
Abstract

Introduction
Total talar extrusion with no remaining soft tissue attachments is an extremely rare injury that may occur as a result of a high-energy extreme supination and plantar flexion forces causing an anterolateral dislocation. 1,2 Due to the extreme rarity of such cases, few reports can be found in literature and the ideal treatment has not been determined. 1–4,6,7,11
Immediate replacement has been described; however, the disruption of all sources of its blood supply would almost always doom the talus to irreversible avascular necrosis and concomitant clinical disability. 6 The risk of devastating infection following reimplantation into the open, debrided wound should also be considered. 7
Tibiocalcaneal fusion has been advocated for symptomatic avascular necrosis of the talus after fracture dislocation injuries and, furthermore, as an appropriate surgery for total talar extrusion. 3 However, significant disadvantages of tibiocalcaneal fusion include loss of function, deformity of the hind part of the foot, and shortening of the involved limb, as well as the technical difficulty of the procedure. 10
Recently, the repair of large bone defects using a prosthesis or hydroxyapatite bone substitutes combined with mesenchymal stem cells has becoming increasingly popular. 8,9,13 Bone and bone marrow are anatomically contiguous and functionally interdependent. 14 Bone marrow is composed of haematopoietic and non-haematopoietic stem cells from which different cell types originate, such as osteoblasts, osteoclasts, endothelial, and fibroblastic cells. 12 In addition, haematopoietic cells, such as lymphocytes and megakaryocytes, contribute to the regulation of bone remodeling.
We report the only case, to our knowledge, in which a totally extruded talus with no remaining soft tissue connection was re-implanted four months after trauma, with the addition of autologous bone marrow mononuclear cells to repopulate the implant with haematopoietic and mesenchymal precursor cells.
Case Report
In May 2000, a 30-year-old woman was involved in a motor vehicle accident, sustaining a fracture of L2, a fracture of her left tibia and fibula, and a total extrusion of the talus through a 10-cm wound along the anterolateral aspect of her right ankle (Figure 1, A and B). The talus was found a few meters from the patient and placed in saline while she was transferred to a trauma ward where she received first aid.
Surgical stabilization of the vertebral column was performed first. The neurological status of the lower extremities was completely intact and no major vascular lesions were reported. Irrigation and debridement of the ankle wound was performed and an antibiotic-impregnated polymethylmethacrylate spacer was inserted in the talar place, in order to maintain the length and shape of the limb. An external fixator (Orthofix, Bussolongo, Italy) was then placed across the ankle joint (Figure 2). The tibio-fibular fracture in the left limb was also treated with external fixation. The expulsed talus was examined and found to be intact; it was sent to a bone bank for freezing.
