
Abstract
Background: Osteoarthritis of the first metatarsophalangeal (MTP) joint is a painful, disabling condition. It can interfere with the ability to run and even walk without pain. An implant of cobalt-chrome steel alloy to replace the base of the proximal phalanx is one solution. The purpose of this study is to review our results with one of these implants. Materials and Methods: A series of 23 cases of hemiarthroplasty for the treatment of hallux rigidus from June 2000 to October 2001 has been evaluated using the AOFAS rating system, and the results are presented. Results: The average preoperative AOFAS score was 57 (range, 39 to 80). The AOFAS score after hemiarthroplasty was 88 (range, 75 to 100) at last followup (34 to 72 months). There were no perioperative complications except for a small hematoma. Only one patient has required further surgery after 3 years for worsening of a preexisting tendency to hallux valgus. Conclusion: A hemiarthroplasty retained, in most cases, joint mobility, strength, and alignment while relieving pain. There was no evidence, at last followup, of component loosening or osteolysis.
INTRODUCTION
Osteoarthritis of the first metatarsophalangeal (MTP) joint is a painful, and sometimes disabling, condition. It affects adult males and females in almost equal numbers mainly in the sixth and seventh decades of life, but may become noticeable in the fourth and fifth decades without obvious cause. Its origin may be preceded by a traumatic episode but is frequently bilateral and without a history of trauma. It may exist in the absence of degeneration in other synovial joints. In 1887, when the condition was first described by Lucy 34 and separately by Davies-Colley, 9 it concerned young men. It was given the name ‘Hallux Rigidus’ by Cotterill in 1888. 7
Little has been written on its incidence or its prevalence. In an analysis of 264 lateral foot x-rays, Grady 20 found hallux rigidus in 81, an incidence of 30%, but its degree of severity or clinical complaint was not noted. Weinfeld and Schon 49 describe it as “a common disorder” and list 439 cases treated by surgery. While it is most likely a universal complaint, papers on the subject listed in Medline are exclusively from North American and European sources.
The pathological evolution of hallux rigidus (HR) follows the same path as degenerative arthritis in other synovial joints. Loss of surface cartilage or subchondral osseous damage is followed by the formation of subchondral sclerosis and bone cyst formation. There is synovial inflammation and joint fluid increases. The capsule of the joint thickens, osteophytes form around the metatarsal head and phalanx, and the joint enlarges. The range of motion diminishes. Symptoms vary with the individual, the stage, and the severity of the joint disease. Pain on running curtails ‘jogging,’ and walking at a normal gait may be painful. Loss of motion at the first MTP joint leads to adaptive strategies. They include foot eversion by heel pivot, external rotation of the leg at the hip joint, reduced stride-length, and load transfer to the outer border of the foot.
There is no single cause for HR. While more common in older age, it may be present at any age after the third decade. Bilateral occurrence in the absence of other synovial joint involvement, may suggest an anatomical or structural abnormality. Lucy 34 and Davies-Colley 9 thought the condition resulted from stiff soles and too short boots. Camasta 6 cites pes planovalgus and “hallux equinus” with a shift in the axis of motion at the first MTP joint. Although elevation of the first MT has been suspected, Horton 24 found 8 mm of elevation of the first MT to be normal and even at that elevation, no difference between HR and controls. As with all degenerative joint disorders, trauma may play an initiating or continuing role in etiology. Stubbing the toe severely could be a contributing factor, but the literature does not note an increased incidence in professional soccer players, nor does it cite occurrence in the dominant “kicking” limb. Hallux rigidus may be a feature of some inherited forms of cartilage degeneration, which is believed to have a link to Bone Morphogenic Protein receptor signaling (BMPR 1a) reduction. 43 It can be found in other forms of arthropathies, such as rheumatoid arthritis, psoriatic arthropathy, gout, and hemochromatosis.
Treatment, when symptoms warrant, includes conservative and surgical options. Concern over available surgical options for the treatment of first MTP joint arthritis (including proximal phalangeal resection, soft tissue interposition, silastic hemiarthroplasty, and arthrodesis) has led to the development of a cobalt-chrome implant for resurfacing the proximal joint surface of the proximal phalanx.
