
Abstract

INTRODUCTION
Avulsion fractures of the calcaneal tuberosity are uncommon injuries. A recent study of fracture epidemiology has shown that calcaneal fractures account for 1.2% of all fractures 4 and studies of calcaneal fractures have shown that avulsion fractures of the calcaneal tuberosity comprise only 1.3% to 2.7% of calcaneal fractures. 4,12,17 It is therefore understandable that little has been written about these fractures.
Two types of avulsion fracture have been described. Rothberg 11 described a true avulsion fracture (Figure 1) in a 60-year-old female and this fracture type has since been documented by a number of authors. 7,10 The ‘beak’ type of avulsion fracture (Figure 2) has also been documented by a number of authors over the last 60 years. 3,15,16,18,19 These fractures were initially thought not to involve the tendoachilles insertion but Sutro, 16 Lowy, 7 and Prothero 10 questioned this and demonstrated that the ‘beak’ fracture was also an avulsion fracture. A recent report describing 24 calcaneal tuberosity fractures found only three avulsion type fractures in their series. The representative image in the article was a ‘beak’ type fracture. 15 We have encountered both types of avulsion fracture but we have also seen a third type of calcaneal tuberosity fracture which has not previously been described.

An avulsion or ‘sleeve’ type tuberosity fracture.
A ‘beak’ type of tuberosity fracture.
CASE REPORT
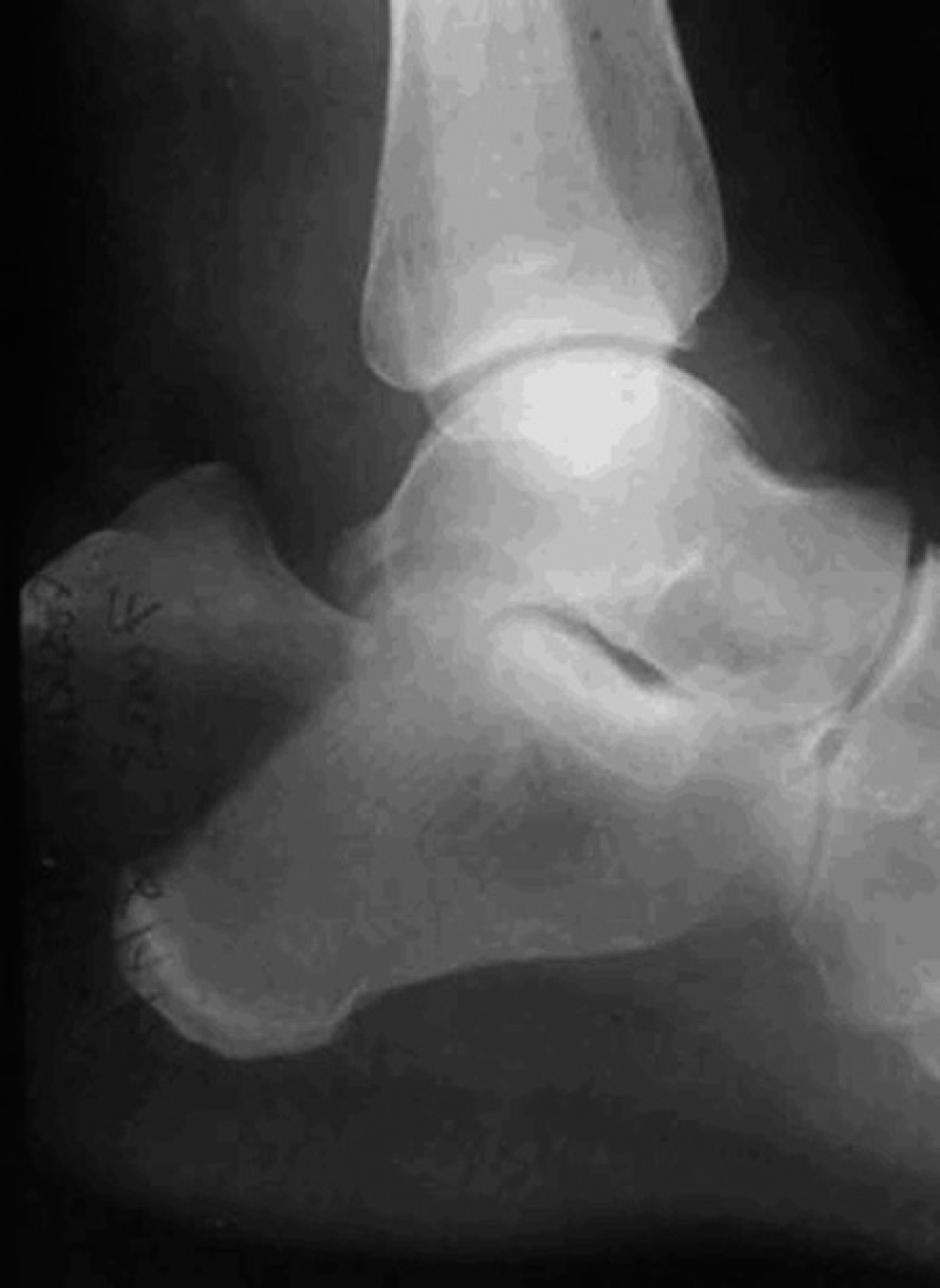