Four months passed before the general condition of the patient permitted her to be referred to our institution. Treatment options were discussed with the patient. Because the frozen talus was still available, re-implantation with the addition of bone marrow mononuclear cells (BMMCs) was chosen. The technique for preparing the BMMCs is available in an online addendum to this article.
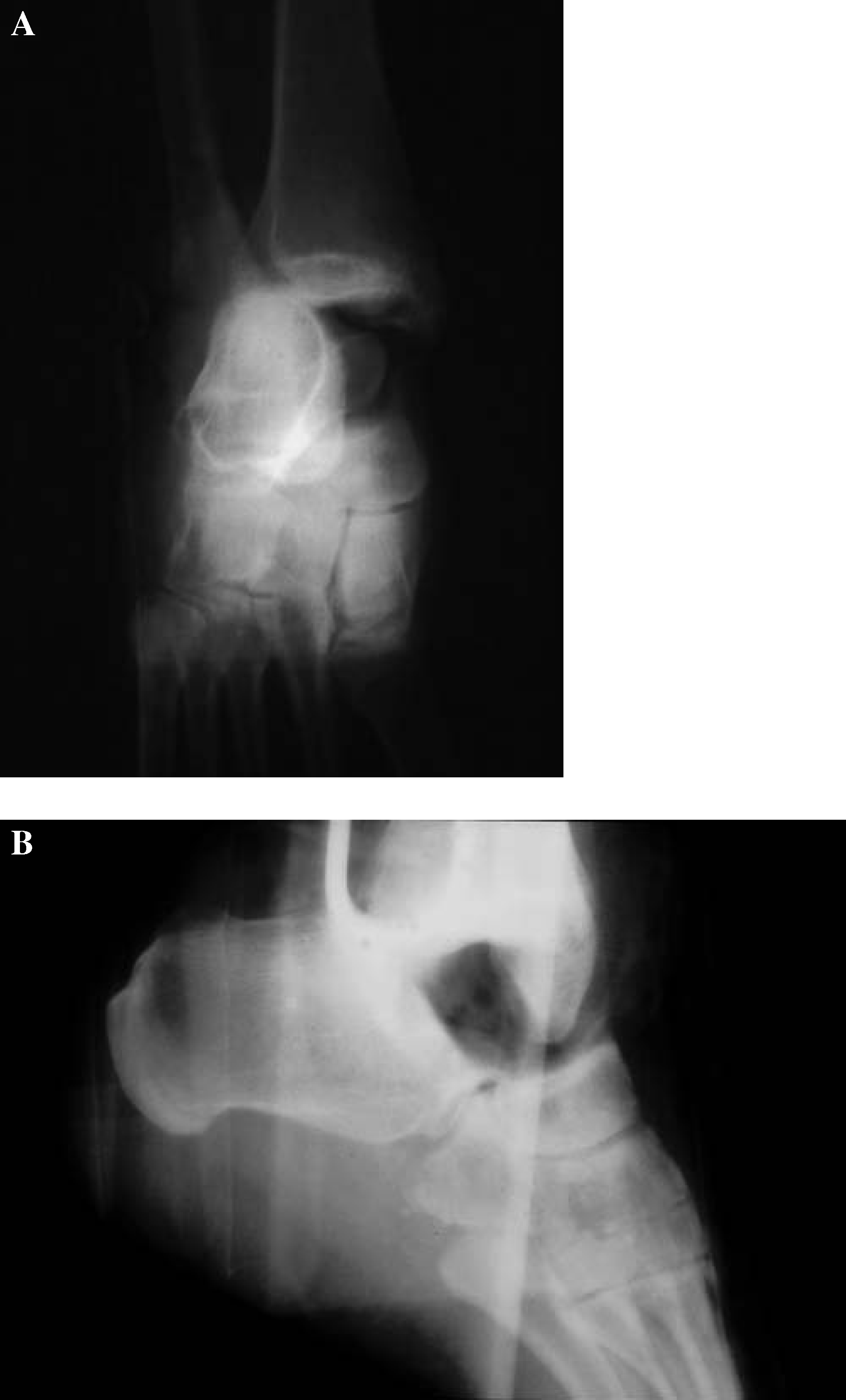
Anteroposterior (A) and lateral (B) view of the ankle demonstrating the absence of the talus.
Surgical Technique
Under general anaesthesia, the patient was placed in the supine position and a tourniquet was applied to the thigh of her right limb. The external fixator was removed and an anterior approach to the ankle was performed. The cement spacer, which matched the talus, was removed. Finally, the engineered talus was placed (Figure 4) and held with a screw inserted from the neck of the talus to the calcaneus (Figure 5, A & B). A drain was applied and standard closure was performed. A boot was worn after surgery and daily passive ROM was permitted four days after surgery. Intravenous antibiotics were administered preoperatively and continued for 5 days. Clinical and radiographic followup was performed monthly during the first 3 months; clinical, radiographic, and MRI followup was then performed at 4, 6, 8, 12, 24, 36 months and at 5 years followup.

Demonstration the antibiotic-impregnated polymethylmethacrylate spacer inserted into the ankle joint and stabilization with the external fixator (Orthofix, Bussolengo, Italy).

Through an anterior approach to the ankle, the cement spacer was removed and the talus reimplanted.
Swimming and cycling with no weight bearing was allowed after four months. After seven months, the screw fixing the talus to the calcaneous was removed. Walking with partial weight bearing was permitted after four months. The patient progressed to full weightbearing one year post-operatively without the use of external support.
Results
No intraoperative or postoperative complications occurred. At the most recent followup evaluation (5 years and 10 months after the injury), the patient was very satisfied with the results obtained. She had no pain in the right ankle or foot when walking for hours, even on uneven terrain, and was able to resume her previous level of skiing and hiking. She required a 1.5-cm insole and wore comfortable shoes, although fashionable shoes could be worn occasionally.
The physical examination revealed normal alignment of the ankle with a plantigrade foot. The patient walked with a normal gait. The right limb was 1.5 cm shorter than the left. The ankle was stable with a range motion of about 30 degrees (Figure 6, A & B). Fifteen degrees of subtalar motion was also present.