This report will present and analyze the outcome from a clinical trial of 23 cobalt-chrome hemiarthroplasty implants in 19 patients, for whom standard conservative methods had failed. None of the patients had received a first MTP joint cortisone injection.
DESIGN PHILOSOPHY
The primary goal of resurfacing part of the metatarsophalangeal joint is to remove some or all of the pain arising from arthritis in the joint. The abrasion of cartilage creates microdebris from rough, irregular joint surfaces, which initiate an inflammatory response. Provision of a smooth, inert, bearing surface on one side of the joint should reduce shedding of cartilage debris. The geometry of the phalangeal joint surface is the most easily reproduced.
The secondary goal is to improve, if not fully restore, normal joint kinematics. This is achieved by correcting joint soft tissue contractures, removing marginal osteophytes, and replacing the damaged phalangeal surface with a precisely positioned, smooth, polished metal implant. The stability of the implant is increased and micromotion prevented by making its anchoring stem anatomically shaped to correspond with the endosteum of the phalangeal medullary canal. Roughening the stem surface improves adhesion to bone cement and it can be prepared for biological ingrowth. The bearing surface is angulated in relation to the stem to obtain correct alignment to the articulating surface of the metatarsal head. The bearing surface of the implant is the average reproduced surface geometry of the phalangeal proximal bearing surface as outlined below.
Instruments are designed to ensure precise removal of the minimum amount of the phalangeal base through the subchondral layer at an angle of 4 degrees in the coronal plane. Other instruments are designed precisely to prepare the endosteum of the phalanx to accept the implant stem with a matching shape.
The implant is made of quality wrought cobalt, chromium-28, and molybdenum-6 alloy as specified in ASTM-F 1537 (American Society for Testing Materials, Philadelphia, PA). Cobalt alloy is chosen for its wear properties and proven biocompatibility. 14 The instruments for osteotomy and medullary canal preparation are made of 17–4 PH stainless steel as specified in ASTM-F 899.
After establishing the general principles of design, a morphometric analysis 44 was performed on normal adult male and adult female cadaver feet to determine the following anatomical measurements:
The average length of the proximal phalanx;
The average width, medial and lateral, dorsal and plantar, of the phalanx at 3 positions: proximal maximum, distal maximum, and mid-length maximum;
The height and width of the proximal joint surface;
The interior dimensions and shape of the phalanx; and
The surface geometry of the phalanx.
The interior dimensions of the proximal half of the phalanx were determined from cross sections and CT scans. With the endosteum defining the limits, it is a symmetrical 3-sided pyramidal space with a larger dimension on the plantar surface. The geometric form is a trihedron. 44
The dimensions of the resulting implants (small, medium, and large) are the average of the morphometric dimensions with a reduction in the stem of the component by 1 mm to accommodate a layer of bone cement or a porous coating for bone ingrowth (Figures 1 and 2).

The Trihedron, cobalt-chrome implants in small, medium and large sizes. There is a 4-degree angle in the coronal plane between base and stem. The cemented version is shown.

The Trihedron implants bearing surfaces, small, medium and large.
The joint contact surface is a pre-determined standard thickness, equal to the normal cartilage thickness and the minimal subchondral layer excised. It has a polished surface contoured to correspond with the average natural joint radial curves of the phalangeal base. The surface contour of the base has a radius larger in the medial-lateral than that in the dorsal-plantar direction. Instruments have been manufactured to ensure precision proximal phalangeal subchondral osteotomy and removal of the medullary cancellous bone from the proximal half of the phalanx. An osteotomy guide allows removal by oscillating saw of the minimal amount of subchondral bone from the phalanx at a precise angle of 4 degrees in the coronal plane, in keeping with the morphometric findings and to ensure anatomic compliance. Templates have been designed to mark the outline of the medullary bone to be removed to accommodate the component stem in the correct rotational orientation.
SURGICAL PROCEDURE
The skin is prepared with antiseptic and the whole foot is enclosed in a transparent sheet of adherent plastic to exclude from the operation site all toes and the distal part of the great toe.