The fracture shown in Figure 3A occurred in a 57-year-old female who fell while running. She presented with a painful right foot and an inability to weight-bear or plantarflex her foot. X-rays showed avulsion of bone from the middle third of the posterior tuberosity of the calcaneus (Figure 3A). Ultrasound showed that the tendoachilles had been avulsed from its insertion and this was confirmed at surgery. Intraoperatively, it was found that the proximal portion of the calcaneal tuberosity was intact confirming an isolated insertion of the tendoachilles into the middle third of the calcaneal tuberosity in this patient. The tendoachilles was reattached using a suture anchor (Figure 3B). The patient was kept in a semi-equinus cast below-knee cast for 4 weeks and a plantigrade below-knee cast for a further 4 weeks. She was permitted to fully bear weight after 10 weeks and was referred for physiotherapy. She made a good recovery resuming normal function with no pain after 6 months.

An infra-bursal avulsion tuberosity fracture.
Anatomy and Pathogenesis
All of the major anatomy textbooks document that the tendoachilles inserts into the middle third of the posterior tuberosity of the calcaneus and that there is a bursa between the tendon and the upper third of the posterior tuberosity 1,6 (Figure 4A). This has recently been confirmed in an anatomical study of the insertion of the tendoachilles in man which has shown that when force is transmitted to the bone from a loaded tendon it is directed towards the plantar fascia by a series of highly orientated trabeculae. 9
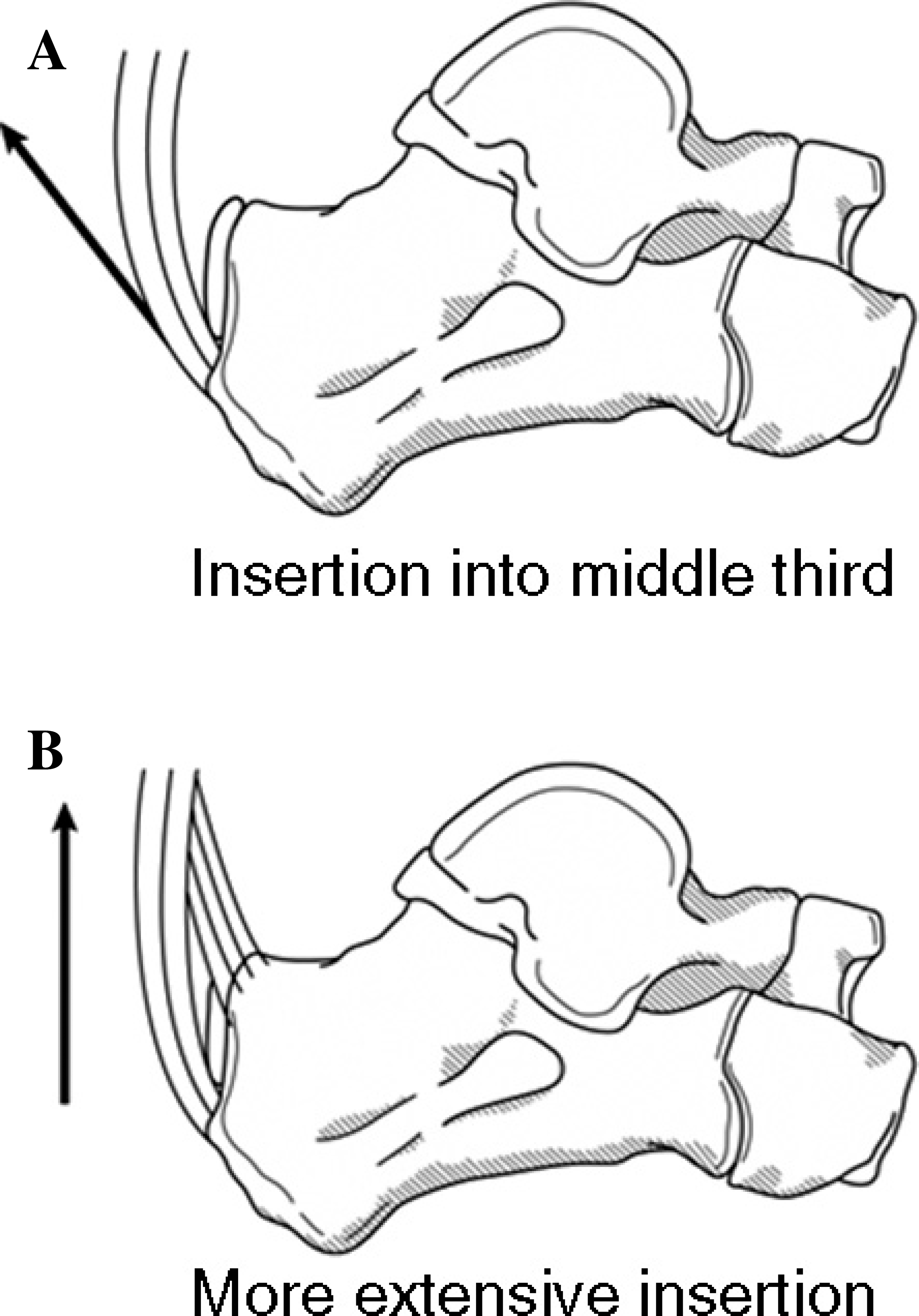