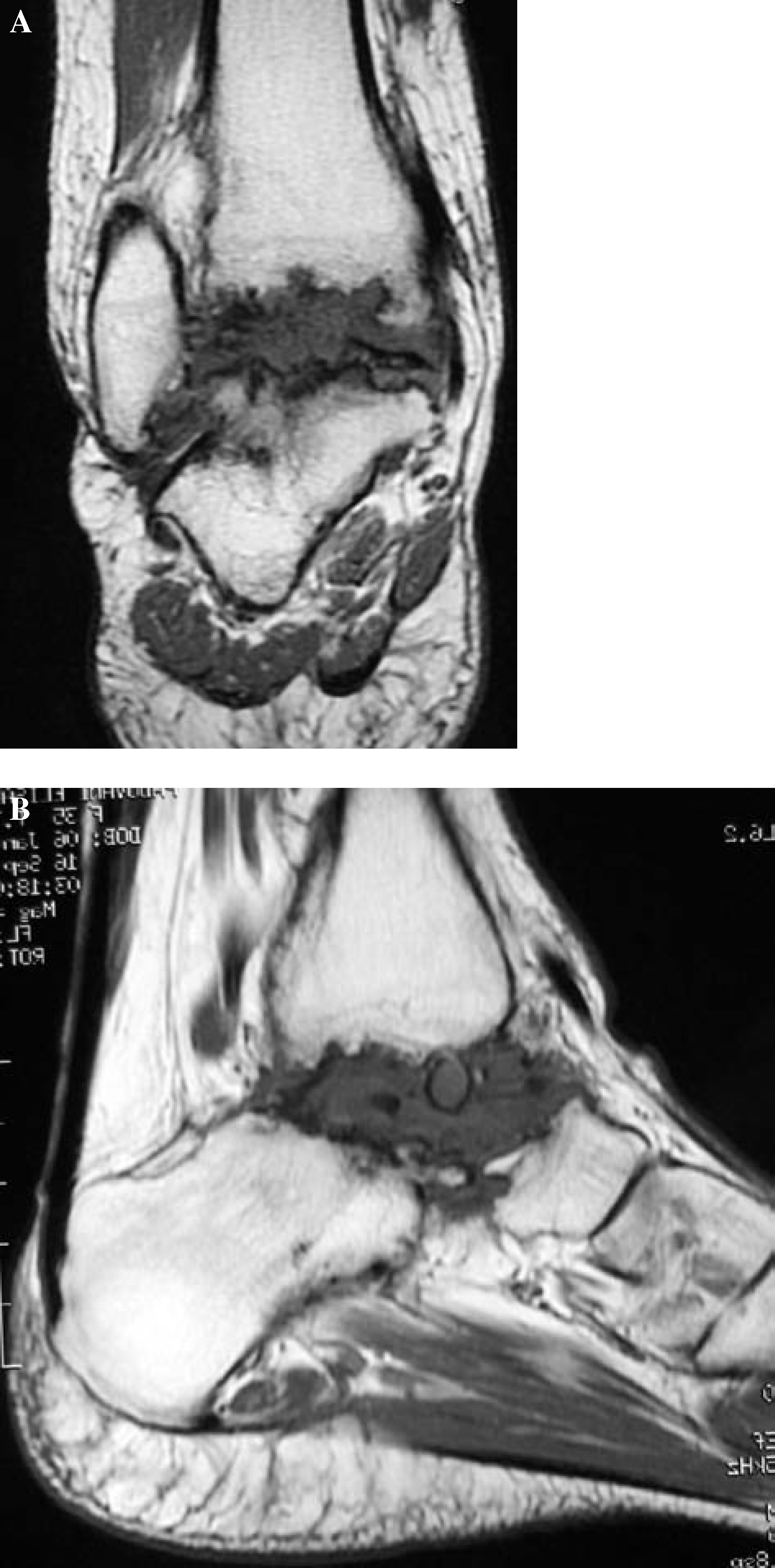
X-rays and MRI evaluation demonstrated a slow and progressive fragmentation and resorption of the engineered talus over time. At 5 years followup, the talus was seen to be completely replaced by a fibrous tissue maintaining 1.5 cm of distance between tibia and calcaneus (Figure 7, A & B).