After a dorsal skin incision over the MTP joint medial to, but parallel with, the extensor hallucis longus tendon, the periosteum and capsule of the joint are incised in the same line. Osteophytes are removed from the distal metatarsal and proximal phalanx. The raw bone area on the metatarsal neck is filed to leave a smooth surface. Bone wax is applied to minimize blood accumulation and tissue adhesion. A guided 1/8-inch diameter (3.175 mm) drill is passed into the medullary canal through the center of the phalangeal base joint surface to just beyond the midpoint of the shaft. The osteotomy guide tool rod is inserted to orient the osteotomy cut. The proximal surface of the phalanx is removed by using the guided blade of an oscillating saw and any edge osteophytes remaining are trimmed. The line of cut is a predetermined distance from the joint surface in the subchondral bone. The proximal medullary cancellous bone is removed to the endosteum using trihedron shaped rasps of small, medium and large dimensions. Bone removal is facilitated by initial use of a powered side-cutting burr.
A trial plastic implant is placed in position to assess proper tissue tensioning around the joint before the cobalt-chrome implant is inserted. A small amount of antibiotic containing PMMA cement provides adequate fixation. A porous coated implant can be press-fitted after the same preparation. The capsule is sutured and the skin is closed with a totally buried absorbable suture. Five 10-ml 0.5% plain long-acting local anesthetic are injected around the operation site to reduce postoperative pain. An intravenous bolus of antibiotic is given 1 hour before surgery and 3 postoperative doses are given orally at 8-hour intervals. A simple bandage is used for support. Weightbearing with crutches is allowed immediately.
MATERIALS AND METHODS
Permission to conduct this clinical trial was obtained from the Health Sciences and Affiliated Teaching Hospitals Research Ethics Board and from the Therapeutics Products Program of the Medical Devices Bureau. All patients enrolled in this series signed consent forms acceptable to the Research Ethics Board.
The clinical trial began on June 13, 2000. The last implant in the series was inserted on October 2, 2001. The AOFAS scale 27 was applied prior to surgery and at the time of followup. The pre-surgical scores were compared with the post-surgical scores using the paired sample t-test. All patients in this group fell within most of the seven categories of the Regnauld Third Degree classification of severity 39 listed by Grady et al. 20
Cemented hemiarthroplasty was performed on 19 patients, nine of whom were male. The patients' ages ranged from males 41 to 61 (average age, 51.6) years and females 35 to 70 (average age, 54) years. There were 14 right feet and 9 left feet, with 4 patients having, at the same time, bilateral procedures, making a total of 23. Followup visits for clinical examination were performed at 2 weeks, 6 weeks, 6 months, and yearly thereafter when possible. Clinical examination included the state of the wound, assessment of pain, joint motion, joint stability, extensor and flexor strength, mode of walking, foot and leg gait orientation, and x-ray. The ability of the patient to return to normal walking pressure between the great toe pad and the ground was also noted but not measured by pedobarography. Patient satisfaction was gauged and return to work recorded.
RESULTS
The first MTP joints were affected in six patients as part of generalized osteoarthritis of the Kellgren and Moore type, 26 most visible as Heberden's nodes 23 on the fingers.
One patient had hemochromatosis with multiple joint OA. One patient had post-traumatic OA and poorly controlled gout. Five patients had one and 6 patients had both first MTP joints affected by osteoarthritis with no other joints involved. Among them was a patient with congenital joint hypermobility.
There were no wound infections but one patient had a small hematoma that spontaneously resolved.
The followup time from the day of surgery averaged 68 (range, 34 to 72) months. The preoperative AOFAS score average was 56.8 points (range, 39 to 80).
At the last followup, it averaged 88.2 (range, 75 to 100). The average gain in the AOFAS score was 31.4 points. The patient with least improvement moved from 42 to 75 points and the patient with the greatest improvement moved from 44 to 100 points. Table 1 contains the results of the pre- and postsurgical significance testing for the AOFAS. The changes were highly statistically significant for pain (p < 0.001), activity (p < 0.001), footware (p < 0.022), motion (p < 0.001), and summary score (p < 0.001). The other four components of the scale were already at their maximum value at the time of the presurgical assessment and did not change.