It would seem from a review of the orthopaedic literature that some individuals have a more extensive insertion of the tendoachilles into the calcaneus (Figure 4B). This has been confirmed surgically 7,10,16 with Lowy 7 showing that in ten dissected specimens two had higher than normal tendoachilles insertions.
The literature also suggests that avulsion fractures of the calcaneal tuberosity are osteopenic or osteoporotic in origin. 15,20 In the nine cases documented by Lowy 7 and Prothero 10 the average age was 62 (range, 39 to 77) years. All the cases of tuberosity avulsion fractures described by Squires were over age 75. 15 These fractures have also been shown to occur in diabetics in whom they are insufficiency fractures associated with a peripheral neuropathy. 2,5
Classification
We propose a classification incorporating the three types of calcaneal tuberosity avulsion fractures (Figure 5). A Type I fracture is a ‘sleeve’ fracture in which shell of cortical bone is avulsed from the posterior tuberosity (Figure 1). Type II fractures are the classical ‘beak’ fracture in which there is an oblique fracture line running posteriorly from just behind Bohler's angle (Figure 2) and the Type III fracture is the infrabursal avulsion fracture from the middle third of the posterior tuberosity which has not been previously described (Figure 3). All occur in osteopenic or osteoporotic bone but we believe it likely that the Type I ‘sleeve’ fracture probably occurs in older patients with significant osteoporosis.
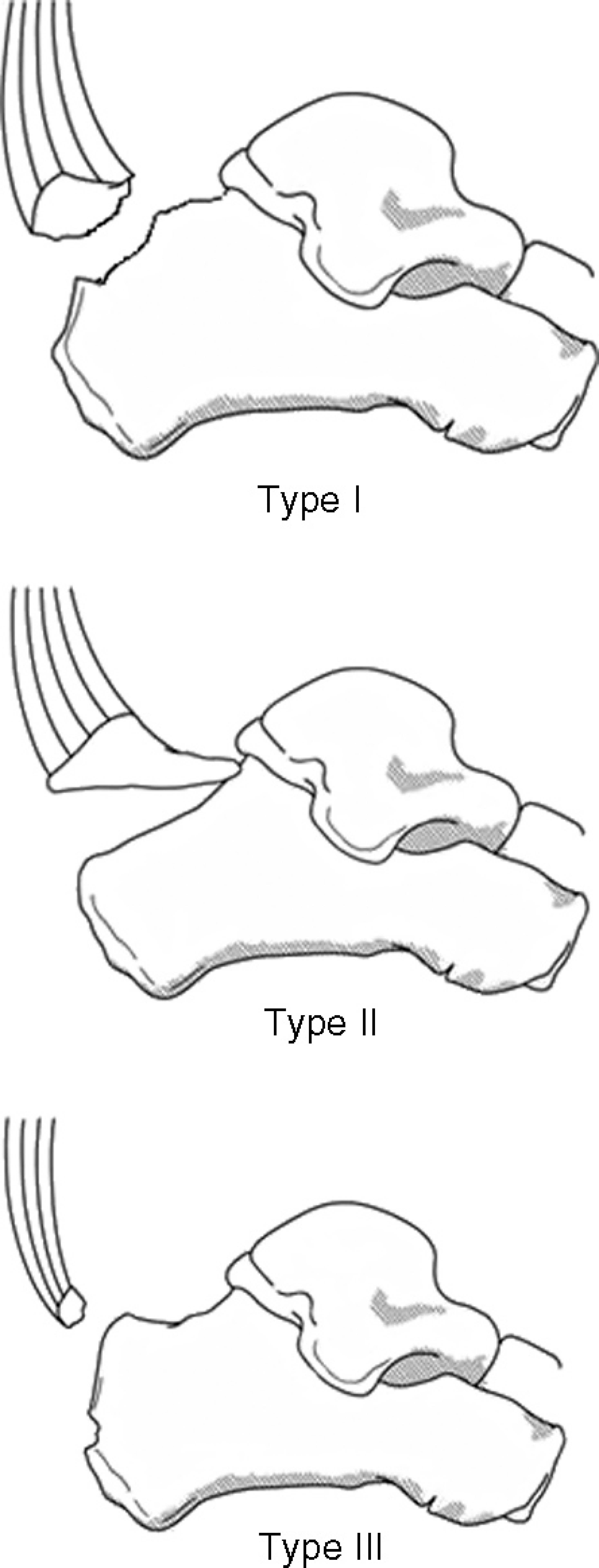
Classification of tuberosity fractures: Type I - The ‘sleeve’ fracture. Type II - The ‘beak’ fracture. Type III - The infrabursal fracture.
