon and, therefore, they may not be applicable to all patients undergoing reconstruction for adult acquired flatfoot deformity. Without randomization of the patients, bias in the selection process may be present. Although the choice of hindfoot procedure lacked randomization, it was consistent during the period of time that each patient received a reconstruction. This choice was not biased overtly by anything other than the surgeon's preference at the time of surgery. The absence of a significant difference in the AOFAS scores between the groups would suggest that they had a similar amount of pain and incapacity performing activities of daily living due to their flatfoot before their reconstructions. Also, the temporal dichotomy associated with the distribution of the patients contributed to a difference in the number of patients and the duration of postoperative followup in each group, it is unlikely to have had affected the results of radiographic evaluation or the rate of nonunion and additional surgery. In fact, the longer followup associated with the LCL group strengthens the conclusion that this procedure preserves the initial correction over time better than a calcaneal osteotomy. Finally, the conclusions are based on the results of radiographic analysis and chart review only. This study did not correlate these objective findings with patient-assessed measures of outcome. Although the use of functional measures of outcome and a determination of the rate of patient-assessed satisfaction may have provided additional information and enhanced the interpretation of the objective findings, the proscriptions of the institutional approval to proceed with this retrospective investigation precluded the prospective acquisition of such data.
In summary, reconstructions performed with LCL produced a greater change in the realignment of a flexible flatfoot, maintained more of their initial correction over time, and were associated with a lower incidence of additional surgery than reconstructions with a MTO of the calcaneus. Furthermore, the LCL group demonstrated these superior results despite possessing more preoperative pedal malalignment than the MTO group. However, a higher incidence of degenerative change in the hindfoot was observed in the LCL group. Although this finding is of concern, it is unknown whether it was a consequence of the severity of the preoperative adult acquired flatfoot deformity, the procedure used to correct the deformity, or a combination of these or other factors. The results of this study may prove beneficial in the preoperative decision-making process and the postoperative course. Subsequent investigations of these two procedures using a prospective, randomized, multi-center methodology are warranted to further examine the respective roles of LCL and MTO of the calcaneus in the operative management of adult acquired flatfoot deformity.