Mean baseline and last followup scores for the AOFAS (n = 23)
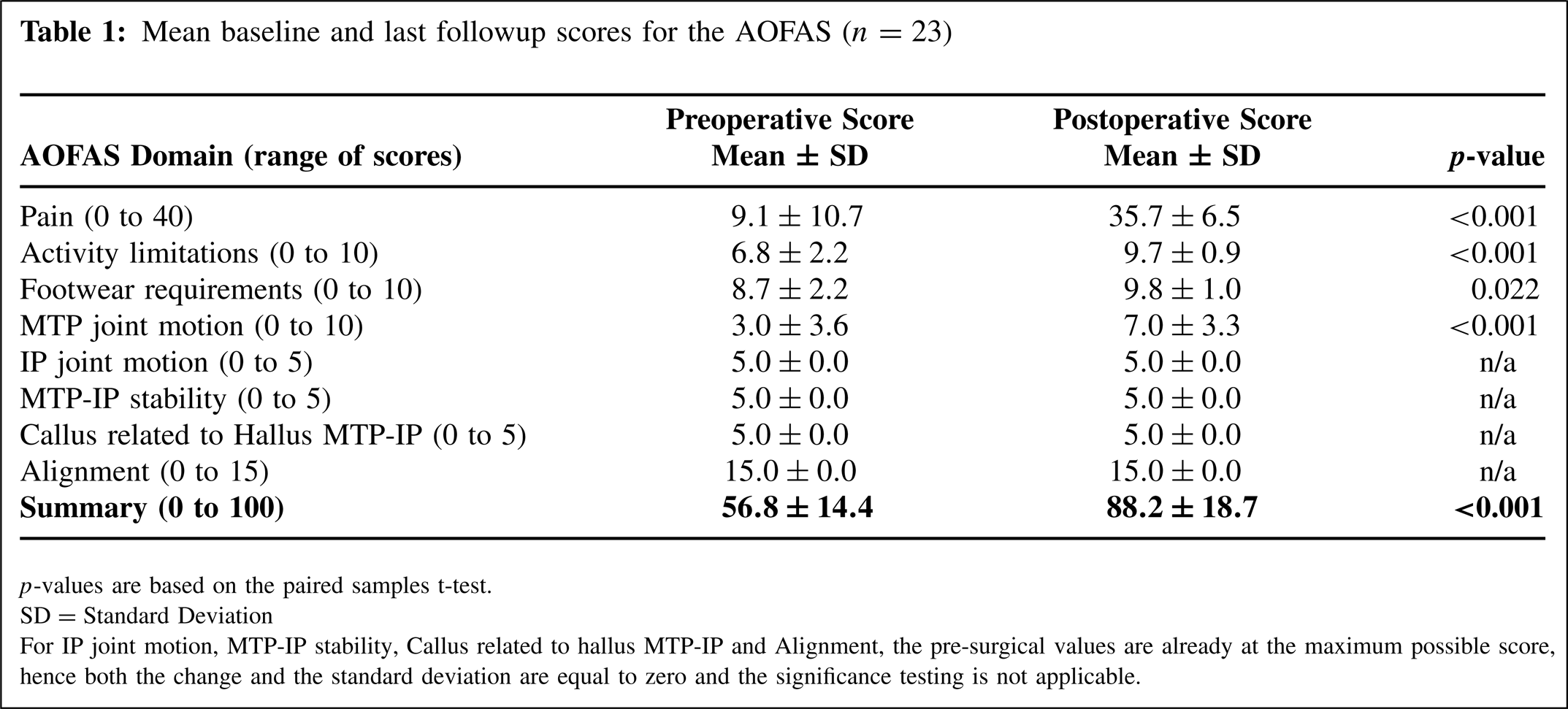
p-values are based on the paired samples t-test.
SD = Standard Deviation
For IP joint motion, MTP-IP stability, Callus related to hallus MTP-IP and Alignment, the pre-surgical values are already at the maximum possible score, hence both the change and the standard deviation are equal to zero and the significance testing is not applicable.
In the pain category, where no pain is 40 points and severe pain zero points, 2 patients moved from zero to only 20 at followup. One of those patients had poorly controlled gout and the other had developed osteoarthritic changes between the sesamoids and the head of the first metatarsal. Four patients who had generalized osteoarthropathy with Heberden's nodes prominently present on all fingers, moved from zero to 30 points on the pain scale at the last followup. While all followup x-rays showed no change in the position of the implants, no osteolysis and no changes in the cement layer, the x-rays of the patients with Heberden's nodes showed a higher tendency to the growth of new osteophytes (Figures 3 and 4).