DISCUSSION
Given the published anatomy of the insertion of the tendoachilles into the posterior calcaneus it is surprising that the Type III avulsion fracture has not previously been described. Indeed if the anatomy textbooks were correct it should be the only possible type of avulsion fracture. It has been shown that in a number of individuals there is a broader insertion of the tendoachilles into the calcaneus but although Lowy 7 demonstrated this in two of ten dissected specimens the true prevalence of this anatomical variant is unknown. It would seem however logical to suggest that individuals who have this type of insertion are at greater risk of an avulsion fractures as only Type I and II fractures have been previously described. It may be that the more direct pull provided by the broader insertion of the tendoachilles in these individuals (Figure 4B) increases the risk of avulsion fractures. We believe that this is likely the case as it would account for the discrepancy between the anatomy of the area and the prevalence of Type I and II fractures.
Snow et al. demonstrated that with age the continuity between the Achilles tendon and plantar fascia diminishes. 14 Neonates have a thick, continuous sheet of fibers connecting the two structures which is gradually lost with age. The elderly foot demonstrates only a zone of periosteum on the postero-inferior calcaneus between the Achilles insertion and plantar fascia attachment. The suggestion that the Achilles insertion may in fact be receding offers some explanation for the variable point of attachment described by different authors. Furthermore, calcification of the retrocalcaneal bursa adjacent to the insertion could alter the actual zone of tendon attachment. 13
We believe that age-related changes of the tendoachilles insertion, combined with diminished bone density, explain why avulsion fractures of the calcaneal tuberosity occur with increased age. The balance between these two factors may determine which type of fracture will occur. We have seen a case of Type I fracture in a younger patient however, the majority of cases occur in the elderly with poor bone quality. Type I and II fractures can only occur in patients with a more proximal insertion. The Type III fracture described above occurred in a patient with a tendoachilles insertion into the middle third of the calcaneal tuberosity.
The recommended management of all displaced calcaneal tuberosity fractures is accurate reduction and stabilization to allow restoration of the Achilles tendon insertion as well as minimize deformity. 7,10,15 Complications after non-operative treatment of displaced calcaneal tuberosity fractures include: skin necrosis, Haglund's deformity and loss of plantarflexion strength. 7,10
Implant options include screw fixation, tension band wiring or by suturing the avulsed bone fragment to the calcaneus. 7,10,15 Suture anchors have previously been used successfully in this area. 8 The choice of technique depends on the size of the avulsed bone fragment and the degree of osteopenia. Type I fractures typically have limited available bone stock and if screw fixation is not possible, tension band wiring or suture anchors can be used. Type II fractures should have adequate bone to accommodate interfragmentary screw fixation. Type III fractures should be treated by suturing the tendon to the calcaneus. Identification of the fracture type preoperatively will facilitate preoperative planning to ensure that the appropriate implants are available.
CONCLUSION
We believe that it is important to appreciate the different types of calcaneal tuberosity avulsion fracture in order to plan surgical treatment. All three types are osteopenic or osteoporotic and may be associated with diabetes occurring late in the condition when a neuropathy is present. With an increasingly elderly population osteoporotic fractures are increasing in incidence as are the numbers of patients presenting with the late manifestations of diabetes. It is therefore likely that these fractures will be more commonly seen in the future.