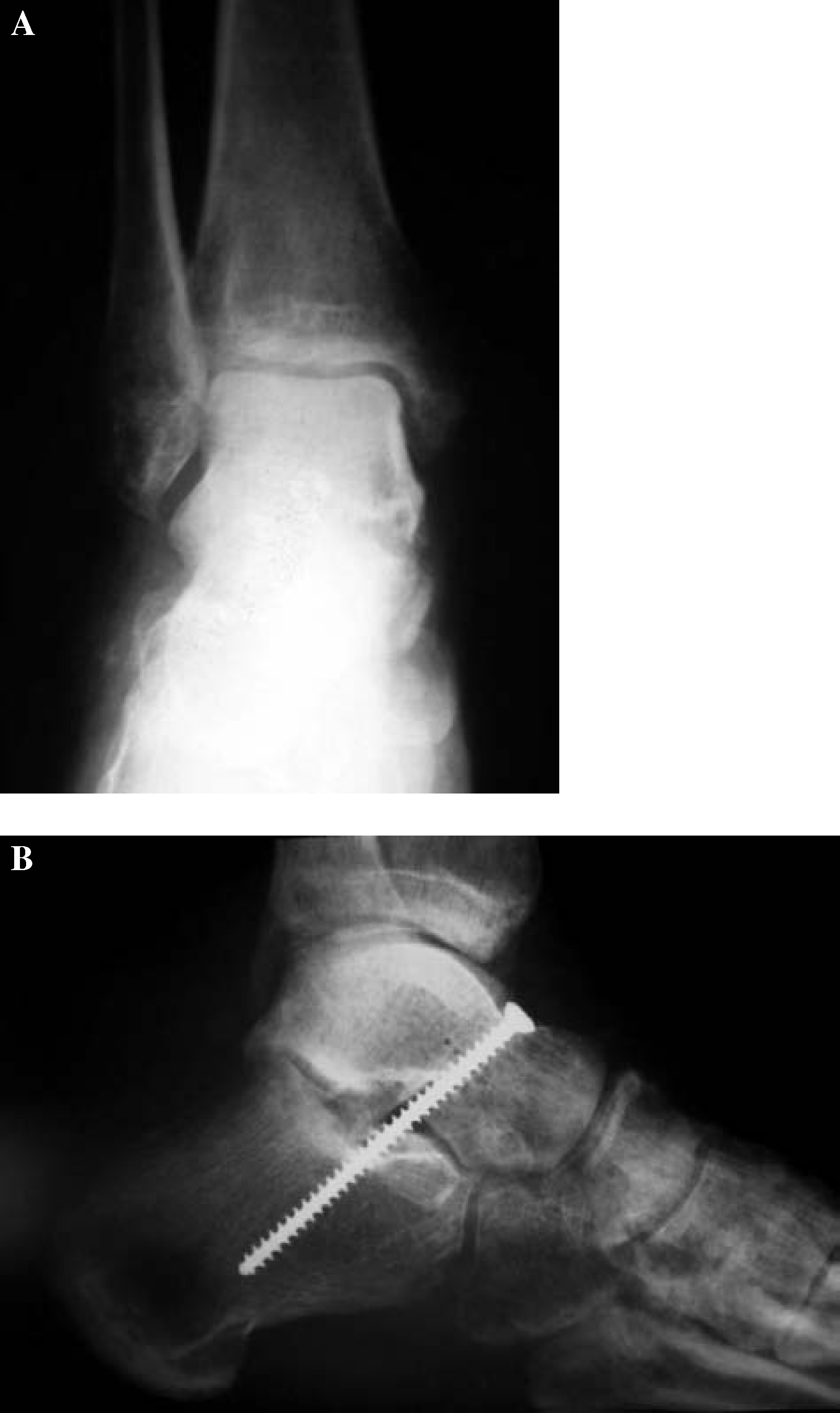
Stabilization of the re-implanted talus was obtained with a screw inserted from the neck of the talus to the calcaneus. Anteroposterior (A) and lateral (B) postoperative views.
Discussion
Due to the high rate of complications following talar extrusion, the usual treatment choice reported in the past has been an immediate tibiocalcaneal arthrodesis. 7 Yet, the results of the few cases of re-implantation reported in the literature are encouraging.
Brewster and Maffulli 2 reported two cases of total extrusion of the talus and immediate re-implantation in each case. In both cases, normal talar architecture and radiodensity were maintained two years post-operatively, but in one case, osteoarthritic changes of ankle and talonavicular joints developed. In another case presented by Assal and Stern, 1 at 5 years followup, the talus maintained normal bone density, but radiographic evidence of arthritis and anterior ankle impingement was present at 3 years.

In the case presented, the delay in re-insertion of the frozen talus occurred as that patient presented to us four months after her accident. It is obvious that chondrocyte viability of the re-implanted talus was compromised and the attempt at enhancing revascularization of the talus by using the BMMCs was not successful.
Although the radiographic results were disappointing demonstrating collapse of the re-implanted talus at 5-years followup, the clinical results were quite satisfying, possibly due to the progressive development of fibrous tissue acting as a spacer. We postulate the implantation of the BMMCs in the talus may have been helpful in the development of this mechanically strong fibrous tissue, since these cells represent a mixed population of haematopoietic and non-haematopoietic mesenchymal precursor cells.
Conclusion
Based on our clinical result, the authors feel that avascular necrosis of the talus does not necessarily lead to an unsatisfactory result and that re-implantation of an extruded talus, even after a time delay following freezing, may be considered a reasonable option. 4,11