Foot A-P radiographs showing preoperative hallux rigidus and 3 years postoperative followup in the same patient with the implant.

Lateral views of the same foot, preoperatively and postoperatively, 3 years.
The average patient age at the time of surgery was 53 (range, 35 to 70) years. All patients who were employed prior to surgery returned to their existing jobs in 2 to 4 weeks. These jobs included heavy labor, farming, secretarial work, check-out counter cashiering, and policing. Most patients in this series were retired. All younger patients returned to their former activities, which involved wearing work boots in several cases, but in one case, a requirement daily to run several miles.
All patients were educated for a return to normal patterns of walking, which required pressing the pad of the great toe onto the ground, unloading the outer border of the foot and turning the leg into neutral rotation.
As part of the followup, all patients were asked if they were satisfied with their surgery. Two patients were disappointed with the fact that they had not achieved normal movement in the first MTP joint. Nine patients said that they were “pleased” and 12 “very pleased” with the results of their surgery. Several women were particularly happy to be able to wear a variety of heel heights on their shoes. One patient, in a myocardial rehabilitation program, returned to prescribed daily ‘jogging,’ which, prior to implant surgery, foot pain had made impossible.
DISCUSSION
The hallux or great toe is padded and under strong muscular control to meet the requirements for normal walking and running. The plantar directed force it develops at ‘toe-off’ needs large, smooth cartilage covered surfaces for load transfer at the MTP joint. Damage to the surface cartilage by trauma or degeneration can initiate the biological processes of osteoarthritis. The ‘mechanical’ causes of joint degeneration listed by Camasta 6 include pes planovalgus leading to “hallux equinus,” a shift in the axis of motion at the first MTP joint and elevation of the first metatarsal.
Another ‘mechanical’ cause may be excessive pressure contact of the opposing joint surfaces near the dorsum of the joint. The reduced area of contact can damage cartilage as it does in hip dysplasia and in the malaligned knee.
The first MTP joint may be affected as part of a generalized osteoarthropathy of idiopathic or inflammatory type. The idiopathic type described by Kellgren and Moore, 26 for example, may not affect the alignment of the hallux unlike the destructive forms of gout and rheumatoid arthritis.
Osteophyte formation around the joint margins, mainly dorsal and lateral, can in itself, be symptomatic even when the cartilage is relatively well-preserved. Less common forms of degenerative arthritis, such as psoriatic arthropathy and hemochromatosis, can cause pain and stiffness of the first MTP joints. Although the smaller MTP joints are also affected, their involvement may not be as disabling.
Pain and restriction of joint movement are the main complaints. As the source of these symptoms is the inner side of the foot, loadbearing is transferred to the lateral metatarsal pads and the outer border of the foot. One patient in this series had fatigue fractures of the fifth metatarsals. Another adaptation to the rigidity of the first MTP joint is external rotation of the leg by heel pivot, to effectively shorten the antero-posterior length of the foot. Medial knee and hip pain can be a consequence.
Since the first description of HR by Lucy 34 and Davies-Colley 9 in 1887, measures have been sought to reduce the pain and the effects of joint stiffness. Conservative treatment used in early cases, consists of analgesics, anti-inflammatory drugs, and intra-articular injection of water-soluble cortisone. The mechanical remedies include shoes with Jones bars, rocker bottom soles, steel reinforced soles, and a variety of orthotics. While some of the conservative methods are successful in relieving the symptoms many patients seek more permanent solutions, which are often surgical.
Surgical treatment in some form or other has been performed since at least the time of W.L. Keller 25 and can provide subjective patient improvement. 17 Other surgical options include cheilectomy, osteotomy, joint resection, joint fusion, and joint replacement. Cheilectomy is applicable to the earliest cases where there is a good joint space and osteophytes that are particularly prominent. Although initial symptomatic improvement can be obtained from cheilectomy, there is, after an average of three years, deterioration in the range of motion and worsening progression of the radiological rating of arthritic degeneration, according to Mulier. 38 Feltham 13 claimed an AOFAS score of 80 in 53 cases at an average of 65 months after cheilectomy. Those over 60 were able to reach an AOFAS mean score of 89.
Lau and Daniels 30 reviewed 24 cheilectomy cases after an average of 2.1 years. They had a mean AOFAS score of 77.3. The percentage of a relatively young age patient group (average age, 51.9 years) that was satisfied was 87.5%. They found on pedobarographic analysis, decreased load under the great toe, but increased weight transfer to the lesser metartarsal heads. Coughlin and Shurnas 8 report on 80 patients (93 feet) who had cheilectomy. At an average followup of 9.5 years after cheilectomy, 92% had success in pain relief and function.
Osteotomy of the first metatarsal or proximal phalanx is designed to alter the alignment of these bones in the sagittal plane. The metatarsal, if elevated, is made more plantigrade and the proximal phalanx, with a dorsal wedge osteotomy, is upward angulated. Neither of these procedures alter the joint surface.
Southgate and Urry 43 did a retrospective review of 10 proximal phalanx osteotomies and 20 arthrodeses, for hallux rigidus. They compared osteotomy with the arthrodesis and found that a greater force occurred under the first metatarsal after osteotomy than after arthrodesis, but callosities were more common after arthrodesis.
Blyth and Mackay 4 recorded the results of 18 dorsal wedge phalangeal osteotomies in the treatment of HR. Good or excellent results were obtained in 14 cases with a mean followup time of 4 years. All patients were significantly improved with regard to pain, activity, problems with footwear, and range of motion.
Thomas and Smith 47 describe a dorsal wedge osteotomy of the proximal phalanx in conjunction with cheilectomy. The average age of the patients was 47 years. At followup, 58% of the patients had no pain and 42% only mild pain. All osteotomies united; however, 8 patients complained of restrictions in their choice of footwear.
Ronconi 40 reported on distal oblique osteotomy of the first metatarsal. Thirty osteotomies were performed on patients with a mean age of 54 years. After 21 months, 84% had ‘good to excellent’ results. There was improvement in the range of motion, but increased pressure on the second and third metatarsal heads. Roukis and Townley 41 describe a comparison of an endoprosthesis compared with periarticular osteostomy. The authors presented a short tem followup and analyzed the comparative results. Twenty patients (20 feet) had a periarticular osteotomy. Sixteen were seen for followup. Seven patients (9 feet) had a resurfacing endoprothesis. Stastistically significant differences between preoperative and postoperative values were found for the osteotomy group-for the metatarsal protrusion group (p = 0.000), transverse plane angulation of the second digit (p = 0.000) and lateral talo-first metatarsal angle (p = 0.015). No other significant differences for either group were found.
Since the first description by Keller in 1912, 25 resection of the proximal part of the proximal phalanx has been an easy and commonly performed operation. The patient, however, loses the big toe as a functional digit. Contracture of soft tissues may produce an ugly, displaced, uncontrollable, cosmetically unattractive, great toe. Reducing the amount of resected bone, risks continued pain and poor function. Resection of the metatarsal head is not recommended.
Barca 2 placed the rolled plantaris tendon at the base of the first phalanx in 12 cases. He claimed that after 21 months, there was improved motion and reduced pain.
Hamilton and Hubbard 22 felt that capsular interposition arthroplasty could give predictable pain relief in carefully selected individuals with severe (Grade III) hallux rigidus. They used minimal resection of the phalanx, and interposed the dorsal capsule and the extensor hallucis brevis tendon in the space created. However, approximately 30% of the patients undergoing the procedure experienced some degree of postoperative, transfer metatarsalgia and required an orthosis for sports.
Mroczek and Miller 37 used a modest metatarsal cheilectomy with an oblique resection of the phalanx base preserving the flexor hallucis brevis attachment combined with interposition arthroplasty of the dorsal joint capsule. They claim that such a modification produced a satisfactory outcome while maintaining plantar flexion power and the length of the toe. Miller and Maffulli 36 recommend interposition arthroplasty using the ipsilateral gracilis tendon for patients who do not want an arthrodesis. Kennedy et al. 27 report on 18 patients (21 feet) with severe joint cartilage loss, who had interpositional arthroplasty at an average age of 56 years and at a mean time of 38 months followup. All had relief of pain. The mean increase of range of motion was 37 degrees and followup AOFAS mean was 78.4. They had a 6% complication rate. Berlet et al. 3 used a minimally invasive soft tissue arthroplasty, inserting human acellular regenerative tissue matrix. They describe preliminary (mean, 10.1 months) results in 8 patients with an average age of 50.2 years. Treating Coughlin Grade 3 hallux rigidus they had no complications. The preoperation AOFAS score averaged 66.7 and 89.6 at followup.
Arthrodesing the first MTP joint is a popular form of surgical treatment with a good record of success in pain relief. It has, however, significant disadvantages. It does not address the problem of ‘rigidus,’ as it extends the stiff, medial ray of the foot to the interphalangeal joint. Arthrodesis is unlikely to solve the altered gait pattern of external leg rotation on heel pivot. Fusion ideally requires a set angle of 15 degrees dorsiflexion and 5 to 10 degrees of valgus. Fusion may not appeal to women who wear high heels or to runners. There is an incidence of non-union and the risk of increased load transfer to other metatarsal heads. A number of jobs require workers to kneel or squat in positions that require toe dorsiflexion. With first MTP joint fusion, the interphalangeal joint may become hyper-extended.
In a clinical study, Lombardi 32 followed 21 cases, treated by arthrodesis, for an average of 28 months. The AOFAS scores rose from 39 to 75. In a radiographic study, Lombardi et al. 33 found that fixed dorsiflexion of the hallux caused plantar flexion of the first ray and an increase in the height of medial longitudinal arch. Lauge-Pedersen 31 has shown that, in a small series of patients, it is possible to achieve bony fusion of the first MTP joint in patients with HR using a minimally invasive percutaneous technique. The author did not, however, comment on the rate of fusion.
DeFrino et al. 10 studied 10 feet in 9 patients with severe HR. Arthrodesis of the first MTP joint was assessed with the AOFAS hallux score, by radiography and by dynamic pedobarography. After 34 months on average, all preoperative tests were repeated and gait analysed. Their patients showed subjectively a significant clinical improvement. The mean AOFAS score improved from 38 to 90 and the pedobarographic analysis demonstrated restoration of weight bearing on the first ray with greater maximum force carried by the toe pad at toe-off. However, kinematic data indicated a significantly shorter step length with some loss of ankle plantar flexion at toe-off on the fused side. The kinematic data indicated a reduction in both ankle torque and ankle power at push off. Nonetheless, there was effective pain relief and a high level of patient satisfaction. Ettl et al. 12 reviewed 34 arthrodesis patients. They had a good functional result but only achieved an AOFAS score of mean 53. Taylor et al. 46 favor arthrodesis and post good results. Forty-three of their patients (54 feet) had arthrodesis. At a mean followup time of 21.7 months, 30 patients (88.2%) rated their results as excellent or good. Four (11.8%) rated their result as poor. Internal fixation devices were removed from 5 feet. Gibson and Thomson 18 found, in a randomized controlled trial, fusion superior to total joint replacement. Sixty-three patients, ages ranging from 34 to 77 years, were randomly assigned to arthrodesis (38 toes) or arthroplasty (39 toes). At the 24 months followup, while pain improved in both groups, it was greater after arthrodesis (p < 0.01). Six arthroplasty implants loosened and had to be removed.
It is interesting that Anderson 1 found that HR alone, not surgically fused, could cause atrophy of calf muscles. He found 17 patients with HR out of 1,000 consecutive patients in a general rheumatology practice, who had less than 30 degrees of dorsiflexion at the first MTP joint compared with 60 degrees on the unaffected side. Each one of these patients had between 1 and 2.5 cm of atrophy of the affected calf measured at a point 15 cm below the insertion of the patellar tendon. None of these patients had great toe pain as their primary symptom. Twenty-five control patients were examined by the same technique and none had a difference in circumference between the two sides of more than 0.5 cm. This observation suggests that there is loss of muscle bulk in the calf when the great toe is unable to move at the MTP joint. Hall and Nestor 21 using a stiff insole in 20 normal individuals, noted altered sagittal plane kinematics at the ankle, knee and hip when the first metatarsophalangeal joint had restricted dorsiflexion. As noted earlier, DeFrino et al. 10 found similar alteration in kinematics at the ankle after fusion of the first MTP joint. Their kinetic data indicated a reduction in both ankle torque and ankle power at push-off.
Other concerns about fusion include the requirement after surgery to wear a cast on the foot for 4 to 6 weeks with protected weight bearing or confinement to a wheelchair, for the elderly, if they are not able to use crutches or walkers. Other concerns are for non-union and less than ideal position of the fusion.
A metal hemiarthroplasty, ‘BIOPRO’ has been in use since 1952. Its use was reported-on by Townley and Taranow 48 in 1994. Silastic hemiarthroplasty was commonly used, associated with cheilectomy, from the late 1960's until all silastic implants became controversial in 1995. The toe implants worked well initially but had a tendency to break down and produce a local immune response. McNearney 35 describes inguinal lymph node foreign body granulomas after placement of a silicon rubber implant in the first metatarsophalangeal joint.
Brage and Ball 5 while supporting fusion, note the value of a metallic hemiarthroplasty, in its ability to allow restoration of alignment and maintenance of motion, length and strength in the great toe, which they consider to be fundamental in attaining a good clinical result. Giza and Sullivan 19 describe the results of 103 hemiarhroplasties over a period of 4 years. Stiffness was the most common problem. The authors suggest 51 degrees of dorsiflexion is needed for normal gait.
Total arthroplasty for the first MTP joint was described by Ess. 11 Ten patients with hallux rigidus who were treated using the ReFlexion endoprosthesis were followed. At 2 years, the AOFAS scoring system rated 5 excellent, 1 good, and 4 fair or poor. While flexion and extension improved, three patients' implants became malaligned. One uncemented, phalangeal component became loose. The author concluded that this implant should not be used for athletes and young people. Fuhrmann et al. 15 were cautious with total arthroplasty over the stability of the joint and radiolucent lines around components.
Kundert et al. 29 report on their results with a modular hemi- or total arthroplasty. Between 1998 and 2004 the authors performed 47 replacements, 13 hemiarthroplasties, and 34 total arthroplasties. Fourteen of their patients with at least 36-months followup were analyzed. Three had to be revised and were excluded from followup. Eleven cases reached a mean followup time of 4 years. The overall mean Shankar score was excellent. There was a limited range of motion in 3 HP and 4 TP's. The authors quote an unpublished trial of 55 Toefit-Plus arthroplasties that revealed problems of distal loosening and bone fissuring in 12%. Fuhrmann 16 published a mid-term (39 months) followup of a 3-component total arthroplasty (ReFlexion). Radiolucent lines were seen around 25% of the phalangeal and 10% of the metatarsal components (cemented) but that did not impair the clinical results.
The results of the cobalt-chrome Trihedron hemiarthroplasty in this clinical series have been very satisfactory. The implant has provided relief of pain and stiffness in patients suffering from the effects of HR. The bearing surface of the implant follows the geometry of the original phalangeal surface. All patients had relief of pain, although mild, occasional discomfort remained in 5 patients. Joint stability (AOFAS 5), correct alignment (AOFAS 15), and full muscle strength (AOFAS 5) were achieved with one exception, a patient with pre-arthroplasty hallux valgus, who later required hallux valgus correction. With one exception, all patients had increased movement in the MTP joint although a normal range may not have been achieved. The AOFAS mean range of motion was 3 before hemiarthroplasty and at followup it was 7(p < 0.001). The reasons for the less-than-normal movement in 2 instances were related to prior surgery on the first MTP joint with significant scarring. One patient with hemochromatosis had a total range of motion of 20 degrees pre-surgery. The range improved in the early postoperative years but reverted to 20 degrees by final followup. Patients with large Heberden's nodes had difficulty in achieving a normal range of motion and tended to show very minor recurrence of osteophyte formation on the metatarsal head. The patients in this series were able to return to a normal gait and choice of heel height. Running was possible in those who chose to do it. Most of the patients were retired but those still working returned to their original occupations within two to four weeks after surgery. There has been no evidence of loosening of the components at an average of over 5-years followup. Strict adherence to isolating the wound area from the rest of the foot, peri-operative antibiotics and postsurgical local anesthesia, avoided wound infections.
CONCLUSION
In view of the disadvantages of some surgical procedures for the treatment of HR (such as cheilectomies, resections, osteotomies and arthrodeses), a morphometrically correct, cobalt-chrome hemiarthroplasty seems a safe and effective alternative.